
Abstract
Introduction:
An aberrant crossing vessel(s) (CV) is considered an important cause of uretero-pelvic junction obstruction (UPJO) in adults. Intrinsic defect at the uretero-pelvic junction (UPJ) is not necessarily present and so, dismembered pyeloplasty would not be necessary. We introduce in the present study a novel technique, laparoscopic transposition pyelo-pyelostomy (LTP) to treat UPJO caused by aberrant CV in adults.
Patients and Methods:
From July 2004 to August 2010, 21 adult patients were diagnosed as having UPJO secondary to aberrant CV and were treated laparoscopically by transposition pyelo-pyelostomy. The main presentation was pain in 13 patients, while 3 patients presented with fever. Five patients were accidentally discovered as having hydronephrosis in ultrasound (U/S). Preoperative intravenous urography and U/S revealed grade III hydronephrosis in 11 patients and grade IV in 10 patients. Diagnosis of CV was suspected preoperatively in the IVU in 15 patients and was confirmed by computed tomography. The remaining six patients were diagnosed intra-operatively.
Results:
The operative time ranged from 75 to 125 minutes with a mean of 93 minutes. The mean time for anastomosis was 12 minutes. No intra-operative complication was reported. Drain was removed after 48 hours, and mean hospital stay was 3 days. Symptom improvement was encountered in all symptomatic patients. Postoperative US done at 3 months revealed resolution of the hydronephrosis in 10 patients, and 11 patients had a residual grade I hydronephrosis. Diuretic renography at 1 year postoperatively revealed normal T1/2 in 19 patients.
Conclusion:
LTP is a simple procedure that spares the normal UPJ and provides a wide, stentless anastomosis which nullifies the risk of re-stenosis and failure.
Introduction
Patients and Methods
From July 2004 to August 2010, 69 adult patients were diagnosed as having hydronephrosis secondary to UPJO in the Department of urology, Alexandria University. Diagnosis of CV as the cause of this UPJO was suspected preoperatively in the IVU in 19 patients and was confirmed by computed tomography. Another nine patients were diagnosed as having CV intra-operatively. This study was conducted on these patients in a prospective manner. All patients were scheduled for laparoscopic dismembered pyeloplasty (LDP). LTP was performed for 21 patients with UPJO secondary to CV, while intrinsic defect at the UPJ could not be excluded in the remaining seven patients with CV, so they were treated by LDP. Isotope diuretic renography was done preoperatively, showing an obstructed pattern with good renal function in all cases.
Under general anesthesia, all patients are placed in the flank position. Using a three port technique, a transperitoneal laparoscopic approach is performed. The UPJ is exposed with identification of the CV. The dilated pelvis is meticulously dissected away from the vessel(s). With the UPJ and the pelvis away from the CV, the patency of the UPJ is initially anticipated by the normally looking ureter and the rapid drainage of the full renal pelvis once the vessel(s) is pulled away from the compression site. This is further tested by filling the collecting system with saline injected using 22-gauge Chiba needle placed percutaneously into the renal pelvis with a filling rate of 10 mL/minute. As the renal pelvis distends with saline, we observe proper drainage through the UPJ, propagation of peristaltic waves from the pelvis down to the ureter, and the constant flow of saline all though the test. Once the patency of the UPJ is confirmed, the pelvis is transected 2 cm above the UPJ, transposed to the opposite side of the CV, and then re-anastomosed. Anastomosis is performed by 5/0 vicryl suture in a continuous running manner with only one knot at the beginning and another one at the end (Fig. 1). No DJ stent is placed after this wide, water tight anastomosis. A closed suction drain is placed and later removed once drainage is stopped.

Diagrammatic illustration of transposition pyelo-pyelostomy.
Patients were followed up after 3 months for symptom assessment and resolution (or significant reduction) of hydronephrosis by U/S. At 1 year postoperatively, all patients had U/S and diuretic renography. Patients were followed up thereafter annually by U/S.
Results
Of the 28 adult patients diagnosed with UPJO secondary to aberrant lower pole CV and planned to undergo LTP, intrinsic defect at the UPJ could not be excluded intra-operatively (by the saline filling test) in seven patients, and LDP was performed for them. The remaining 21 cases underwent LTP. Thirteen patients were women, and 8 patients were men. Age ranged from 14 to 47 years with a mean age of 25 years. The main presentation was flank pain in 13 patients, while 3 patients presented with microscopic haematuria. Five patients were accidentally discovered as having hydronephrosis in U/S. Preoperative IVU and U/S revealed grade III hydronephrosis in 11 patients and grade IV in 10 patients.
