
Abstract
Background and Purpose:
Ureteral stents are a fundamental part of many urologic procedures. Serious complications, including migration, fragmentation, and stone formation, still occur, especially when stents have been forgotten for a long time. No widespread consensus for the type or indwelling time to avoid ureteral stent complications has been reached, however. We investigated the correlation between the indwelling time and encrustation, incrustation, coloration, and resistance to removal.
Patients and Methods:
A total of 330 ureteral stents in 181 patients were examined.
Results:
Overall, 155 (47.0%) stents were encrusted, and the encrustation rate was 26.8% at less than 6 weeks, 56.9% at 6 to 12 weeks, and 75.9% at more than 12 weeks. A total of 46 (13.9%) stents resisted removal, and 3 of these could not be removed by cystoscopy. The median indwelling time was 72 (14–124) days for stents that resisted removal and 31 (30–60) days for irremovable stents. The frequency of encrustation with coloration was higher than that without coloration in the period of less than 6 weeks and the period between 6 to 12 weeks of indwelling time.
Conclusions:
In our study, although ureteral stent encrustation was related to the indwelling time, heavily encrusted ureteral stents necessitating additional procedures for removal occurred within an indwelling time of 3 months. The exact interval for removal of an indwelling ureteral stent to avoid additional procedures for removal is therefore difficult to determine.
Introduction
Serious complications, including migration, fragmentation, and stone formation, still occur, especially when stents have been forgotten for a long time. 2 –5 No widespread guidelines exist, however, for the management of these potentially serious problems. 6 The incidence of encrustation has been shown to increase with the duration that the stent remains indwelling. 7 Because stents are continually improved, such as occurred after the development of hydrophilic coating, the actual etiology of encrustation is unclear, 6 and, to the best of our knowledge, there have been no detailed examinations of the optimal indwelling time.
We investigated the correlation between the indwelling time and encrustation, incrustation, coloration, and resistance to removal in 330 ureteral stents.
Patients and Methods
A total of 330 ureteral stents in 181 patients were investigated in our department between June 2010 and February 2011. Informed consent was obtained from all patients. Ureteral stents were removed using topical, conscious sedation, and general anesthesia with or without epidural anesthesia for the various procedures, including stent removal, before/after shockwave lithotripsy (SWL), before/after ureteroscopy (URS), and before/after percutaneous nephrolithotomy (PCNL). After removal, all stents were examined for the location and severity of stent encrustation, incrustation (endoluminal crustation), and coloration. At the time of removal, we also examined the resistance to removal.
The level of encrustation was divided in two grades (severe/moderate) at each site as shown in Figure 1. The levels of encrustations were determined by at least two urologists. A total of four urologists determined the grade of encrustations, and all urologists agreed with the same definition of encrustation.
