
Abstract
Purpose:
We report results of the introduction of a laparoscopic radical prostatectomy (LRP) care pathway. This included the introduction of a transversus abdominis plane (TAP) local anesthetic block and other measures to reduce the impact of factors known to delay postoperative recovery. Outcomes including pain, analgesic requirements, complications, and length of stay are reported.
Patients and Methods:
Two hundred consecutive patients undergoing LRP from 2008 to 2010 were prospectively studied. A detailed perioperative care pathway was developed and implemented. The pathway was modified after a pain audit to include bilateral transversus abdominis plane regional anesthetic blockade. Same day discharge criteria were applied to suitable patients. Demographics and perioperative and follow-up data were prospectively collected and recorded on a database.
Results:
Overall, 78% of cases were discharged after 1 night stay; 14 patients were managed as true day cases without overnight stay. Operative time (P<0.0001), intraoperative blood loss (P=0.018), %≤1 day stay (P=0.0091), transfusion, and conversion rate (nil in latter 100 cases) all improved significantly in the second 100 group of patients compared with the first 100 cases. The introduction of TAP blocks led to significant reductions of mean intraoperative and postoperative opiate use (17.3 mg to 1.3 mg and 1.9 mg to 0.2 mg morphine, respectively) without any significant effect on perceived pain. True day cases did not experience a significantly different rate of complications than the whole cohort.
Conclusions:
Through a structured care pathway incorporating the TAP block, 1 night stay laparoscopic prostatectomy can be safely delivered with reduced inpatient stay costs. In selected patients, day-case prostatectomy is feasible.
Introduction
We therefore set out to systematically reduce the impact of surgery to the patient through thorough patient preparation (ie, procedure and perioperative pathway counseling, preoperative anesthetic assessment), and complete minimization of perioperative symptoms. Our aim was to reduce LOS while maintaining safety. This strategy was supported by a prospective pain and analgesia audit before and after introduction of transversus abdominis plane (TAP) local anesthetic block. The TAP block has previously been described for open radical prostatectomy patients. 2 It was shown to reduce morphine requirements by up to 70% and reduce postoperative nausea and vomiting by 50% in open abdominal surgery 3 and has been shown to be effective in randomized controlled trials for obstetric and gynecologic surgery and laparoscopic cholecystectomy. 4 –6 After the introduction of the care pathway including the TAP blocks, we observed improvements in recovery that led to patients inquiring about same-day discharge.
We describe the care pathway we have used, results of our audit of TAP blocks on pain and analgesic requirements, and perioperative details including LOS, complications, and readmission data.
Patients and Methods
Patient selection and preparation
The current care pathway is shown in Table 1, and its evolution is described below. All 200 consecutive patients who underwent LRP from 2008 to 2010 were included for the purpose of this report regardless of pelvic lymphadenectomy or variation in indication (organ-confined vs locally advanced). In addition to National Institute of Clinical Excellence standard practice of selection and workup, all patients are advised to anticipate a 1-night stay in hospital or, in some cases, same-day discharge (<12 hours). Patients were considered for same-day discharge if they met the following conditions: American Society of Anesthesiologists score 1 or 2, body mass index <30, with blood loss <200 mL, <10 mg morphine (or equivalent) perioperative opioids, watertight anastomosis, minimal discomfort or malaise, drain not needed, and responsible adult at home. Patients whose procedures lasted >2 hours were initially not considered for same-day discharge, although this condition was later relaxed because patients with procedure times 2 to 3 hours long appeared well enough to go home. A cutoff of 3 hours is now used. Demographics and perioperative and follow-up data were prospectively collected and recorded in a database.
IV=intravenous; PR=per rectum.
Initial anesthetic technique (patients 1–100)
Initially, patients received a standard general anesthetic using propofol, fentanyl, and vecuronium for induction, sevoflurane in air/oxygen for maintenance. Invasive monitoring was not used routinely. Intraoperative fluids were restricted to 1.5 L, and patients were ventilated to maintain a normal end-tidal CO2. Patients received paracetamol, a nonsteroidal anti-inflammatory drug (NSAID), and morphine sulphate toward the end of the procedure. Postoperative pain experienced while in the recovery ward was managed with additional doses of morphine sulphate as needed. Once on the ward, patients received regular paracetamol, diclofenac sodium, and tramadol with morphine as needed.
