
Abstract
Background and Purpose:
Holmium laser enucleation of the prostate (HoLEP) is a recognized option for surgical management of benign prostatic hyperplasia (BPH). While laser parameters and enucleation techniques have been widely investigated, morcellation techniques remain poorly evaluated in the literature. Our goal was to objectively evaluate the available devices used for morcellation during HoLEP.
Material and Methods:
An in vitro evaluation of two morcellators (Lumenis and Wolf) and two nephroscopes (Wolf and Storz) was conducted. For morcellators, the following parameters were assessed: Aspiration power (time to aspirate 1 L of water), morcellation power (g of baked chicken meat morcellated in 2 minutes), and visual control of the cutting part of the device (visible or not visible). For nephroscopes, data collected were: Field of vision (measured on a 4 cm distant sight) and irrigation flow (time needed to drain a 3-liter bag of water suspended at 1 m of height).
Results:
For the Wolf and Lumenis morcellators, aspiration power parameters were 20.4 mL/s and 22.2 mL/s, and morcellating power parameters were 2.5 g and 6 g of tissue per minute, respectively. The cutting part of the Wolf morcellator was permanently under control during the procedure, whereas the distal part of the cutting device was out of vision control with the Lumenis. Evaluation of Storz and Wolf nephroscopes showed that field of vision was larger with the Storz, and irrigation flow was 0.35 and 0.52 L/min, respectively.
Conclusions:
The Storz nephroscope has a greater field of vision but less important blood flows. The Lumenis morcellator is faster than the Wolf morcellator. These objective data could set up the basis for a prospective trial comparing the two devices.
Introduction
B
The technical aspects of HoLEP technique have been largely studied and reviewed, 8 –10 but most of them are focused on the enucleation part of the procedure and/or laser parameters. To our knowledge, the second part of the surgical procedure consisting of intravesical morcellation of the enucleated prostatic tissue remains poorly evaluated in the literature. This step, however, is crucial during HoLEP for at least two reasons. First, morcellation is a source of morbidity because bladder injury is possible by the morcellator, 11 contrary to other transurethral procedures. Second, morcellation lengthens the duration of the procedure and thus impacts its time efficiency. Furthermore, morcellation duration and complexity are linked to the weight of prostate tissue removed by enucleation. Given that many reports advocate for HoLEP efficiency in large prostates, 11,12 optimization of morcellation is mandatory during the procedure.
Contrary to enucleation, morcellation has not been a source of multiple innovations. Like in the initial description of the technique, 13 morcellation is conducted by using a nephroscope, permitting the introduction of a morcellator in the bladder. Morcellation is performed with an ergonomic morcellator specially designed and under endoscopic view that must be perfect to limit bladder injuries. Two types of nephroscopes (produced by respectively Storz and by Wolf), and two morcellators (produced by Lumenis and Wolf) are available. To date, the objective performances of these devices, which partly condition the result of the procedure, have not been studied. Our goal was to assess the technical specificities of these two devices to bring reliable information to urologists for daily practice.
Materials and Methods
An in vitro evaluation of two morcellators (VersaCut,™ Lumenis Incorporated, Santa Clara, CA, and Piranha,™ Richard Wolf GmbH, Knittlingen, Germany), and two nephroscopes (Richard Wolf GmbH, Knittlingen, Germany and Karl Storz, Tuttlingen, Germany) was conducted to assess their objective performances and comfort of use. The devices are shown in Figures 1 and 2.
