
Abstract
Background and Purpose:
The vast increase in recent publications on renal mass biopsy (RMB) suggests an increased interest in the subject. The objective of the survey was to assess the use of RMB in current urologic practice, including related factors such as indications and patterns in practice.
Methods:
The link to a web-based questionnaire (
Results:
In total, 190 responders completed the survey of whom 73% indicated performing RMB “never” or “rarely” compared with 9% performing RMB in 25% to 100% of cases. Thirteen percent of responders reported never to take a RMB. Of the latter, significantly fewer practice in university hospitals (6% vs 20%–30%, P=0.003). Main indications to perform RMB are still tumors in solitary/transplant kidneys and in metastatic disease. Lack of influence on clinical management and risk of false negatives were the main reasons not to perform biopsies. Sixty-one percent prefer histological biopsies compared with 8% who prefer cytological aspiration; 31% indicated that they combine both techniques. Other tissue differentiation techniques (Optical Coherence Tomography, Raman-spectroscopy) are unknown to 65% of urologists.
Conclusion:
RMB is not yet applied widely in urologic practice, with academic urologists performing RMB less infrequently. Core biopsies are still preferred, although combined with cytologic punctures by a considerable number of responders.
Introduction
Nevertheless, increased literature diffusion may not necessarily reflect changes in clinical practice, because new diagnostic methods occasionally need several years before they are fully implemented in current practice. 9 In the previous decade, two surveys exploring the role of RMB in medical practice 10,11 showed that RMB was scarcely performed. The primary objective of the current study was to assess the use of RMB in current urologic practice. A secondary objective was to assess related factors such as indications and patterns in practice.
Methods
An electronic survey was generated (
Statistical analysis
Analysis was performed based on the result overviews provided by the Surveymonkey-website. Subsequent statistical analysis was performed in close collaboration with the biostatistical department of our institution and using Predictive Analytics SoftWare (PASW) 18.0.2. The Pearson chi-square test was applied on cross tables to assess unequal distribution of answers between the different groups of responders. To assess differences between specific groups of responders individually, the cross tables were subdivided in 2×n tables. When applicable (ie, ordinal variables) the chi-square test for trends was performed to demonstrate a linear trend between variables. For all tests, a P value less than 0.05 was considered statistical significant.
To prevent confusing figures, responses (in percentages) on indications for and reasons to refrain from performing RMB were grouped in “most important” (first and second most important indications), “least important” (the last two least important indications), and the reactions in between these categories as “median.” GraphPad Prism 5.01 for Windows was used to create the figures.
Results
In total 190, of the 1854 persons responded, resulting in a response rate of 10.2%.
Demographic data
Demographic data is displayed in Table 1. Overall majority of responders were urologists with a median of 10 years since registration (0–45). The majority of the responders practiced in North America (57%) and 72% in training hospitals (57% university- and 15% nonuniversity training hospitals). Eighty-seven percent of responders practiced in either North America, Europe, or Asia.
Patterns in practice
The majority of responders (73%) never or rarely take biopsies and only 9% of the responders take biopsies in more than 25% of cases (Table 2).
Of the responders who indicated they performed RMB, 61% perform only histological (core) biopsies (CB) whereas 31% perform both histological CB and cytological punctures (Table 2).
Biopsies are mainly performed by radiologists and with a 18-gauge needle (78% and 62%, respectively), and CT-scan is the guidance modality of preference (62%), followed by ultrasound (37%). Seventy-eight percent reported never to use MRI for guidance.
Table 3a shows the distribution of biopsy rate over the different types of practice. Pearson chi-square shows an unequal distribution over the different types of practice (P<0.001). Subdividing the results in 4×2 cross tables shows that there are differences in the rate of biopsy performance between all the hospital types with the exception of nonuniversity training hospital vs private practice: University hospital vs nonuniversity training hospital (P=0.001), university hospital vs nontraining hospital (P<0.001), university hospital vs private practice (P<0.001), nonuniversity training hospital vs nontraining hospital (P=0.008), nontraining hospital vs private practice (P<0.001), and nonuniversity training hospital vs private practice (P=0.263). In all the 4×2 cross tables, there were no significant differences for the chi-square test for trend: University hospital vs nonuniversity training hospital (P=0.406), university hospital vs nontraining hospital (P=0.571), university hospital vs private practice (P=0.052), nonuniversity training hospital vs nontraining hospital (P=0.869), nonuniversity training hospital vs private practice (P=0.360), nontraining hospital vs private practice (P=0.309). There was a significant difference, however, in the rate of “never perform biopsy” between those responders practicing in university hospitals compared with the other types of practice (6% vs 20%–30%, chi-square test P=0.003).
The distribution of biopsy rate frequency per continent is displayed in Table 3b. Chi-square test showed an unequal distribution of biopsy rate over the regions (P<0.001). When distributions were subdivided by 4×2 cross tables, no difference was found between North America and Europe (P=0.402); however, the biopsy rate in Asia differed significantly from the two western regions (chi-square test for trends P<0.001 for North America and P=0.002 for Europe, respectively).