Perioperative pain audit
An audit of on-demand analgesia use and postoperative pain was conducted before and after introduction of bilateral TAP blocks to the care pathway. The audit measured opioid analgesia use (mg of morphine or equivalent), and pain was assessed while the patient was in the recovery ward, 3 to 4 hours after TAP block insertion, using a categorical pain scoring system with visual aids (1=no pain; 2=mild pain; 3=moderate pain; 4=severe pain; 5=worst possible pain). 7 The audit started with patient no. 80 and ended with patient 159 (n=79). TAP blocks were introduced in patient 101. After the audit, TAP blocks were routinely performed in all patients.
TAP block technique
Having obtained prior consent, TAP blocks were placed after induction of anesthesia before the procedure as described previously. 8 Briefly, TAP blocks were placed under sterile conditions and with ultrasonographic guidance (Esaote MyLab25 Vision). An anterior approach was used with the ultrasound probe placed in the flank, between the 12th rib and the iliac crest. At the beginning of each procedure, 20 mL of 0.375% bupivacaine was inserted bilaterally with an “oval filling sign” on injection of local anesthetic confirming correct positioning of the anesthetic.
Current anesthetic technique (patients 101–200)
As well as routinely receiving a preprocedure TAP block, patients now receive a standard general anesthetic using propofol, fentanyl, and vecuronium for induction, desflurane in air/oxygen for maintenance, and intravenous paracetamol and diclofenac sodium for routine postoperative analgesia. Patients 101 to 109 routinely received morphine, 5 mg, at the end of surgery; however, this was omitted from patient 110 onward because it appeared unnecessary. Hyoscine, 20 mg, was routinely given as prophylaxis for bladder spasm. For postoperative analgesia, patients received regular paracetamol and diclofenac with oxycodone supplemented as needed.
Surgical technique
LRP was performed using the technique described by Stoltzenburg 9 that uses extraperitoneal balloon dissection. The following modifications were undertaken: Endopath (Ethicon) ports, peritoneal fenestration for bilateral pelvic lymph node dissection in intermediate or high-risk patients, avoidance of Robinson drain, and use of hemostatic adjuncts (Surgicel [Ethicon, Livingstone, Scotland] and FloSeal [Baxter, UK]) where indicated, limitation of Trendelenburg position, low CO2 insufflation pressure, and avoidance of hypercapnia, and lastly, stress test of anastomosis for water tightness.
Postoperative care, discharge arrangements, and follow-up
Patients are nursed in a day-case/short-stay ward and are encouraged to drink, eat, and mobilize within 2 to 3 hours of surgery. The patients operated on in the morning, who fit true day-case criteria, are considered for discharge during the afternoon after consultant review. In addition, for true day-case LRP, patients are provided with direct telephone contact details of the surgeon in case of any early complications not recognized before discharge. Patients living far away or who are not well supported at home are not selected for same-day discharge. Nurse-led trial without catheter takes place 7 days after the procedure. True day-case patients are followed up with a phone call and questionnaire on the first postoperative day to address safety concerns and accurate prospective capturing of complications. Routine catheter urine and midstream urine cultures are obtained to seek out proactively and treat infections at the time of catheter removal and again at first outpatient review. Outpatient review is arranged early at 30 days for the same reason. All complications were classified according to the modified Clavien-Dindo system. 10,11
Data were statistically compared when appropriate with Mann-Whitney, Wilcoxon, Student t, chi-square, or Fisher exact test.
Results
Patient demographics, relevant preoperative clinical and pathologic data including descriptive statistics are illustrated for the entire cohort as well as the first and second 100 patients and true day-case patients (Table 2).
TAP=transversus abdominis plane; preop=preoperative; PSA=prostate-specific antigen; LOS=length of stay.
Overall, 156 (78%) men were managed as 1-night stay patients and 14 (7%) of these were true day-cases, all occurring in the second cohort who received a TAP block. Operative time, intraoperative blood loss, transfusion, and conversion rate all improved significantly in the second 100 group of patients compared with the first 100 cases and were particularly low in the highly selected group of true day-case patients (Table 2).