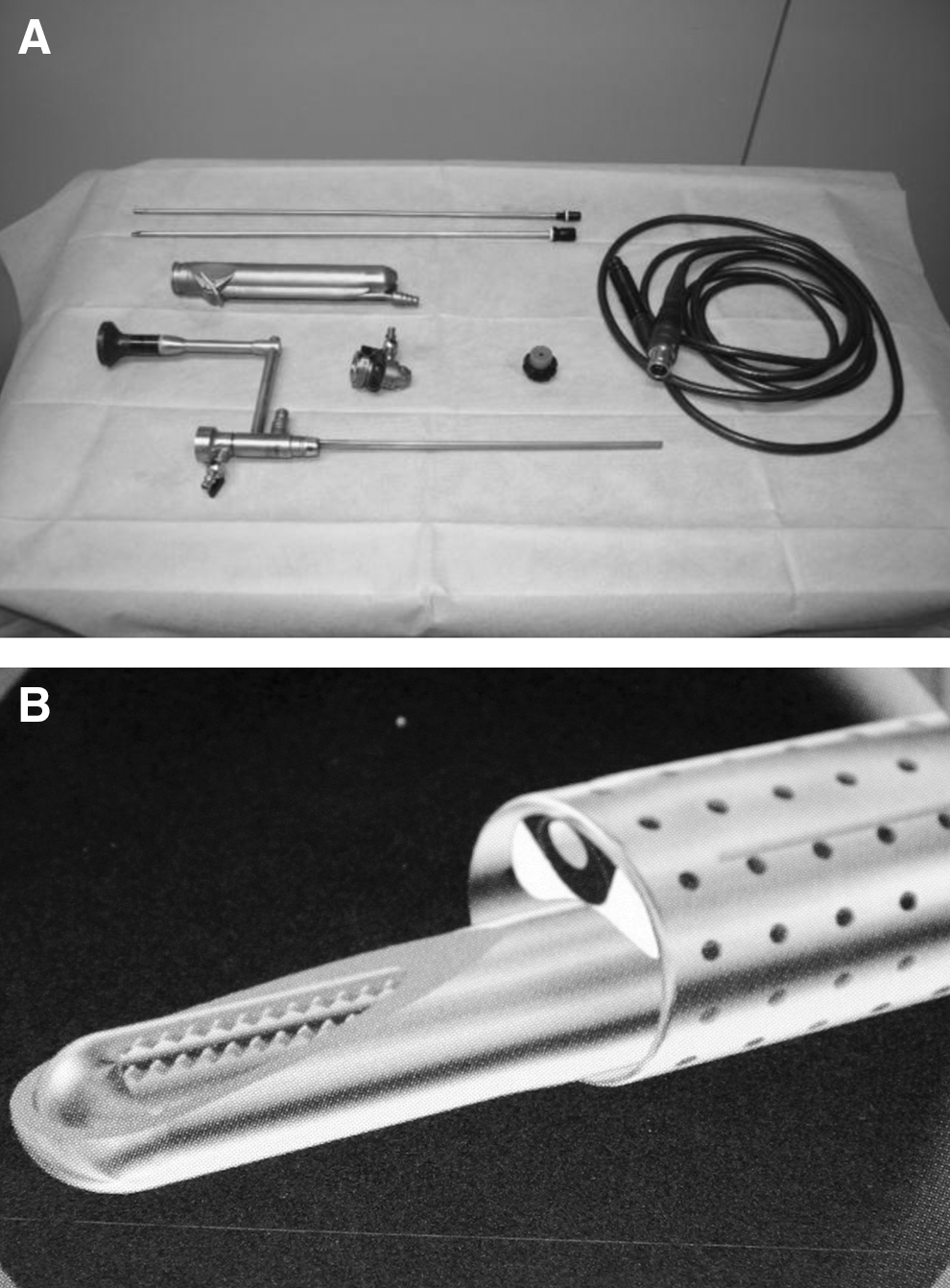
The Wolf device.