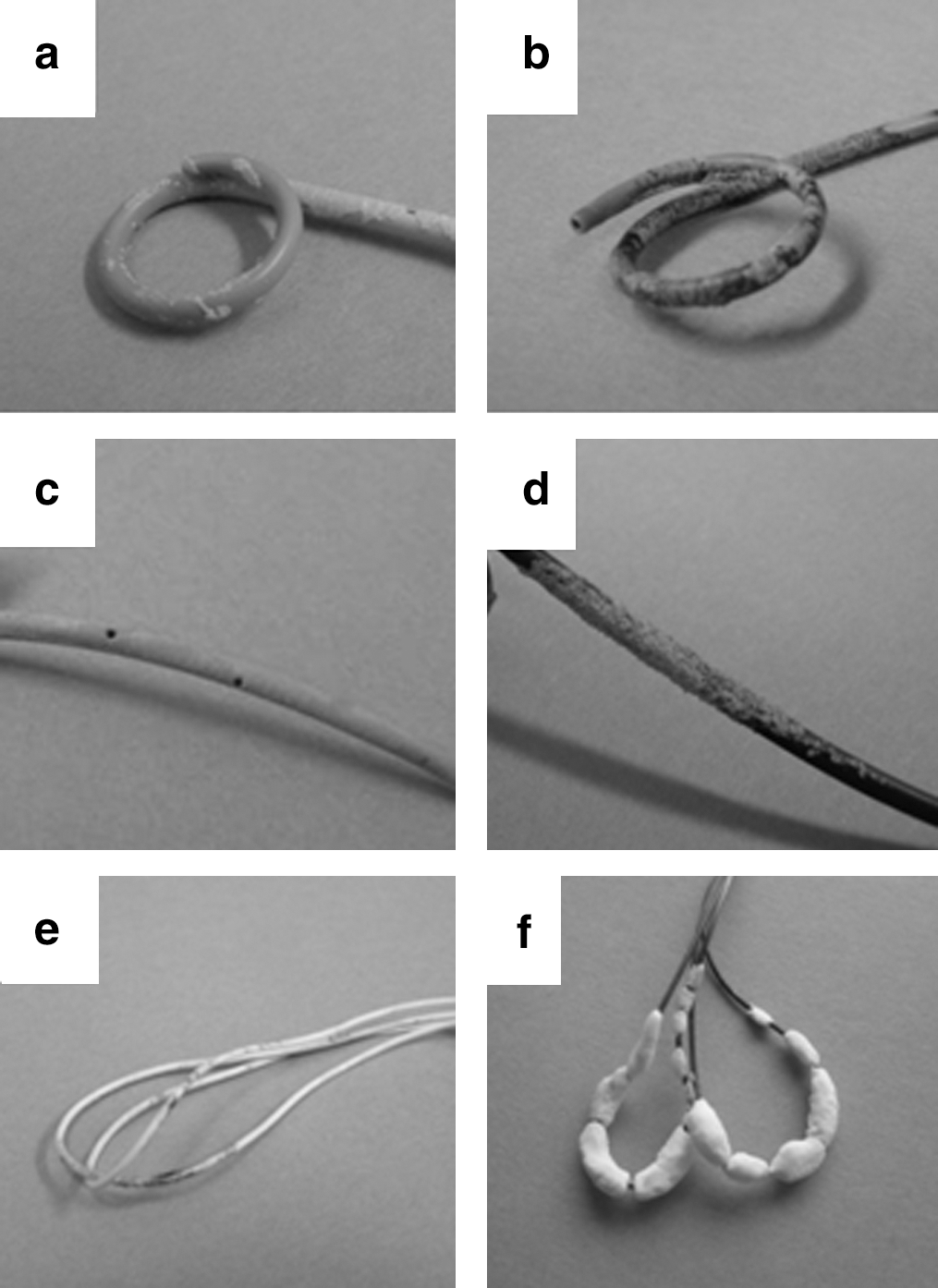
As the level of ureteral stent incrustation increased, the resistance to inserting the guidewire into the ureteral stent was classified as “moderate incrustation,” and when guidewire insertion was impossible, it was classified as “complete incrustation.” We used a guidewire (Endoaccess, Piolax Co, Japan) that had 4 cm of flexible materials with 7 cm of hydrophilic coatings in the head, followed by the stiff end. Moderate incrustation was considered to be present when it was impossible to insert the flexible end, but it was still possible to insert the stiff end. Complete incrustation was considered to be present when it was impossible to insert the stiff end.
The level of resistance was also divided into two grades: “Moderately resistant” and “irremovable.” The moderately resistant grade necessitated more force to remove the ureteral stent using a cystoscope than normal. In addition, the irremovable grade was considered to exist when the stent could not be removed cystoscopically, even if the distal end of the loop was extracted using a 500-mL saline bag in 5 minutes.
With regard to the level of coloration, we classified stents as “brown” if at least of quarter of the stent was brown and “black” when at least a quarter of the stent was black.