Audit of pain and opioid use before and after introduction of preprocedure TAP block
We observed that the main sources of pain were the anterior abdominal wall (despite standard port site local anesthetic infiltration) and referred pain to the penis as a result of bladder spasm. To avoid systemic opiate analgesia and reduce the associated side effects, a preprocedure TAP block was introduced, and bladder spasm was medicated with hyoscine, 20 mg, as prophylaxis. Mean perioperative and postoperative intravenous morphine use reduced significantly from 17.3 mg to 1.3 mg and 1.9 mg to 0.2 mg, respectively. The last 49 of the 59 patients in the post-TAP audit have not used morphine in the recovery ward. Mean postoperative pain scores reduced slightly from 1.47 to 1.3 (P=0.99) after the introduced changes (Table 3, Fig. 1). No change in pain scores was anticipated because only the modality of pain relief was changed. There were no TAP block related complications; however, two patients were noted to have a temporary rise in creatinine level related to NSAID use that may not have occurred if opiates had been used.
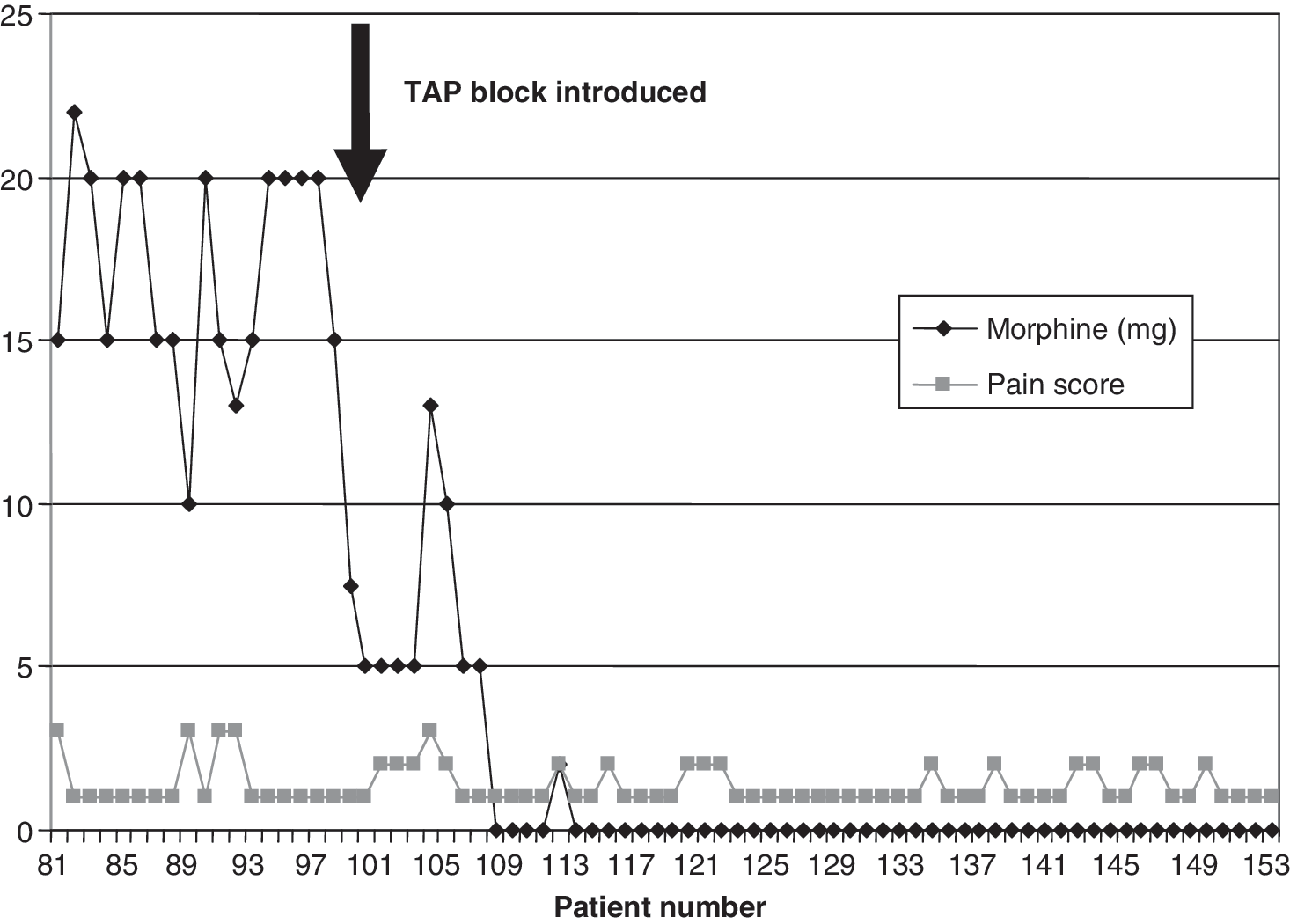
Audit of opioid use (patients 80–159): Perioperative intravenous morphine use and postoperative pain scores during adjustment of care pathway. Arrow indicates introduction of transversus abdominis plane (TAP) block.
