
Abstract
Background and Purpose:
Over the last 50 years, chemolysis as a primary or adjuvant treatment for urinary stones has fallen in and out of favor. We review the literature for a historical perspective on the origins and chronology of Renacidin therapy, focusing on landmark studies and impracticalities that have seemingly condemned it to history.
Materials and Methods:
A MEDLINE search was performed on the topic of chemolysis of urinary calculi. Historical literature was reviewed with regard to stone composition, treatment modalities, outcomes, and complications.
Results:
A total of 61 articles were reviewed, 40 of which were case series, representing a total of 817 patients studied. Mulvaney first introduced Renacidin in 1959 as a modification of Suby and Albright's 1943 solution. Because of an overabundance of nonstandardized irrigation protocols, six deaths were reported in the early 1960s resulting in a Food and Drug Administration ban on the practice of upper urinary tract stone dissolution. Over time, Renacidin returned to the urologist's arsenal, appearing first as an adjunct to dissolve catheter and bladder calculi and later (1990) as an approved agent for renal pelvis and ureter use. This feat was almost single-handedly the result of a successful hemiacidrin case series published in 1971 by Nemoy and Stamey. By using daily urine cultures, prophylactic antibiotics, and meticulous intrarenal pressure monitoring, Nemoy and Stamey virtually eliminated all major irrigation complications, paving the way for a flurry of studies. More importantly, they established the link between residual struvite stones, persistent infection, and recurrent staghorn stone formation.
Conclusions:
Dissolution of urinary calculi by chemolysis has been shown to be safe and effective if performed with sterile urine cultures, prophylactic antibiotics, and low intrapelvic pressures. The pioneers of this therapy are remembered for their attempts to develop an alternative to open surgery, and, in the process, solidified the “stone-free” concept for infection-based stones.
Introduction
“In the future, it is likely that irrigations of the urinary tract with various solutions designed to dissolve stones will be an important part of the practice of urology.”
“Any urologist who treats stone disease should be familiar with the fundamentals of chemolysis and its potential role in the management of urinary calculi.”
The closest realization of dissolving stones came in the form of a solution called Renacidin (10% hemiacidrin). The triumphs, catastrophes, and controversy that surrounded Renacidin's use and seeming downfall will be chronicled in this review. In the peak of its popularity, Renacidin was being used to achieve stone-free status in recurrent struvite stone formers as a means of eradicating bacterial infection, a concept that is still relevant today. Although it is impossible to fully catalog 60 years of Renacidin's history, the novelty of its use in urology deserves mention and gives perspective for potential future therapies in the endourologists' armamentarium.
Materials and Methods
Relevant studies were searched from electronic databases including Cochrane Central Register of Controlled Trials (The Cochrane Library), MEDLINE, and EMBASE. Reference lists were also made from urology and nephrology textbooks and review articles. An on-line Google search was also used to identify legal documents and other pertinent materials. Search terms included all forms and abbreviations of renacidin, hemiacidrin, chemolysis, dissolution, urologic solution G, Suby's solution, ethylenediaminetetraacetic acid, and Guardian Chemical Corporation.
A total of 61 papers were reviewed. Of these, 21 were identified as basic science inquiries, case reports, or lower urinary tract investigations. The remaining 40 focused primarily on upper urinary tract stones, totaling 817 patients. All 40 upper tract stone studies were case series. Prospective clinical trials or cohort studies were not identified nor were any detailed Renacidin protocols before 1971. No data were present on patient selection criteria in these case series, and clear-cut variables (irrigation time, length of stay in hospital, stone analysis, etc.) were often lacking. From these 40 papers, 15 were chosen to be presented in tabular form.
The Beginning of Dissolution
The first reported case of stone dissolution was by Crowell 4 in 1924. Using a primitive retrograde catheter, Crowell methodically filled a young cystine stone former's renal pelvis with an alkaline antiseptic lavage of mercurochrome every other day. Along with oral sodium bicarbonate for urinary alkalinization, Crowell repeated these weekly lavages for a total of 10 months until the roentgenogram was clear of stones. After this success, Hellstrom 5 (1938) used 1% phosphoric acid with a mixture of boric acid and potassium permanganate to acidify alkaline salts associated with Staphylococcus-associated lithiasis.