Statistical analysis
All continuous variables are expressed as the means±standard deviation. The numerical data were compared by the Mann-Whitney U test. Stent events related to indwelling time were analyzed using the chi-square test. A P value of 0.05 or less was considered to be significant.
Results
A total of 181 patients underwent removal of 330 internal ureteral stents: 324 (98.2%) stents for stone disease and 6 (1.8%) stents for benign ureteral stricture. Of these, 50 patients had two replacements, 23 patients had three replacements, 6 patients had four replacements, 3 patients had five replacements, and one patient had seven replacement stents in each site. The characteristics of the patients and ureteral stents are shown in Table 1. All ureteral stents were made of hydrogel-coated polyurethane.
Overall, 155 (47.0%) stents were found to be encrusted. The site and grade of encrustation are shown in Table 2. The stent length and patency (encrustation, incrustation, coloration, and resistance to removal) were not significantly correlated. In terms of the stent caliber, a size less than 6F led to a significantly higher encrustation rate than was seen in those more than 7F in Figure 2.
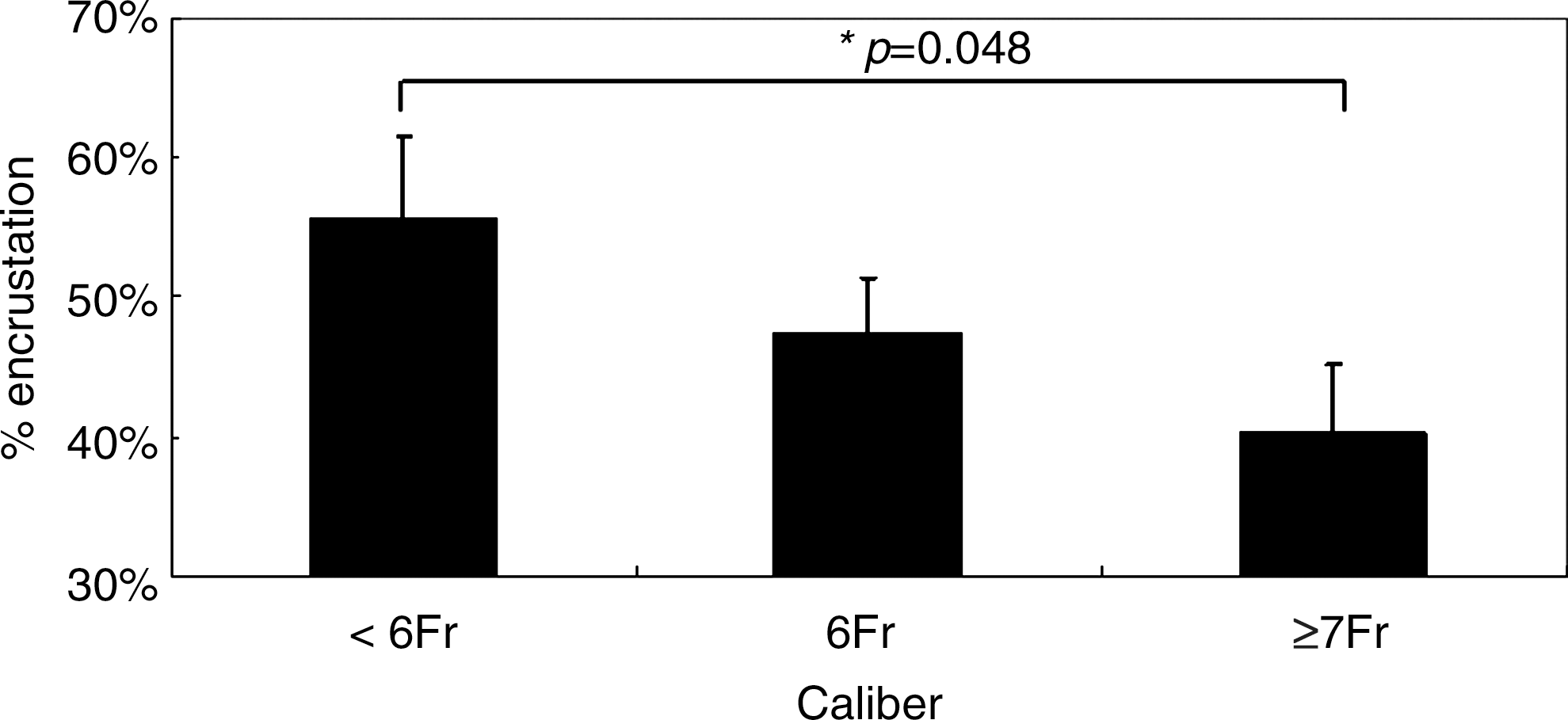
The correlation between stent caliber and encrustation. A size less than 6F led to significantly more encrustation than a size more than 7F. (*: P<0.05)
Of all of the stents, 46 (13.9%) stents were resistant to removal, and three of these could not be removed by cystoscopy. One stent needed SWL and two stents needed URS with a holmium:yttrium-aluminum-garnet (Ho:YAG) laser for removal. The indwelling times of these irremovable stents were 30, 31, and 61 days, respectively.