Changing attitudes toward biopsy based on the recent literature and knowledge of developmental imaging techniques with potential as a substitute for the histopathological biopsy are shown in Table 4.
OCT=optical coherence tomography.
Indications for RMB
Indications to either perform or to refrain from RMB are best displayed in Figure 1.
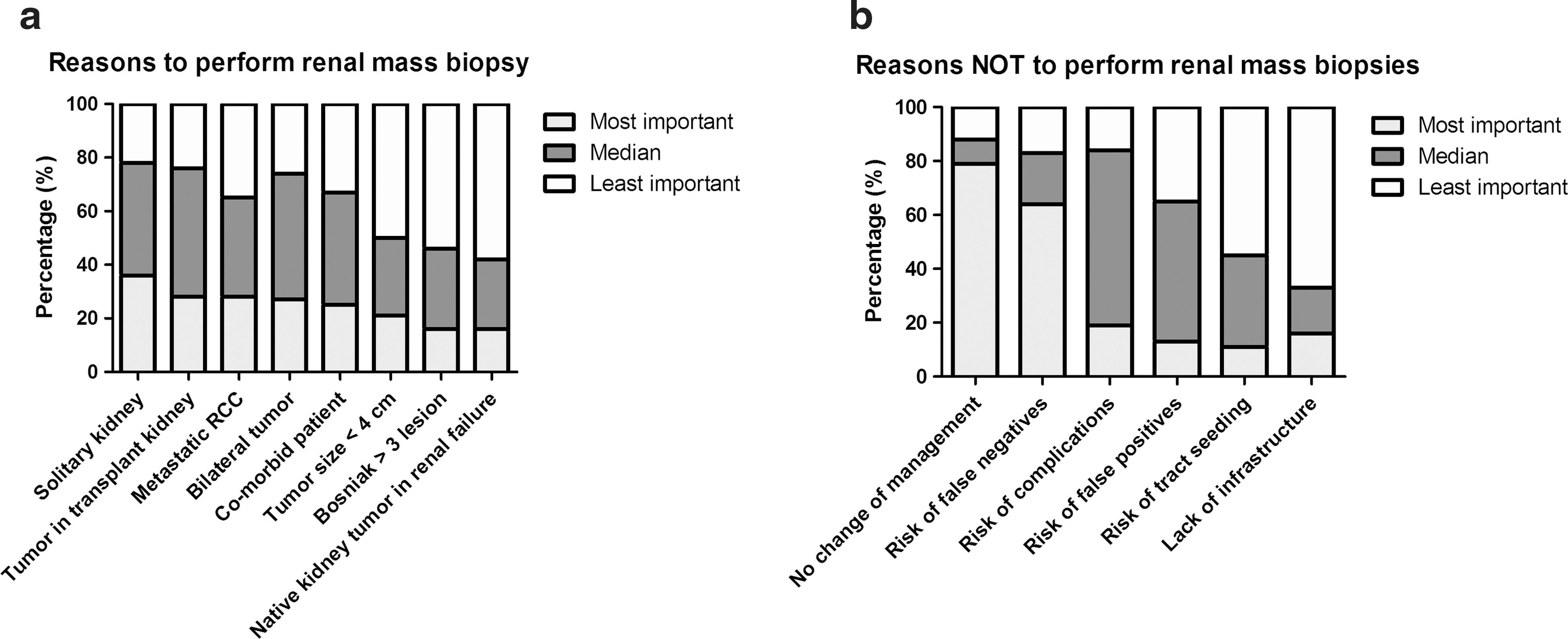
Indications to perform
Discussion
Our electronic survey distributed to members of the EUS demonstrates that only a minority of urologists performs RMB regularly.
Patterns in practice
Results of biopsy diffusion should be compared with previous surveys. 10,11 Data on clinical practice type, years in practice, and hospital size (number of beds) in our survey were comparable with the Kümmerlin and colleagues 11 survey. Nevertheless North American urologists were more prevalent in the current survey while there was a majority of European responders in the 2005 survey held during the World Congress of Endourology in Amsterdam, the Netherlands (57% North America and 19% European in the current vs 16% North America and 45% European in the 2005 survey. Comparison of such characteristics with the survey of Khan and associates 10 is hindered because the presentation of questions was different.
The number of responders that “never take a RMB” decreased from 56% to 43% in 2005 (both previous surveys were conducted in 2005) to 13% in the current survey with a linear trend to increasing penetration in clinical practice (Table 5). Nevertheless, the real impact of RMB in the diagnostic process of renal masses remains low with only 9% of the responders taking biopsies in at least 50% of cases. These figures do not reflect the significant growth of publications in the last years. The discrepancy between literature diffusion and effective implementation in clinical practice is a well-known phenomenon and rather than physicians alone, the organization of care, resources, leadership, and social environment are the main causes delaying implementation. 9
The chi-square test for trends showed a statistical significant difference in biopsy rate between the current survey and that of Kummerlin and associates (P<0.001).
