
Abstract
Background and Purpose:
The recent technologic advances in the newer generation of flexible ureteroscopes have significantly enhanced the therapeutic and diagnostic efficacy of ureteroscopy. The purpose of our study was to assess ureteroscopy and lithotripsy of renal calculi without a safety wire, using the ureteroscope as the safety device.
Patients and Methods:
Medical records for patients undergoing ureteroscopy by a single surgeon were retrospectively reviewed from December 2006 to December 2009. Inclusion criteria for our study included all adult patients who underwent wireless flexible ureteroscopy for the management of renal calculi and had 1 month follow-up data.
Results:
Of the 568 patients who underwent ureteroscopy during this period, 268 patients met our study inclusion criteria. The mean age of the patients undergoing wireless ureteroscopy was 33 years, and the mean body mass index was 33.1 kg/m2. Mean stone diameter of the renal calculi treated was 12.0±5.9 mm. Fifteen percent of the patients had a ureteral stent in place before the procedure, and 84% of the patients had a stent placed after ureteroscopy. Twenty percent of the patients needed ureteral dilation, and 15% of the patients had a ureteral access sheath placed intraoperatively. The overall complication rate was 2.6% (major=0.7%, minor=1.9%). Complications included: Four urinary tract infections, two patients with urosepsis, and one patient with urinary retention. No patients had ureteral perforation or ureteral avulsion.
Conclusions:
Using the ureteroscope as the safety mechanism, ureteroscopy is safe with regard to maintaining renal access and control. Routine safety wires during ureteronephroscopy are not necessary assuring the ureteroscope is in the kidney.
Introduction
Patients and Methods
Institutional Review Board approval was obtained, and the medical records for patients undergoing ureteroscopy by a single surgeon (SYN) were retrospectively reviewed from December 2006 to December 2009. Inclusion criteria for our study included all adult patients who underwent wireless flexible ureteroscopy for the management of renal calculi (with no ureteral calculi) and had 1 month follow-up data. Preoperative patient characteristics, including patient age, sex, body mass index (BMI), stone size and location, were all recorded. Operative notes were reviewed to verify that wireless ureteroscopy was performed, to identify if ureteral dilation was necessary, if an access sheath was used, if a ureteral stent was left postoperatively, and to assess for any intraoperative complications. All medical records were reviewed up to the patients' 1-month follow-up to identify any emergency department visits, hospital admissions, and postoperative complications.
Wireless ureteroscopy was defined as ureteroscopy with laser lithotripsy performed for renal calculi without a safety wire in place. The procedure began with rigid cystoscopy and placement of a 0.035-inch Sensor™ (Boston Scientific) wire up the ureter into the renal pelvis under fluoroscopic guidance. The bladder was drained and the rigid cystoscope removed. The flexible ureteroscope was then passed over the wire under fluoroscopic guidance up to the renal pelvis. Once in the renal pelvis, the guidewire was removed, and ureteroscopy with laser lithotripsy was performed using the holmium:yttrium-aluminum-garnet laser with a 200 -m fiber. (Fig. 1).
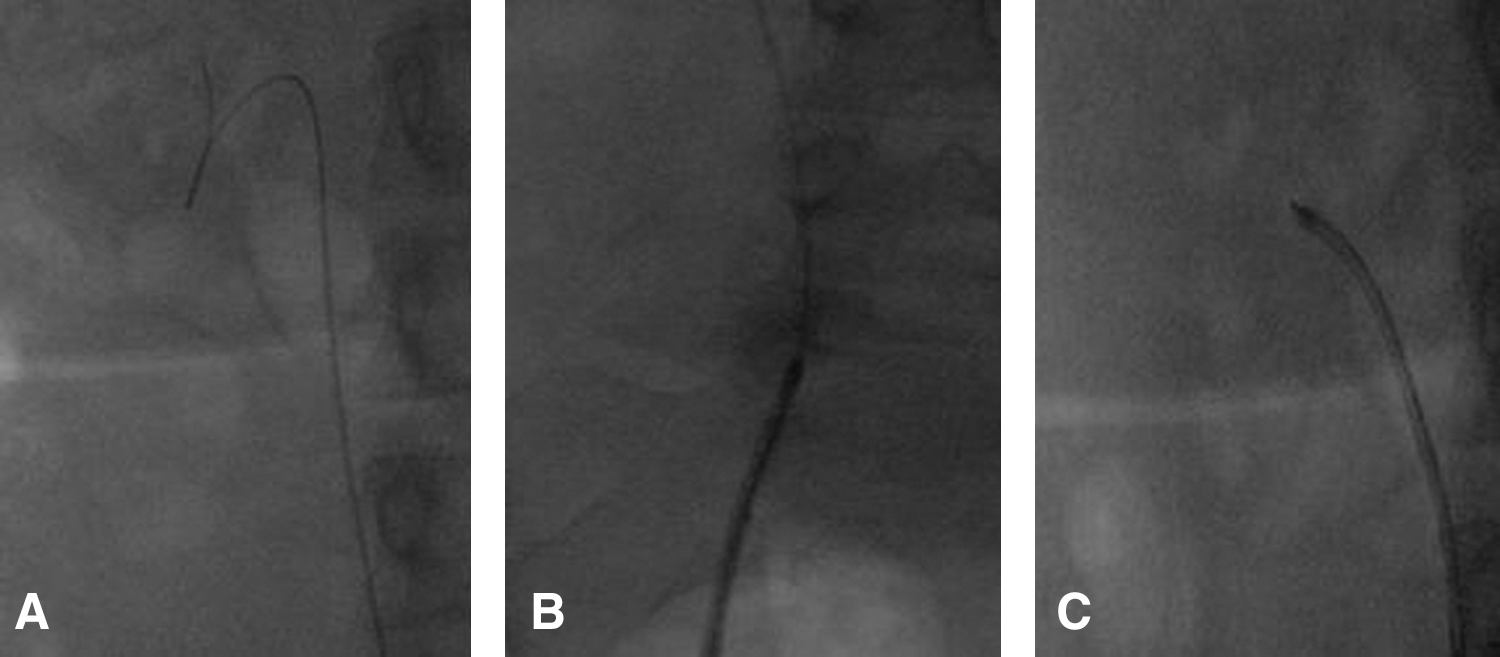
Ureteroscopy without a safety wire.
At the end of the procedure, contrast was used to opacify the collecting system followed by wire placement if a stent was to be placed before removal of the ureteroscope. In cases where the ureteral orifice needed dilation to perform ureteroscopy, an 8F to 10F coaxial dilator (Boston Scientific) was used. A ureteral stent was placed at the end of the procedure in patients with a large stone burden or in patients who needed ureteral dilation. A ureteral access sheath was placed in selected patients with large stone burden or who needed endoscopic basketing of multiple stone fragments.
Results
