
Abstract
We demonstrate a safe and reproducible technique for laparoscopic port-site closure. First, we use hemostatic tonsil forceps to deliver a 0-polyglactin suture into the abdomen via a puncture through the rectus fascia parallel to the fascia defect under visual guidance. Second, we perform a similar puncture with the tonsil forceps on the opposite side of the fascia defect under direct vision to grasp the suture. This cost-effective maneuver is safe and eliminates the need for ancillary port-site closure devices.
Introduction
Laparoscopic port-site closure devices and bioabsorbable hernia plugs have been developed to prevent incisional port-site hernias and to lessen the difficulty often encountered with closing the fascia defects. 3 These devices obviously increase the instrument cost for the case with the purported benefit of reducing this devastating complication.
We report a novel technique that eliminates the need for additional port-site closure devices. The described technique is safe, simple, reproducible, and cost-effective.
Technique
We close all 10-mm and 12-mm port sites in our adult laparoscopic and robot-assisted cases. First, with simple pressure, we use hemostatic tonsil forceps to deliver a 0-polyglactin suture into the abdomen via a puncture through the rectus fascia parallel to the fascia defect under visual guidance (Fig. 1). Second, we perform a similar puncture with the tonsil forceps on the opposite side of the fascia defect under direct vision to grasp the suture (Figs. 2 and 3). Pneumoperitoneum can be maintained by leaving the port in place during the delivery of the suture. Furthermore, pneumoperitoneum is often not an issue during hand-assisted laparoscopic cases because the punctures and suture can be grasped with ease and little loss of pneumoperitoneum before closure of the port site. Last, the defect from delivery of the suture has not resulted in significant bleeding from the port site, and there is no loss of pneumoperitoneum from the tonsil site defect.
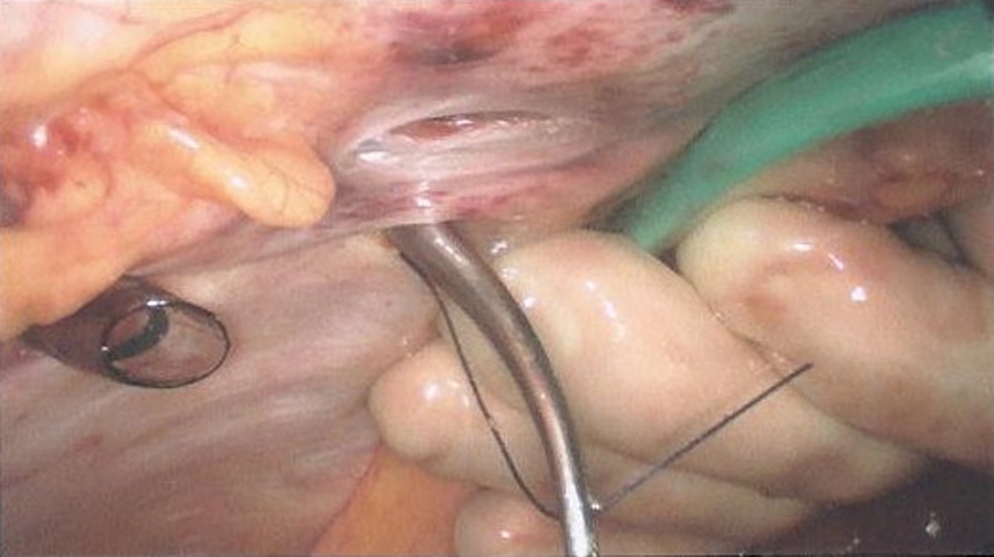
The patient underwent laparoscopic hand-assisted left radical nephrectomy. Hemostatic tonsil forceps were used to deliver a 0-polyglactin suture into the abdomen via a puncture through the rectus fascia parallel to the fascia defect under visual guidance to facilitate port-site closure.