NA=not applicable; FNA=fine needle aspiration.
The type of practice does not seem to influence the frequency in performing a biopsy. Comparison of the different types showed differences among all of them except between nonuniversity and private practice. While these data suggest a difference in the biopsy frequency between university hospitals and all other types of practice, a trend could not been proven toward higher frequency in any of the practice types in the current survey. Nevertheless, there was a significant difference in the rate of responders that “never” perform a biopsy between the university hospitals and the nonuniversity hospitals. This figure may indicate that biopsy policy is more liberal in university settings were the influence of recent literature or study purposes are higher than in private or nontraining sectors.
Histological CB is preferred over cytological fine needle aspiration (FNA), although one-third of the responders combine both. Overall, 40% of the responders use FNA, a fair increase with respect to the 2005 survey 11 (Table 5). This might be explained by encouraging reports on FNA accuracy in determining biology and subtype and high interobserver concordance as well as implementation of ancillary cytopathologic techniques. 4,8,12,13 Furthermore, combination of both types of biopsies improves the accuracy of the test including subtype and grade. 14 –16 The majority of the biopsies are taken by radiologists, and in more than half of the cases, the 18G needle is preferred over other calibres.
Rationale for biopsy
For almost 40% of the responders, the main reason to perform a biopsy is a solitary kidney followed by tumor in transplant kidney, metastatic RCC, bilateral tumor or presence of comorbidity, and tumor categorized as SRM. These figures fully reproduce the results of a previous survey where the presence of a tumor in a solitary kidney or bilateral tumors were the most important indications to perform a biopsy. 10 While no overall changes in attitude could be recorded, the present survey underscores that biopsy is increasingly considered in the case of metastatic RCC, from 29% of responders taking a biopsy in 2007 to 65% indicating in the current survey that this is the most/moderate important reason. As far as this indication is concerned, however, the physician has to be aware that a high accuracy in subtype determination is needed because this will drive the choice of systemic therapy. 13 The recent reported lower accuracy of the RMB in those large and heterogeneous metastatic renal masses may hinder the usefulness of RMB in this setting. 17
The presence of a SRM was not among the most important reasons to perform a biopsy in our survey. Approximately 50% of the responders indicated that a small tumor size was one of the least important reasons. Although surgical series consistently show that the probability of a benign lesion increases with decreasing tumor size, 1,18,19 implementation of partial nephrectomy obviates the need for a mandatory preoperative biopsy because tissue will be available for pathologic diagnosis. Conversely, a diagnosis can only be established by means of a biopsy when ablation therapy or active surveillance is the strategy of choice. When considering the still limited penetration of the last two policies, it is understandable that 80% of the responders in the current survey identified the lack of change in management as the most important reason “not to perform a RMB.”
Still, the risk of false-negative results was the second most important reason not to biopsy. There is, for this rationale, an apparent contradiction with the recent literature. Recent reviews and original articles show that false-negative results are almost sporadic. 4,5,20 Although accuracy of RMB has been rising, still a shortcoming is the highly variable definition of accuracy. Influence on clinical management can only be expected when the diagnostic test provides a high accuracy, and in the case of a biopsy, erroneous sampling or failed biopsies should be included in the calculation of overall accuracy because the test did not support the diagnostic objectives.
Limitations
The response rate in our survey might be considered as a major limitation. Several factors can explain the lower response rate compared with the 64% 10 and 22.2% 11 of the previous surveys. First, the current survey was sent to all the e-mail addresses of members of the EUS, regardless of their field of interest or their type of practice. It is likely to assume that members of the EUS not involved in treatment of renal tumors are less willing to respond to the current survey. Furthermore, it is possible that a part of the e-mail addresses was outdated and therefore the message never reached those recipients. Last, it is well known that postal or locally distributed surveys such as the previous two generate a higher response rate compared with a web-based survey with e-mail announcements. 21
When compared with other surveys, however, the current study is standing out because it is fully focused on RMB and contains a comprehensive set of questions that address multiple aspects of the matter. Furthermore, it was distributed by a professional society with an own target population, and preparation and implementation of the study was done completely independent without any support from third parties, such as commercial companies. Before distribution, a pilot version of the study was tested by several senior and junior urologists both in the Netherlands and in the United States for ease of use and linguistics.
Conclusion
Despite the relatively low response rate when compared with other studies, the current survey suggests that there is a significant decrease in the rate of responders indicating “never to take biopsy.” The real impact of RMB in the preoperative workup of renal masses still remains low, however. Main reasons to perform RMB did not change mainly apart from a clear increase in the rate of responders taking biopsy in case of metastatic RCC. SRM alone is not considered an important reason to perform RMB. The use of FNA has increased in the last years, particularly in combination with core biopsy.
Footnotes
Disclosure Statement
No competing financial interests exist.