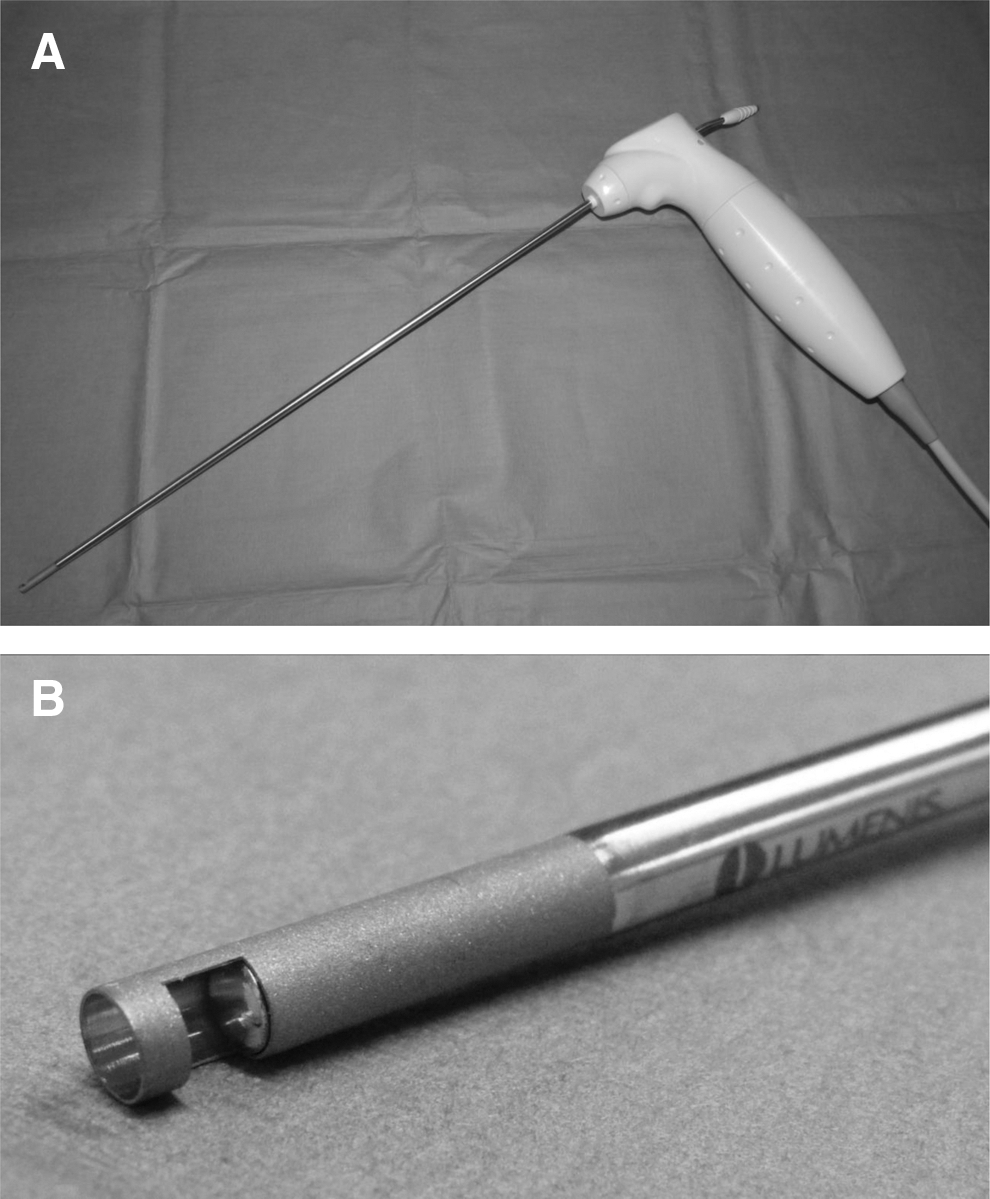
The Lumenis device.
The tests were conducted separately for nephroscopes and morcellators. For nephroscopes, data collected were field of vision and irrigation flow. Field of vision was evaluated by looking through the nephroscope on a sight placed perpendicularly 4 cm in front of the end of the scope. The irrigation power was evaluated by assessing the time necessary to drain a 3-L water pouch suspended 1 m over the device.