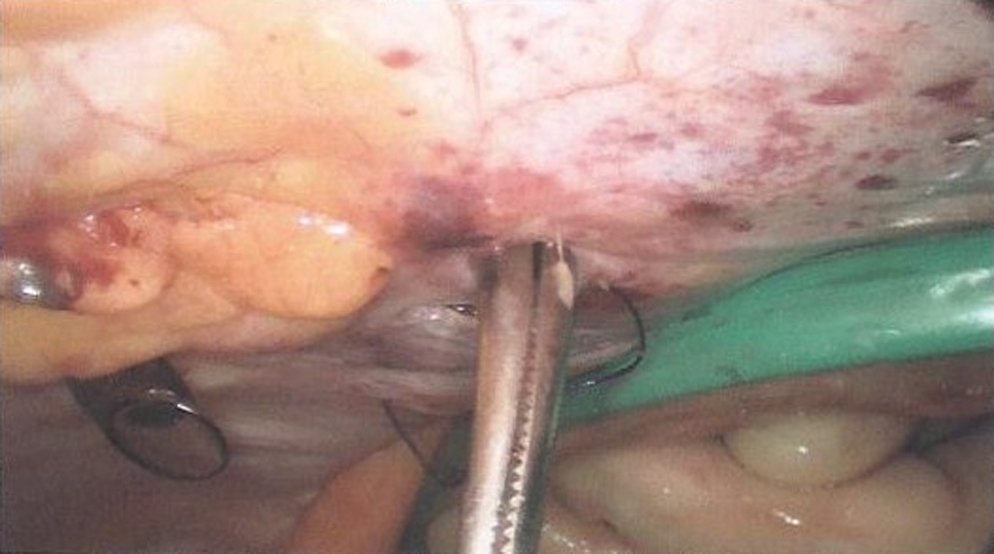
A similar puncture with the tonsil forceps on the opposite side of the fascia defect under direct vision to grasp the suture.

Endoscopic view of fascia closure.
This cost-effective maneuver is safe and eliminates the need for ancillary port-site closure devices. The remaining camera or hand assistant ports are used for specimen extraction and closed under direct vision.
Discussion
Various types of laparoscopic port-site closure devices have been developed to prevent incisional port-site hernias and to lessen the difficulty often encountered with closing fascial defects. There are generally three separate groups of closure devices available that include (1) intracorporeal closure under direct vision, (2) extracorporeal under direct vision, and (3) use of tactile sense when desufflation is performed. 4
An example of the first group includes the Endoclose (Tyco Auto Suture International, Inc, Norwalk, CT) spring-loaded suture carrier loaded with a suture that is introduced into the abdomen between the edge of the skin and the port. The suture is released, and the device is then passed through the opposite fascia defect, suture loaded with another instrument, suture grasped, and the device/suture are brought out of the abdomen. 5
An example of the second group is the Carter-Thomason device (Inlet Medical, Inc, Eden Prairie, MN) that consists of two parts: The Pilot Guide and the Carter-Thomason suture passer. 4 The technique involves insertion of the Pilot Guide into the fascial defect accompanied by pinholes for insertion of the Carter-Thomason suture passer to close the defect. 5,6
The straight, closed Lowsley retractor (Circon ACMI, Stamford, CT, USA) is an example of the last group of port closure devices and techniques in which the retractor is passed through a 12-mm port into the abdomen. The blades of the Lowsley retractor are then opened, port removed along the shaft of the retractor with the retractor, and port pulled upward to facilitate standard hand-sutured closure. 4,5
The simple maneuver we describe has enabled us to eliminate the need for laparoscopic closure devices for this critical step of the operation and reduce additional instrument costs. Furthermore, the technique described could be used in a situation in which the surgeon uses a Carter-Thomason device and the device malfunctions and/or becomes contaminated without a replacement available. The cost of the above technique vs the Carter-Thomason device is significantly lower. The retail price of a polyglactin suture is $4.22, while the Carter-Thomason device retails for $115.50, not including the suture cost. If you include the suture cost for both techniques, the final cost savings using the alternative technique vs the Carter-Thomason device is $115.50.
Complications may range from port-site bleeding, bowel or other intra-abdominal organ/vessel injury, as well as port-site hernia as described with use of other laparoscopic port-site closure devices. 3 In our experience, with direct visualization and meticulous control of suture delivery, we think our technique minimizes complications with a blunt-ended instrument.
Footnotes
Disclosure Statement
No competing financial interests exist.