
Abstract
Percutaneous nephrolithotomy (PCNL) is one of the most common treatment options in the management of kidney stones in children. While colon perforation during PCNL is reported as a rare complication in adults, there are scarce data regarding colon perforation during pediatric PCNL. We report the successful management of colon perforation occurring during PCNL and of a renal stone in a 6-year-old child. Moreover, we describe the procedure to be followed for colon perforation in children.
Introduction
Case Report
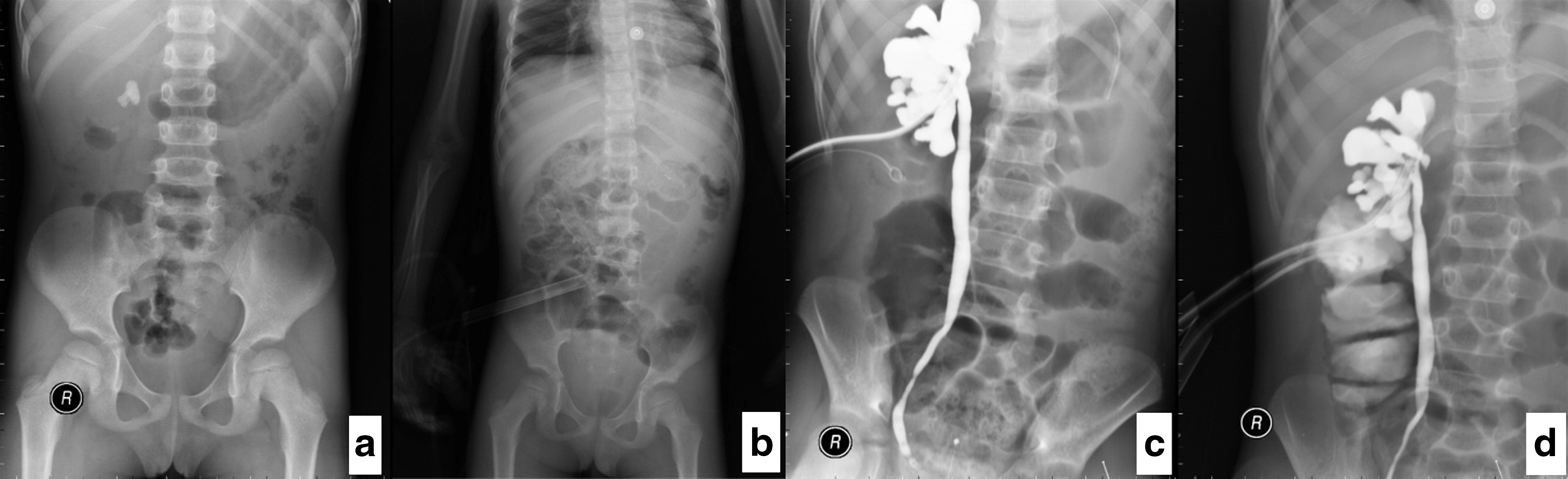
A 6-year-old child was referred to our clinic because of right flank pain. He was hospitalized for a 2.2 cm renal stone in the right ureteropelvic junction and grade 2 hydronephrosis (Fig. 1a). Because no pyuria was observed, PCNL was considered as the main treatment option. Hence, a 5F ureteral catheter was placed with a pediatric cystoscope. The tip of the catheter was extended to the kidney.
The patient was then placed in the prone position. The genitalia were covered with lead protection. The collecting system was punctured using a nephrostomy needle through which the guidewire was passed. The entrance of the guidewire to the ureter was observed on the fluoroscopy monitor. The access was dilated up to 20F using an Amplatz sheath. Later, the kidney was accessed using a nephroscope, and the guidewire was followed. Positioning of the guidewire in the colon was determined. A 16F Foley catheter was placed and its balloon inflated to 2 cc; contrast substance was flushed through the Foley catheter. The contrast liquid was seen in the colon but did not leak to the kidney. The same procedure for renal access was conducted again using a nephrostomy needle, guidewire, and dilation to 20F using Amplatz dilator. This time, renal access with the nephroscope was successful.
The stone was disintegrated with a pneumatic lithotripter, and the stone pieces were extracted with forceps (Fig. 1b). Then, a 10F Foley nephrostomy tube was placed. Antegrade pyelography was performed to evaluate the collecting system. The contrast liquid was observed to fill up the renal pelvis and pass from the kidney to the bladder under fluoroscopy. No contrast liquid transfusion between the colon and kidney was observed under fluoroscopy.
Ceftriaxone and metronidazole antibiotics were administered. A nasogastric catheter was inserted. The oral intake of the patient was stopped, and total parenteral nutrition was begun in the postoperative period. The patient's body temperature was 38°C on the first postoperative day, but no fever was seen in the following days. Antegrade pyelography was performed from the nephrostomy tube on the third day of the postoperative period (Fig. 1c). No fistula was seen between the colon and kidney (Fig. 1d). The contrast liquid passed to the bladder.