The site, grade of encrustation, incrustation, resistance to removal, and coloration and their correlation with the indwelling time are shown in Table 3. The incidence of encrustation with or without coloration is shown in Figure 3. The frequency of encrustation with coloration was higher than the incidence without coloration in the stents that were indwelling for less than 6 weeks and for the period between 6 to 12 weeks.
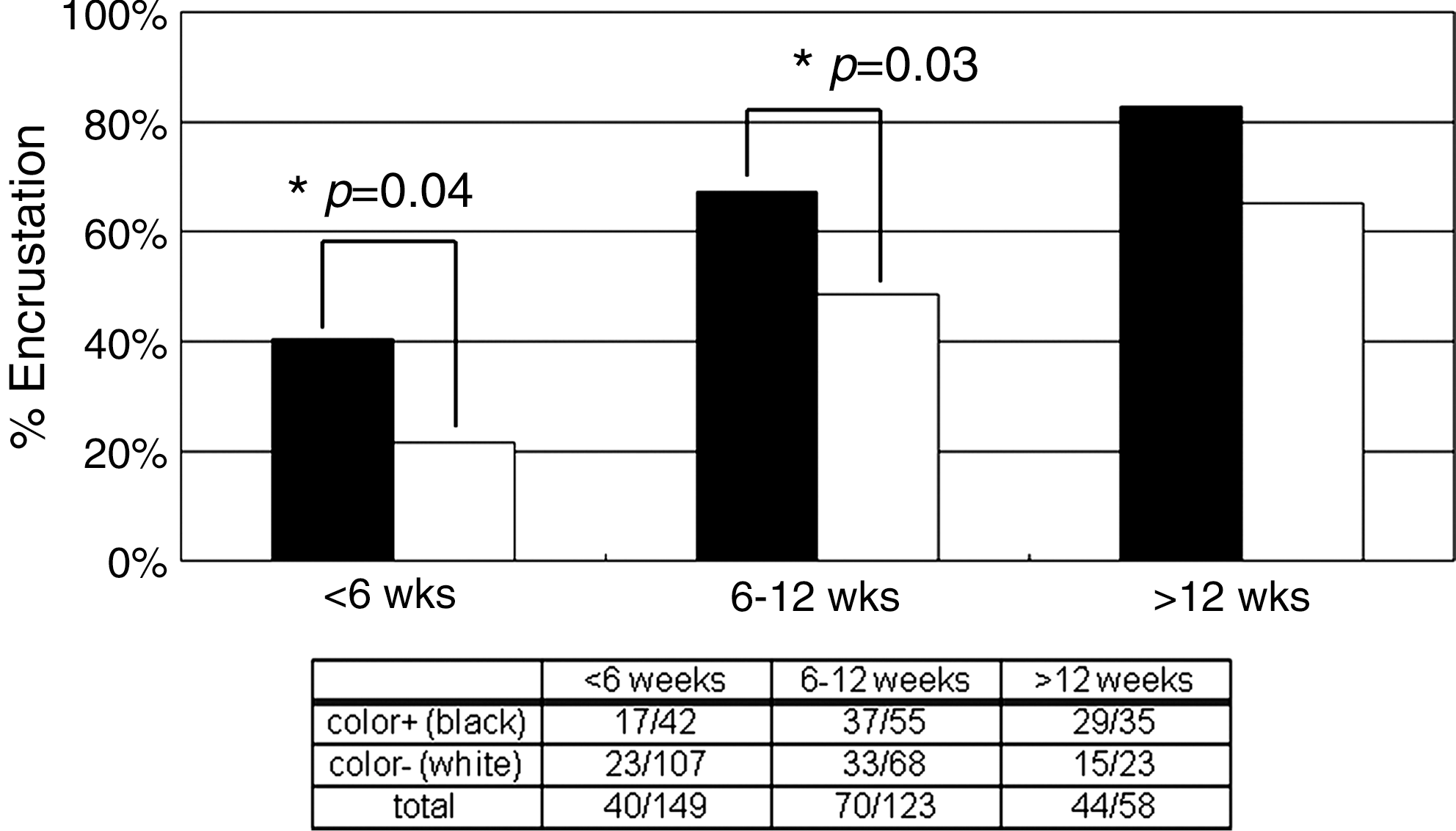
Ureteral stent encrustation with/without stent coloration. Ureteral stents with coloration were significantly more encrusted than those without coloration in both the stents that were indwelling for<6 weeks and 6 to 12 weeks (*: P<0.05).
SWL=shockwave lithotripsy; URS=ureteroscopy.
Discussion
Ureteral stents were first developed in 1967. Since then, various materials and coatings have been developed to help prevent ureteral stent complications, such as encrustation, incrustation, migration, and infections. 1 Because of the improvements in endourologic techniques, the use of ureteral stents has increased in recent years. 8 No widespread consensus for the type or indwelling time to avoid ureteral stent complications has been reached, however. 6,7
Although there are various reasons for encrustation, such as stone disease, urinary sepsis, chemotherapy, pregnancy, chronic renal failure, and metabolic or congenital abnormalities, the ureteral stent indwelling time was the most important factor related to encrustation. 