For morcellators, three parameters were assessed: Aspiration power (time to aspirate 1 L of water), morcellation power (g of baked chicken meat morcellated in 2 minutes), and visual control of the cutting part of the device (visible or not visible). Aspiration power was defined as the time necessary to aspirate 1 L of water. Morcellation power was assessed by measuring the weight of tissue morcellated in 2 minutes. The model was a piece of chicken baked for 10 minutes in a microwave oven at 300 W power to obtain a shape and consistency similar to prostatic tissue. During this procedure, visual control of the cutting part of the device was evaluated and stated as complete (permanent visual control of the cutting part) or incomplete (if the cutting part disappeared in the tissue during morcellation).
Results
Nephroscope evaluation showed that the field of vision through the Storz device was largely greater than through the Wolf device (areas reproduced on the sight are shown in Fig. 3). The area of the field of vision was approximately two times greater with the Storz device. Irrigation flows were 0.35 and 0.52 L/min for the Storz and the Wolf devices, respectively.

Fields of vision obtained with the two devices.
Morcellator evaluation showed that aspiration power was 49 and 45 s/L for the Wolf and Lumenis morcellators, respectively. Morcellating power evaluation showed that 5 g of tissue was morcellated in 2 minutes with the Wolf device, compared with 12 g of tissue in 2 minutes with the Lumenis device. The cutting part of the Wolf morcellator was still under control during the procedure, whereas the distal part of the cutting device was partly out of vision control with the Lumenis.
Discussion
HoLEP is now a technique in widespread use for surgical management of BPH. Indeed, this procedure has proven to be efficient in almost all cases, even in the case of high prostate volume. 12 Several technical modifications have been published after the first reports at the end of the 1990s. 9 Numerous publications studied the influence of the surgical devices, the characteristics of the laser used, the learning curve, and the outcome of the technique, but few reports concern morcellation devices. 14 This time-consuming step of the procedure has to be optimized to save time and reduce incidence of adverse events. However, this phase of the procedure, however, relies mostly on the morcellator equipment, so that comparative studies of available devices could be useful.
In the present study, we have evaluated independently, without any funding or potential conflict of interest, in vitro performances of the devices available on the market. We checked separately the parameters of the nephroscopes and the morcellators devices that can be used for HoLEP.
About scopes, irrigation flow and field of vision strongly determine the practitioner's comfort during the morcellation procedure that can be impacted by a reduced field of visual control, a blurred image because of bleeding and/or insufficient turnover of the intravesical fluids. The Storz nephroscope had a greater field of vision than the Wolf and had an acceptable irrigation power if double irrigation can be used. The Wolf nephroscope, however, can be used alternatively with the morcellation system, thus permitting a gain in time during the procedure.
About morcellators, a fine balance has to be found between morcellation speed and safety of use. While the Lumenis morcellator appeared to be very fast, the end of the cutting part of the device went systematically out of direct vision during our experiments. In our study, the number of grams morcellated in 2 minutes favorably compared with constructor data that mention an approximate 7 g/min morcellation speed. 15 The Wolf morcellator was shown to be safe with a permanent view on the cutting device, an advantage presented by the constructor of the device 16 (Fig. 1). The morcellation speed is not mentioned by the constructor on the official website.
The limit of our study is that it cannot be strictly translated to clinical practice because it was performed ex vivo. To overcome this experimental view, a prospective clinical trial comparing the two devices should be performed to compare both efficacy outcome and clinical data linked to the release of obstruction. This comparative evaluation, however, gives an idea of the performance of the two devices that, to our knowledge, has not been previously described in the available literature. It provides an independent basis to set the goal of a future comparative study. Furthermore, another important issue for clinical practice is the cost of these devices that needs to be compared in terms of initial cost and successive purchase of single parts and accessories.
Conclusions
Our results suggest that the Storz nephroscope harbors the best field of vision during the morcellation process during HoLEP and can bring a good flow level in the bladder if double irrigation is available. The Lumenis morcellator appeared to be faster than the Wolf device, but the cutting part of the device was permanently under control with the Wolf device that was not the case with the Lumenis. These primary objective data could help to set up a comparative trial comparing the two devices in terms of results, complications, and cost-effectiveness.
Footnotes
Disclosure Statement
No competing financial interests exist.