The nephrostomy catheter was removed on the third day. On the fifth day, oral intake was restarted. Afterward, the Foley catheter in the colon was withdrawn 1 cm, and on the eighth day, it was completely removed. The location from which the Foley catheter was removed was followed closely for possible colocutaneous fistula development. After removal of the Foley catheter, there was minimal drainage, which later stopped, and the patient was completely dry. The patient was discharged from the hospital 8 days after the PCNL intervention.
Discussion
Data regarding colon perforation during pediatric PCNL are quite scarce. Our survey of the relevant literature revealed only two cases. The first case reported was a 5-year-old girl; in that case, during PCNL for a stone in the left kidney, at the end of the dilation, it was noted that the guidewire had changed its position and entered the colon. 5 After removal of the kidney stone, a 12F nelaton catheter was placed into the colon using the guidewire to prevent bowel defect with controlled fistulization. The patient started oral intake after 48 hours. The bowel drainage catheter was removed 2 cm each day after the tenth day of the postoperative period. Fourteen days after the intervention, it was completely removed. At the fistula passage between the colon and the skin, a urostomy adaptor was inserted, and the patient was discharged with a urostomy bag. The fistula opening completely recovered after 2 weeks. The trauma was retroperitoneal and managed conservatively. 5
The other case was mentioned by Gedik and associates 6 while discussing the necessity of CT without providing in depth information regarding colon perforation during PCNL. The authors reported that they switched to open surgery after a colon perforation had occrured during their access to the kidney.
There are more reports regarding colon perforation during PCNL in adults compared with children. In the reports, conservative treatment options have been selected for early-detected retroperitoneal colon perforation management related to PCNL complications during the revisions. 7 –12 The basic assumptions underlying all these approaches are a very prompt diagnosis and retroperitoneal trauma. Otherwise, fecal pollution and related peritonitis might occur in intraperitoneal trauma. In our case, catheters were placed into the colon and kidney separately. The catheter inserted into the colon was removed after the formation of the colocutaneous fistula.
No drainage was evident in our case. We believe that prolonged catheter stay in the colon increases the possibility of fistula development. If the patient is not at sepsis risk, if bowel activity and fecal excrement continue, and if there is no evident leakage from the drainage in the colon, the removal of the inserted drainage in the colon earlier than 7 days can lead to earlier fistula improvement.
The factors increasing colon perforation risk during PCNL are advanced age of the patient, existence of horseshoe kidney, previous kidney surgery, inferior location access to the left kidney, lateral posterior axillary line access, and the existence of retrorenal colon. 7,9 In our case, the patient did not have any of the above-mentioned risk factors. The stone was located in the ureteropelvic junction of the right kidney. As in all children, in the present case, the right kidney stone was approached with standard renal access. Because the access did not slide laterally to the posterior axillary line, the present perforation during PCNL might stem from an anatomic variation of the colon. Abdominal CT is the most important visualization technique in determining anatomic variations of the colon. Because the patient was referred to our clinic with an intravenous urogram, we refrained from exposing the child to more radiation; hence, no abdominal CT was performed.
Although a variety of precautions can be taken to prevent colon perforation during PCNL, there is a wide variability in the three-dimensional (3-D) presentation of renal cavities. Thus, it is not easy to standardize a precise and reliable technique for every patient. 13 Ultrasonography-guided puncture might be used in the access to the kidney. 14 Another technique might be the use of CT-guided puncture to the kidney calix in cases with previously reported anatomic variations without inflicting harm to the other organs. 15 Furthermore, 3D CT, performed before PCNL procedures, provides excellent representation of this anatomy and allows a preplanning step; however, it does not show the relationship between the calices and the different organs, such as the colon in particular, and the kidney motion. 16 In the present case, because no indications pointing to colon perforation were evident, the routine PCNL procedure was applied.
Management of a single case is insufficient to set the standard; hence, a series of cases reported would be necessary. In our department, we first applied PCNL in adults; later on, with refinements in instrumentation and technology together with increased experience, PCNL has emerged as one of the standard treatment options in pediatric cases. Despite the fact that most steps applied during pediatric PCNL are similar to those with adults, there are differences in details because of the relatively small body size of children. In this patient, colon perforation had appeared for the first time, and we had to make an instant decision. We took advantage of the theoretical background knowledge earlier acquired and of our practical experiences; consequently, we decided to follow adult guidelines.
Conclusion
PCNL in children is rapidly becoming one of the most prevalent treatment options in urology clinics. Therefore, being aware of and well prepared for possible complications during and after PCNL interventions are of utmost importance. Among these complications, if retroperitoneal colon perforation is promptly recognized and strictly followed, conservative management is possible with the existing treatment options.
Footnotes
Disclosure Statement
No competing financial interests exist.