A year later, Albright and coworkers 6 dissolved human calcium phosphate bladder stones using isotonic citrate solutions (pH=4.0). 6 This acidic solution, however, caused painful mucosal bleeding for the patient, so a rabbit model was developed to study dissolution speed using decalcified teeth. Their work culminated in 1943, when Drs. Suby and Albright 7 reported a reduction in bladder mucosal irritation and bleeding by adding magnesium to the citric acid solution (Table 1). 7 This product (isotonic citrate, magnesium oxide, and sodium carbonate) became known as urologic solution G or Suby solution (Table 2). 7 Although effective, the use of this solution was soon to be overshadowed by the establishment of Renacidin.
Before the 1970s, all percutaneous nephrostomy tubes were placed open or at the time of open lithotomy.
PNT=percutaneous nephrostomy tube; UC=ureteral catheter; CaP=calcium phosphate; NR=not recorded; SPT=suprapubic tube; EDTA=ethylenediaminetetraacetic acid.
Development and Introduction of Hemiacidrin (Renacidin)
In 1955, Guardian Chemical Corporation began manufacturing a liquid product to dissolve calcium deposits that frequently clogged milk pasteurizing equipment and tubing. In 1957, Dr. William P. Mulvaney (urologist at the University of Cincinnati) approached Dr. Alfred E. Globus (founder of Guardian Co. and biochemist who developed the solution) and suggested that the product may be useful in dissolving urinary catheter calcium deposits and encrustation.
After the product was renamed Renacidin, Dr. Mulvaney presented his preliminary data at the 1957 American Urological Association meeting. The solution itself was similar in pH and buffering capacity to the Suby G solution but contained malonic and gluconic acids (Table 2). The protons of these acids were believed to complex with phosphate (phosphoric acid) and calcium (calcium citrate) to form soluble compounds at a pH of 4.0. Because struvite stone solubility increased at pH <5.5, Dr. Mulvaney believed Renacidin would be useful in dissolving struvite stones. For commercial purposes, Guardian began producing the product in powder form, where 100 g Renacidin could be reconstituted in 1000 mL distilled water. Once in solution, Renacidin was stable for long periods and could be autoclaved or boiled without losing its potency. 8