Of the 568 patients who underwent ureteroscopy from December 2006 to December 2009, 268 patients met our study inclusion criteria. The mean patient age was 33 years, 57% of the patients were female, and the mean BMI was 33.1 kg/m2. The mean stone diameter treated was 12.0±5.9 mm. Stone location was: 34 upper pole calices, 33 middle calices, 101 lower pole calices, and 100 stones in the renal pelvis.
Fifteen percent of the patients had a stent in place before undergoing ureteroscopy, and 84% of the patients had a stent placed postprocedure. Twenty percent of the patients needed ureteral dilation, and 15% of patients had a ureteral access sheath placed intraoperatively. There was a significant difference in the mean stone diameter for patients who had a ureteral access sheath placed vs those who did not have an access sheath placed (18.7±8.5 mm vs 10.9±4.6 mm, P<0.001).
The overall complication rate was 2.6% (major complications: 0.7%; minor complications: 1.9%). There were no intraoperative complications (no ureteral avulsions or ureteral perforations). The two major complications (both Clavien grade II complications) involved patients in whom urosepsis developed that necessitated postprocedure hospital admission and treatment with intravenous antibiotics. One patient had a history of a liver transplant and was receiving immunosuppressive medication. Despite receiving antibiotics before the procedure, a fever developed postoperatively in the recovery room, and the patient was admitted for administration of intravenous antibiotics. The second patient presented to the emergency department with fever the evening after undergoing ureteroscopy and was admitted for treatment with intravenous antibiotics. The minor complications consisted of four patients with postprocedure urinary tract infections (Clavien grade II) that were treated with a course of oral antibiotics and one patient who presented to the emergency department with urinary retention (Clavien grade I).
Access into the renal pelvis was obtained in 267/268 cases. In one patient, we were unable to obtain access to the renal pelvis because of multiple ureteral strictures that ncessitated nephrostomy tube placement and subsequent percutaneous nephrolithotomy. Nine patients presented to the emergency department with stent discomfort necessitating stent removal.
Discussion
A longstanding principle of endourology is to always have a safety wire in place during ureteroscopy. The purpose of the safety wire is to maintain access to the upper tract to facilitate placement of an internal ureteral stent in case of ureteral perforation or excessive bleeding. The technologic advances in ureteroscope design, however, including greater shaft durometer, increased active deflection, and better tip control, have allowed for easier access to the collecting system. The smaller caliber ureteroscopes also minimize ureteral trauma and the risk of ureteral perforation. 1 –3 Overall stone-free rates for ureteroscopy are very high, depending on stone location and size, with many of the patients rendered stone free after a single procedure. 4,5
The safety and minimal morbidity of ureteroscopy in a contemporary series has been shown in a review of 1000 consecutive ureteroscopies performed at the Mayo Clinic. 6 The reported overall complication rate in this series was 1.9%, including a 1.3% rate of ureteral perforation, 0.2% incidence of ureteral stricture with no ureteral avulsions. A review of other contemporary ureteroscopy series revealed a 0% to 4% rate of ureteral perforation and a 0% to 1.3% rate of ureteral avulsion. 7 –9
The potential benefits of a single wire or nonsafety wire method include less frictional drag on the ureteroscope, less distention of the ureterovesical junction, faster access times, and potentially faster procedural times. 1 Eandi and associates 10 used a porcine ureteral model to study the force needed to introduce a ureteroscope in the presence of a safety wire and found that an additional 12 and 20 g of force were needed to introduce the semirigid and flexible ureteroscope when a guidewire was present.