The operative time ranged from 75 to 125 minutes with a mean of 93±12 minutes. The mean time for anastomosis was 12 minutes (ranged from 6 to 19 minutes).None of our patients had a severely dilated renal pelvis that required reduction though we feel that, if needed, it would be easily performed. No intra-operative complications were reported, and conversion to open surgery was not needed. Minimal urine leakage from the drain was encountered in eight patients, and the drain was removed after a maximum of 48 hours. Hospital stay ranged from 2 to 5 days with a mean stay of 3 days. Follow-up period ranged from 13 to 66 months with a mean follow-up of 27 months.
Symptom improvement was encountered in all symptomatic patients. Postoperative U/S done at 3 months revealed resolution of the hydronephrosis in 10 patients (Fig. 2), and 11 patients had a residual grade I hydronephrosis. Diuretic renal scintigraphy at 1 year revealed improved drainage in 19 patients with mean T1/2 of 11±2.4 minutes, with delayed drainage (T1/2 of 16 and 19 minutes) in two patients who were symptom free. Mean split function of the affected kidney improved from 33%±5.4% to 39%±4.6% 1 year postoperatively.
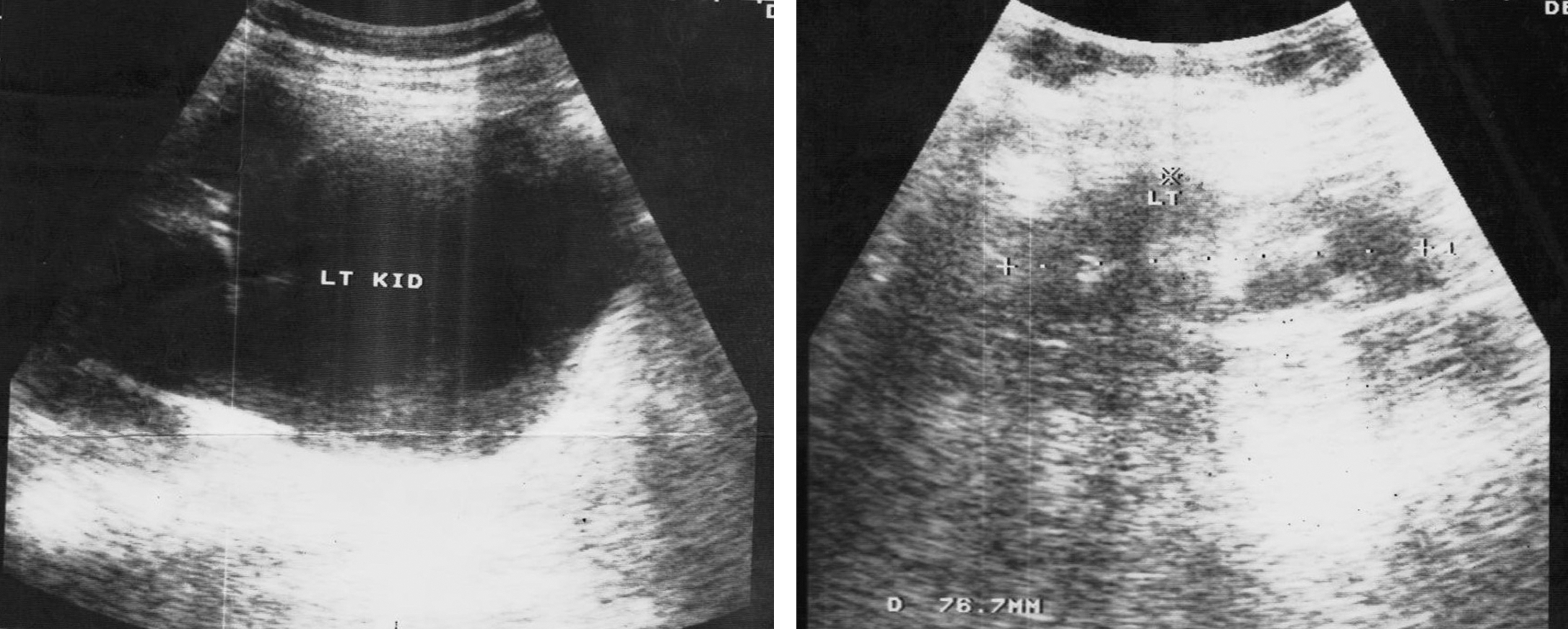
Pre- and postoperative ultrasound of a female patient.