In 1959, Dr. Mulvaney published the first study describing the in vitro properties of Renacidin (10% hemiacidrin) on 50 human calculi as well as in three human case reports. 9 He and his colleagues found that Renacidin sequestered 400% more mineral than any single organic acid alone, such as citric acid. 10 They thought that the added magnesium salts (roughly four times the elemental magnesium of the Suby G, Table 2) provided ion exchange with stone calcium and enhanced dissolution with the added benefit of decreased mucosal irritation. 9,11 –14 It appeared to act as an excellent solvent for calcium phosphate, calcium carbonate, and magnesium ammonium phosphate stones. Cholesterol, uric acid, and calcium oxalate stones, however, were relatively insoluble to Renacidin.
Their “proof of concept” experiment was a small case series of three patients who had significant kidney and bladder stones along with catheter encrustation. Despite a reported 100% success rate (Table 1), this series was limited by lack of stone composition, follow-up data, and the need for indefinite daily 10% hemiacidrin catheter irrigation to ensure removal of calcifications. 9,10
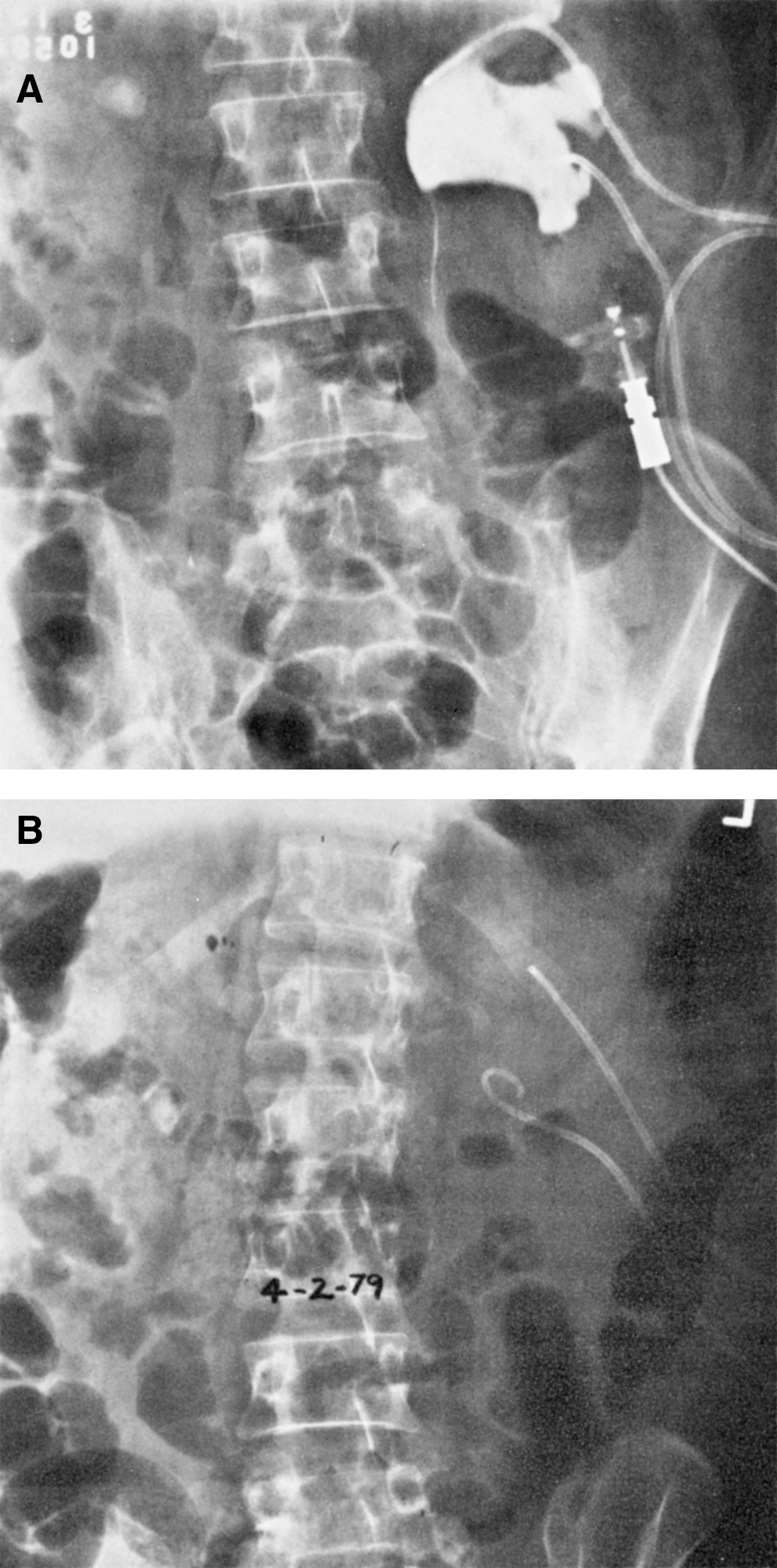
Based on Dr. Mulvaney's initial reports, several large case series with modest results were published using Renacidin irrigations to treat catheter encrustation and a variety of renal and bladder stones compositions, not just struvite (Table 1). 8,13,15 –20 This increase in clinical use also unveiled some limitations. First, because Renacidin solution contained high levels of magnesium and phosphate, its use was contraindicated in patients with advanced renal disease (creatinine clearance <10 mL/min). 21 –27 Second, as if foreshadowing future catastrophies, Mulvaney reported in 1960 that debris and sand tended to obstruct single ureteral catheters, resulting in patient discomfort and obstruction. 15 Years later, the development of percutaneous nephrostomy puncture techniques would lead to improved irrigation and drainage (Fig. 1). 28
In the early 1960s, however, haphazard Renacidin delivery protocols through ureteral catheters were associated with six patient deaths that would take Renacidin almost 30 years to surmount. 29,30
Banned by the Food and Drug Administration (FDA)
The safety of Renacidin irrigation first came into question when Kohler 30 reported a patient mortality during irrigation use. He described postmortem renal infarction, necrosis, and purulent kidney infection in a stone patient with high inflow pressures over 80 mm Hg during Renacidin irrigation therapy. Fostvedt and Barnes 29 added four cases of sudden death from suspected pyelovenous backflow with postmortem findings ranging from papillary necrosis to cerebral edema. 29 Finally, Auerbach and associates 31 followed with a case of severe pyelonephritis, ureteritis, and chemical pyelitis in a patient with bilateral renal calculi. The patient's ultimate cause of death was ruled pulmonary embolus, but the striking renal findings were attributed to Renacidin. 31