Analysis of complications and safety of true day-case discharges
Minor complications (Clavien I and II) are common, particularly when sought out proactively as in this cohort (Table 4). Clavien IIIa events (necessitating intervention) were more common in the second cohort because of an increased rate of extended pelvic lymphadenectomy. No events necessitating general anesthetic were observed (Clavien IIIb). Only two potentially life-threatening complications occurred after discharge in the entire study cohort (extraperitoneal pelvic hematoma and pulmonary embolism). Both patients presented with symptoms at the time of catheter removal 7 days postoperatively (ie, after the standard discharge time) and were treated conservatively. We therefore conclude that same-day discharge is a safe practice, provided patients are accompanied by a well-instructed adult, have direct telephone access to the surgical team, and receive telephone follow-up on the first postoperative day.
TAP=transversus abdominis plane; ASA=American Society of Anesthesiologists.
Discussion
Early discharge after minimally invasive radical prostatectomy clearly brings direct benefits to both patients and healthcare providers through an earlier return to home and reduced inpatient related costs. It is the underlying improvements in perioperative care, however, which allow early discharge that highlight the benefits for all involved. We have described how, through attentive management of all areas of patient recovery, complications can be limited and symptoms can be reduced. Our data would suggest that patients' perioperative quality of life impairment may be minimized compared with standard care, and formal quality of life studies are now needed to evaluate this hypothesis.
The technical aspects of our care pathway each play a part in delivering a low morbidity procedure that allows early recovery. Key to the pathway was the team who all contributed to small improvements. In particular, the development of a specific anesthetic technique for LRP reduced the postoperative pain and drug-related side effects. We have shown through our audit data that the introduction of the TAP block before the procedure results in lower levels of needed opioid analgesia to almost abolishment. This aspect of the care pathway we think has made a significant improvement to the recovery of the patients. Other technical points, including strict control of insufflation pressure, active respiratory compensation for hypercapnia, minimization of Trendelenberg tilt, meticulous hemostasis, and a watertight anastomosis that allows for drain-free surgery, all contribute to early recovery.
It is also important to note that the success of a LRP program depends on the initial training of the surgeon and assistants. Ideally, fellowship training in an institution where many cases can be performed over a short period will allow the surgeon to start in his or her own institution without a long learning curve. The primary surgeon in our series underwent such training, yet it is clear from our data that improvements were made between the first and second 100 cases, indicating perhaps the additional learning curve of the team. Indeed, the skills of the assistant are crucial for this procedure, and we have observed marked lengthening of procedure times when new trainees join the team. Previous dry and wet laboratory training to gain appropriate skills is an essential prerequisite for assistants to prevent avoidable problems at the time of team transition.
The evolution of our care pathway resulted in a number of patients commenting on the evening of surgery that they felt well enough to go home. We also observed that patients presented no serious complications after discharge and the complications that did occur were identifiable early after surgery. This led us to informally ask if patients would find day-case surgery desirable. In essence, there was a group of motivated men who were fit and were well supported at home and who lived locally who found the idea of same-day discharge attractive. We outlined caveats, such as difficulties during and after the procedure (long procedure, pain, bleeding, etc.), and prepared a detailed postoperative discharge note and advice sheet with a contact number for the surgeon. It is not inconceivable that an unrecognized complication could one day occur. Thus, we make telephone contact the next morning to assess pain and try to identify potential symptoms of complications.
Our early experience of 14 patients managed as true day cases indicate that this approach is feasible and worth considering in men who fit clearly defined day surgery criteria. In the future, it may be possible to further improve safety through the use of unobtrusive ambulatory cardiovascular monitoring devices that can communicate with the hospital. These could alert clinicians to the early signs of sepsis and hypovolemia. 12
Footnotes
Disclosure Statement
No competing financial interests exist.