Discussion
CV represent at least 40% of cases with primary UPJO in adults. 1 Based on the assumption that intrinsic defect is always present at the UPJ, DP is the main technique used to treat all UPJO pathologies even for the cases with CV. 6
This is not always the case, and there are a good number of studies that suggest the absence of intrinsic defect in the UPJ segment on histological, physical, and clinical bases. Histologically, Richstone et al demonstrated normal UPJ in adult cases with UPJO and CV treated with LDP. 7 In their study, CV were present in 63.2% of cases, and the most common UPJ histologic finding in these patients was “no intrinsic abnormality.” Physically, evidence was reported by Stern et al, who demonstrated a significant decrease in the renal pelvic pressure by Whittaker test after vascular repositioning of the CV. Mean intra-renal pressure dropped from 25.6±4.5 to 9.5±6.6 cm H2O. 8 The successful outcomes of the Hellström vascular relocation technique, which is done by open surgery 9 and laparoscopy, 5,10,11 gave clinical proof for the absence of concomitant intrinsic defect in cases of UPJO with CV. Similarly, fixing the renal pelvis away from the vessel as in the Pyelopexy performed by Emond and Samson 12 further supports the absence of concomitant intrinsic defect in these cases. This may question the necessity of excising the normal UPJ while treating these cases.
On the other hand, DP, especially when performed laparoscopically, is a tedious procedure that entails manipulation of the narrow and delicate proximal ureter which may lead to edema and devascularizatoin of the periureteric tissues resulting in secondary fibrosis and stenosis. Intracorporeal suturing and knotting add to the trauma of this delicate ureter and also prolong the operative time that is reported to range from 119 to 246 minutes. 13 –16 Ureteral trauma can be expected to be more, and operative time can be much longer if the operator is still in his early laparoscopic experience.
The idea behind this new technique of LTP is to avoid the presumed difficulties and complications of the DP as long as there is no need to harm the normal UPJ segment. In this technique, a very wide pelvic anastomosis is done, avoiding the possibility of stenosis and failure that is reported in up to 12% in the large LDP series. 13 –16 No ureteric stent is placed in this procedure, because the anastomosis is obviously wide. This avoids the common stent complications including bladder irritation, flank pain and stent migration and saves another hospital admission for stent removal. In addition, a watertight tension free anastomosis is easily performed that minimizes urine leakage and secondary peri-pelvic fibrosis. Suturing the two pelvic ends does not necessitate the use of fine sutures and is not as demanding as in DP; thus, it saves time with a mean operative time of 93±12 minutes. This can be very helpful for laparoscopy beginners.
Other techniques avoided manipulating the UPJ and depended on separating the UPJ from the CV either by vascular mobilization to a cephalad position as in Hellström procedure 9 or by pyelopexy 12 performed by Emond lack long term follow-up. Recurrence of compression and obstruction by the CV may occur due to sagging of the pelvis above the mobilized vessel. In the present technique, we transect the pelvis and reposition it to the opposite side of the vessel(s) reproducing the concept of UPJ/vascular separation with no chance for pelvic kink over the transposed vessel, thus avoiding the chance of recurrence and failure.
The key point in this procedure is to satisfactorily confirm the absence of intrinsic obstruction concomitantly with the aberrant CV. We combine the subjective evidence of normally looking ureter and prompt emptying of the distended renal pelvis after vascular separation with the objective evidence of the saline filling test. When in doubt, a dismembered procedure should be performed.
Conclusion
We present our experience with LTP, a novel technique for treating adult cases with UPJO secondary to extrinsic compression by CV. It is a simple procedure that combines the radical correction of the cause of obstruction with the easier, wide, and failure-proof anastomosis of the transposed renal pelvis.
Footnotes
Disclosure Statement
No competing financial interests exist.