Based on these six deaths, on June 13, 1963, the FDA banned the use of Renacidin irrigation for the upper urinary tract and bladder. 28,32 The FDA acknowledged that inconsistencies in protocols and user mistakes likely led to the Renacidin mortalities and pointed to sepsis, rather than direct toxicity of the agent, as the cause of death in all cases. Not surprisingly, Mulvaney came out in defense of the solution, attributing the deaths to obstructed ureteral catheters leading to increased intrapelvic pressures and sepsis. He pointed to the safety of the procedure at renal pressures below 24 to 30 cm H20 and even advocated adding neomycin directly to the solution to prevent infectious complications. 19 The intrapelvic pressures he described were subsequently validated by other investigators to be high enough for stone fragmentation but low enough to minimize pyelovenous backflow. 33 Finally, Mulvaney noted that most adverse events seemed to occur at night when nursing care was scarce, and his safety frustrations were echoed by multiple other authors. 3,8,17,23,34
Based on Mulvaney's comments, on August 8, 1963, less than 2 months after their first decision, the FDA approved Renacidin to “prevent formation of and to dissolve calcifications in catheters in the urinary bladder.” Interestingly, the ruling on the upper urinary tract remained in place until October 1990, when Renacidin was approved as an “orphan drug” for the treatment of renal and bladder calculi of the apatite or struvite variety (United-Guardian Inc., U.S. patent #4,962,208). The term orphan drug refers to a drug or biologic intended for use in a rare disease or condition (defined as affecting fewer than 200,000 Americans) whose sponsor receives certain governmental benefits in exchange for drug development. Therefore, for almost 30 years, Renacidin's use in the upper tract was classified as investigational and needed informed patient consent, approval by a hospital human ethics committee, and occasionally permission from the FDA. 18,35 Undoubtedly, this drug would have retreated into history had it not been for two advocating urologists and a new protocol.
New Life for Renacidin
In 1971, Nemoy and Stamey 14 published a landmark article on the adjuvant use of Renacidin through percutaneous nephrostomy tubes (PNT) after open pyelolithotomy in patients harboring infectious stones, specifically Proteus mirabilis and Klebsiella. 14 More than any previous dissolution article, Nemoy and Stamey highlighted the concept of a formal protocol for dissolution therapy in the setting of infectious stones after open stone surgery (Table 3). First, they outlined absolute contraindications to Renacidin, including infected urine, fever, or persistent flank discomfort. Their pre-surgical guidelines emphasized daily urine cultures for proper antibacterial selection and confirmation of sterility before surgery or irrigation. 14