Working in the renal pelvis without a safety wire often facilitates both access (because there is less friction passing the ureteroscope over a guidewire compared with alongside it), and scope manipulation (because the safety wire may hinder access to the stone as well as increase the torque necessary for rotation of the ureteroscope). At the end of our procedure, contrast is injected through the ureteroscope to opacify the collecting system, and a wire is placed through the ureteroscope before removal to facilitate stent placement.
Moran and Bratslavsky 11 were the first to report the safety of the wireless approach in an abstract on a series of 340 consecutive flexible ureteroscopies performed without a safety wire compared with a large single-center experience of 1500 patients. The stone-free rates between both series were similar (96%) with failures in the wireless group occurring in patients with high-grade obstruction and/or impacted calculi. There were no complications in patients undergoing ureteroscopy without a safety wire. The authors concluded that there were no benefits to placing a safety guidewire in their comparative series. Other ureteroscopy series performed without the use of a safety wire for ureteral and renal calculi, diagnostic ureteroscopy, and ablation of upper tract transitional-cell carcinoma have also demonstrated the wireless technique to be safe with no reported intraoperative complications (Table 1). 10 –13
URS=ureteroscopy; intraop=intraoperative; TCC=transitional-cell carcinoma; postop=postoperative; UPJ=ureteropelvic junction.
Ureteral access sheaths are useful adjuncts to ureteroscopy that allow safer repeated insertion and withdrawal of a ureteroscope. 14,15 Access sheaths also allow for continuous irrigation of the renal pelvis and improved stone clearance as well as allow for lower renal pelvic pressures that may be protective against pyelovenous and pyelolymphatic backflow. 16,17 For patients with a larger stone burden (mean stone size: 18.7 mm), we placed a ureteral access sheath to aid in ureteroscopy with laser lithotripsy and to allow easy basketing of fragments with minimal morbidity. For patients with smaller stones (mean stone size: 10.9 mm) in our series (85%), we did not use a ureteral access sheath and did not extract stone fragments with a basket. Stone basketing can potentially lead to iatrogenic injury to the ureter on each passage of the ureteroscope. Reported complications from ureteroscopy with stone basketing in large series have included ureteral avulsion (0.28%), major ureteral perforation necessitating surgical repair (0.06%), minor ureteral perforation (1.99%), mucosal abrasion (0.52%), and ureteral stricture (0.58%). 7 To minimize morbidity, we generally do not extract stone fragments after ureteroscopy and laser lithotripsy for smaller renal pelvic stones.
Despite the safety of the wireless approach, there are scenarios in which a safety wire should be used. Our study focused solely on renal calculi, but a safety wire should be considered in patients with ureteral calculi, especially if there is a significant amount of ureteral edema or in patients with impacted ureteral calculi. Other cases in which a safety wire should be used include during dilation of a ureteral stricture and when basketing ureteral calculi. Endoscopic adjuncts such as a ureteral access sheath may be used in certain cases to aid in the retrieval of multiple stone fragments and protect the ureter from iatrogenic injury. We also recommend using a safety wire when performing endoincision of the ureter such as during an endopyelotomy or incision of a ureteral stricture because there is a higher risk of bleeding and the possible need to place a stent urgently. Patient safety is of paramount importance; thus,in any endoscopic situation in which there is abnormal anatomy, difficult visualization, or possible difficulty in placing a ureteral stent, a safety wire should be placed.
In our series, ureteroscopy was performed by a fellowship trained endourologist (SYN) with many years of experience. Wireless ureteroscopy should be performed by those urologists who are comfortable with ureteroscopy, and if there is any doubt about whether a safety wire should or should not be placed, it is best to err on the side of caution and place a safety wire. Future prospective studies comparing wireless vs safety wire cases may be needed to better compare success rates, complications, operative time, and cost.
Conclusion
The technologic advances in the newer generation of flexible ureteroscopes has significantly enhanced the therapeutic and diagnostic efficacy of ureteroscopy. Thus, ureteroscopes can act as their own safety wire in the renal pelvis. Flexible ureteroscopy without a safety wire is a safe technique for the management of renal calculi.
Footnotes
Disclosure Statement
Dr. Nakada is a consultant for Cook Urological, For the remaining authors, no competing financial interests exist.