9 A report by el-Faqih and associates 7 indicated that the stent encrustation rate increases from 9.2% for an indwelling time of less than 6 weeks to 47.5% at 6 to 12 weeks to 76.3% at more than 12 weeks. 7 Our investigation supports these data, because the stent encrustation rate was 26.8% at less than 6 weeks, 56.9% at 6 to 12 weeks, and 75.9% at more than 12 weeks in the present study.
Our study included a total of 33 patients who had undergone the insertion of two or more stents on the same side. In patients who have a stent with encrustation, we suggest that the ureteral stent should therefore be exchanged sooner than the initial indwelling time that was used to avoid encrustation. As a result of following this recommendation, the encrustation rate for the initial insertions was 64.2% (median indwelling time: 62 days), while for the second insertion it was 41.8% (median indwelling time: 45 days) in the same patient group (P=0.01).
In our study, the site of ureteral stent encrustation was most frequently the proximal end (upper curl) followed by the distal end (lower curl) and body (midstent). Singh and colleagues 6 reported that dense and thickened encrustation is associated with the upper curl, followed by the body and distal end. Bultitude and associates 3 noted that the reason for the higher encrustation rate in the upper curl may have been because of the presence of more effective peristalsis at the lower part, and because the intraluminal part of the stent is at an angle, thereby decreasing the formation of deposits and also minimizing the encrustation at the lower end.