UTI=urinary tract infection; IVP=intravenous pyelography.
During open surgery, the renal pelvis and collecting system were irrigated copiously with saline to flush out stone fragments. Renacidin irrigation began on the fourth or fifth postoperative day with saline irrigation to test for complete healing of the pyelotomy incision. If no leakage, fever, or flank discomfort occurred, 10% Renacidin was then started at 120 ml/h through a nephrostomy tube. Once there was absence of visible particles on tomography, the irrigations would cease after an additional 24 to 48 hours. Interestingly, they even allowed patients to have control over their irrigations by instructing them on “… how to disconnect the inflow tube at the first sign of flank discomfort, even before notifying the nurse. This important precaution allows immediate reduction of intrarenal pressure in the presence of temporary outflow obstruction.” 14
In response to the controversy surrounding Renacidin-associated deaths, Nemoy and Stamey reasoned they were secondary to pyelovenous backflow of untreated urinary tract infections and stated, “It is abundantly clear from these reports that if the physician is unwilling to assume responsibility for a sterile renal urine prior to and during irrigation … he should not attempt dissolution of infection stones.” 14
With safe and effective protocols in place, clinical applications for Renacidin irrigation and struvite stones intensified (Fig. 2). During the next 15 years (1973 to 1988), Renacidin reached its pinnacle of publications with its use described through PNT after open lithotomy, through ureteral catheters for chronically ill or spinal cord injury patients, and even as primary therapy through fluoroscopic PNT techniques (Table 4). 3,33,35 –38 Many of these investigators also contributed refinements to the protocol, such as irrigating for an additional 48 hours after radiography has shown disappearance of stones or halting irrigation altogether if a week of treatment did not result in a 50% reduction in size. 3,33,36 –38
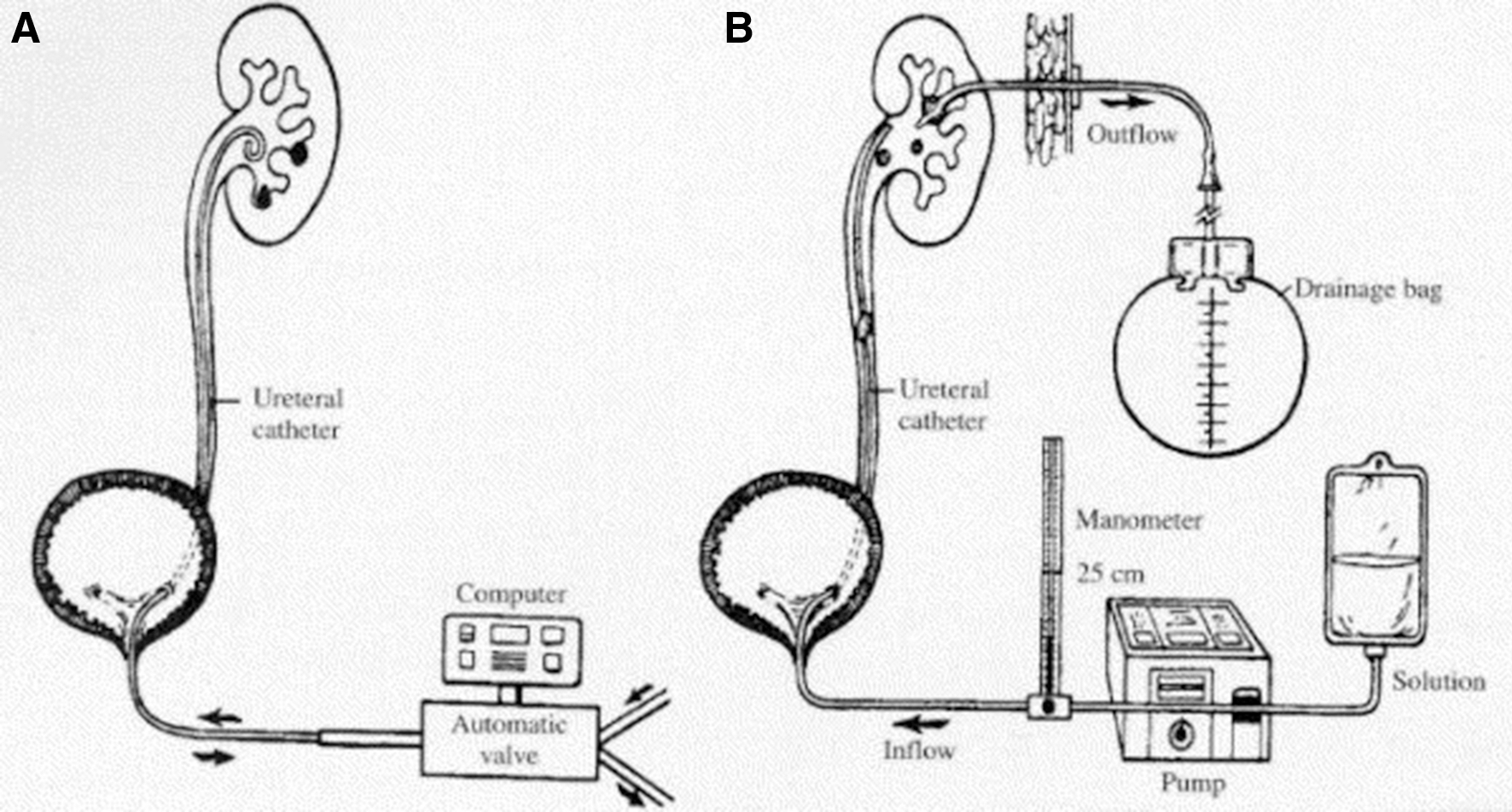
Irrigation equipment configurations for direct chemolysis I.
PNT=percutaneous nephrostomy tube; UTI=urinary tract infection; OL=open lithotomy; UC=ureteral catheter; NR=not recorded; MIS=minimally invasive surgery; SWL=shockwave lithotripsy.
More than their attention to dissolution safety, Nemoy and Stamey 14 are credited with observing the relationship between small residual stones, incomplete infection eradication, and high struvite recurrence rate. They theorized that urea-splitting organisms were deeply embedded within struvite stones, protecting them from the action of antibacterial agents. Unlike many others, they stated that small stones could lead to persistent infection and stone recurrence and strongly advocated for complete stone-free results after pyelolithotomy for struvite stones. 39 Silverman and Stamey 40 went on to prove the theory by placing 46 struvite stone patients with bacteriuria on a “total therapeutic program.” (Table 4) After open surgical debulking and culture-sensitive antimicrobial therapy, they placed all patients on adjuvant dissolution therapy with Renacidin through a Hemovac tube for at least 48 hours or until stone fragments were dissolved. With years more follow-up than any other series, Stamey boasted a 2.5% stone recurrence rate while his peers at that time reported stone recurrences of 30% in 6 years. 41 Stamey concluded that “… the urologist has no choice but to use Renacidin in the kidney when residual struvite or apatite fragments are left in the kidney postoperatively.”
Declining Popularity
Even in light of Nemoy and Stamey's protocols, the shortcomings of Renacidin seemed to outweigh its advantages (Table 5). First, stone analysis was necessary for the proper selection of the irrigant, and this was not always available. Second, vigilance in maintaining flow and proper equipment was frustrating. Constant nursing care was needed for most patients, and placement of additional ureteral catheters or PNT was needed if obstruction occurred. The protocols were labor intensive, necessitating prolonged antibiotics, daily urine cultures, serum magnesium levels, biweekly radiography, and complete absence of fever or pain. Deep venous thrombosis prophylaxis was considered mandatory because of patient immobility during therapy. 28,31,42 In 1979, Dretler and colleagues 28 (Table 4) chronicled these concerns by reporting frequent irrigation cessations for elevated intrapelvic pressures, repeated fluoroscopy trips to radiology, and psychologically taxing lengths of immobility and hospitalization in patients on Renacidin irrigation.
With the introduction of percutaneous nephrolithotomy (PCNL) in 1976 43 and shockwave lithotripsy (SWL) in 1980, 44 the era of minimally invasive surgery (MIS) for stone disease began. Urologists were eager to learn new procedures that reduced patient morbidity and, most importantly, were not banned by the FDA. As MIS popularity expanded, Renacidin began to be used in an adjuvant setting. Spirnak and coworkers 45 described an 80% stone-free rate when Renacidin was combined with SWL in a group of patients with complex struvite stones. Palmer and colleagues 46 detailed a group of patients who completed months of daily outpatient renacidin irrigations through a PNT after PCNL or SWL with only three patients needing inpatient hospital admission during 365 total outpatient days (Table 4). Although they reported total outpatient daily cost equal to that of one hospital day stay, several others documented that adjuvant Renacidin added 11 days to hospital stay and up to 3 months of outpatient therapy. 3,30,33
In October 1990, the ban on Renacidin's upper tract use was lifted, but it was too little, too late. Since 1990, only 20 Renacidin articles have been published, and most of these are in vitro studies. The era of managed care and cost containment did to Renacidin what a 30-year FDA ban could not. Perhaps Rodman 47 was right when he wrote these sentiments, “One has to wonder whether the advent of managed care and the consequent emphasis on shortening hospital stays did not adversely affect the management of struvite stone disease.”
Renacidin is not completely gone. United-Guardian Inc. continues to report annual Renacidin U.S. sales from $1.2 to 1.5 million, primarily from lower urinary and catheter irrigation use. As recent as Medicare contract year 2010, Renacidin has a Healthcare Common Procedure Coding System code and continues to be listed in the Federal Register as a paid outpatient service to Medicare beneficiaries. Certainly, stone dissolution by Renacidin is not a panacea, and discretion must be exercised when considering its use. After reviewing the literature, Renacidin appears to be a valuable addition to the urologic armamentarium if used within its narrow clinical setting and with cautious vigilance.
Conclusions
Renacidin has had a complex history marked with promise and frustration. Although it survived an FDA ban, it could not survive the era of MIS, cost containment, and managed care. Renacidin will be remembered as a novel therapy for patients who were poor surgical candidates and made headway in struvite stone formers, sparing them morbidity and stone recurrence after primary surgical interventions. For patients with colonized urinary tracts and infectious stones, postoperative and prophylactic irrigations with Renacidin were shown to eliminate the nidus for recurrent infection and serve as a potential long-lasting cure. This, at least in theory, should be considered when its higher healthcare costs are discussed.
The importance of Renacidin in the discovery and achievement of stone-free status for the infected stone patient cannot be overstated. Patients with complex struvite stone disease who are not cured by stone removal alone still exist. In these patients, it may be time to reconsider the role of Renacidin irrigation therapy.
Footnotes
Disclosure Statement
No competing financial interests exist. Funding for this study was obtained through grant R01 DK061666-06 (Canales).