The study by el-Faqih and coworkers 7 also described that small caliber stents have a higher rate of encrustation. In this study, a size less than 6F was significantly associated with a higher encrustation rate than when the size of the stent was more than 7F. Singh and associates 6 described that stent incrustation precedes stent encrustation. Ultimately, the entire stent may be encrusted both inside and out. 10 Therefore, large caliber stents tolerate a longer indwelling time before they become incrusted, thus resulting in a longer time to become encrusted.
With regard to encrustation, the rate of encrustation is affected by the surface properties, such as roughness and irregularity. While the actual mechanism underlying encrustation is multifaceted, it requires the absorption of proteins onto the stent to start the encrustation process. 10 –13 The mechanism of encrustation in infected urine is a result of organic components in the urine crystallizing out onto the surface of the biomaterial and becoming incorporated into a bacterial biofilm layer. The bacteria continue to grow, leading to the production of urease, which attacks urea and leads to an increase in the urinary pH. The increased pH attracts calcium and magnesium ions to the biofilm matrix, and results in crystal formation. 12,13
The mechanism underlying stent coloration has not yet been proven, either in the present study, or in the previous studies. Most urologists, however, have experienced the coloration of ureteral stents, and sometimes have noted that colored ureteral stents tend to be encrusted. Our data showed that the colored ureteral stents have a higher encrustation rate than the noncolored stents. We speculated that the observed black coloration is a result of the formation of iron sulfide, which is the product of a chemical reaction between hydrogen sulfide and iron. Escherichia coli and Klebsiella pneumoniae, which are the main causal bacteria of urinary tract infections, produce hydrogen sulfide. 14,15 Iron is generally used for radiopaque materials in the ureteral stents. Therefore, black coloration might indicate the presence of a urinary tract infection.
The ureteral flow is reduced to 83%, 61%, and 58% for 5F, 6F, and 7F catheters, respectively. Peristent obstruction of the catheter reduces ureteral flow more than does intraluminal obstruction. 16 Thus, encrustation is more important than incrustation (intraluminal crustation) in terms of the ureteral flow. 6
Bultitude and asociates 3 noted that in the reported irremovable ureteral stents, 42.8% of stents had become difficult to remove cystoscopically within 4 months, and 14.3% had at 2 months. 9 In our study, although the ureteral stent encrustion was related to the indwelling time, heavily encrusted ureteral stents that necessitated additional procedures for removal (SWL and/or URS) occurred within 3 months of implantation. At the times of removal, SWL and URS were chosen as the first step. In cases of small stones (<1.5 cm), SWL should be applied. 2,9 In the case of impacted stones, URS with a Ho:YAG laser is suitable for removal of heavily encrusted ureteral stents. 9 Failure of removal with SWL and URS indicates that PCNL and open surgery should be performed. 2,9,17 –20
The optimal interval for removal of an indwelling ureteral stent to avoid additional procedures for removal is difficult to determine and likely is patient- and situation-dependent. Further studies are needed to prevent heavy ureteral stent encrustation.
The major limitation of our study is that a few stents exceeded 14 weeks of indwelling, including 1 stent that was indwelling for 52 weeks and 12 stents removed at around 15 to 20 weeks. In the previous reports, it was shown that ureteral stents should be exchanged every 2 to 4 months. 1,2,6,19 We performed a Kaplan Meier curve (with encrustation as the end point instead of death) and thus found a 60% survival (nonencrustation) at 60 days and 30% at 90 to 100 days of indwelling time. At our hospital, ureteral stent replacement within 3 months is recommended to prevent heavy encrustation and urosepsis. It is therefore very difficult to investigate longer indwelling ureteral stents based on ethical concerns.
Conclusion
In this study, ureteral stent encrustation was related to the indwelling time. However, heavily encrusted ureteral stents necessitating additional procedures for removal occurred within an indwelling time of 3 months.
Footnotes
Disclosure Statement
No competing financial interests exist.