
Abstract
Purpose:
We conducted a randomized controlled trial to assess the efficacy of nephrostomy tract infiltration with bupivacaine in tubeless percutaneous nephrolithotomy (PCNL).
Patients and Methods:
All adult patients undergoing unilateral tubeless PCNL from July 1, 2007 to October 31, 2007 were included in the study. Patients were randomized to receive infiltration of bupivacaine in the nephrostomy tract at the end of the procedure or not to receive bupivacaine. To show a 10% difference in postoperative pain, a sample size of 30 persons per group would be needed. Postoperatively, the pain score were obtained at 4 and 24 hours by a nurse who was blinded to the protocol. The perioperative outcome of these patients (study group) was compared with those undergoing tubeless PCNL without nephrostomy tract infiltration of bupivacaine (control group).
Results:
Patient demographics and intraoperative parameters in both groups were comparable. Supracostal access was needed in 65.7% and 72.7% patients in the study and control group, respectively. The nephrostomy tract were infiltrated with bupivacaine in 31 patients. The visual analogue pain score at 4 hours and 24 hours for the study group was 2.66±1.07 & 2.23±0.50 respectively, while in control group was 5.15±1.52 and 3.22±1.11, respectively (P=0.000). There was a trend toward lesser analgesia requirement in the study group (94.8 vs 124.2 mg of diclofenac sodium). There was no difference in the duration of postoperative catheterization, hospital stay, stone-free rates, and complication between both groups.
Conclusions:
Nephrostomy tract infiltration of bupivacaine in tubeless PCNL is associated with less postoperative pain and analgesia requirement.
Introduction
In the urologic literature, there are no standard guidelines on postoperative pain management after PCNL. Various options include use of narcotic or nonnarcotic analgesics, patient-controlled analgesia pumps, single-dose subarachnoid spinal anesthesia, and/or local infiltration of anesthetic agents. 5 –9 Subcutaneous infiltration of local anesthetic agents with or without infiltrations into the nephrostomy tract, renal parenchyma, and/or renal capsule has been shown to decrease early postoperative pain and analgesia requirement after standard PCNL. 5 –8
In the present study, we combined both the above refinements in PCNL to make the procedure more pain free. It was our hypothesis that infiltration of the nephrostomy tract with local anesthetic agent could further decrease the patient-reported pain and narcotic use after tubeless PCNL. Hence, we conducted a randomized controlled trial to assess the efficacy of nephrostomy tract infiltration with bupivacaine on these parameters after a tubeless PCNL. To our knowledge, this is the first study that examines the impact of infiltration of the nephrostomy tract with local anesthetia after tubeless PCNL. We also reviewed all the available literature to know the present role of local anesthetic infiltration for postoperative pain management after PCNL.
Patients and Methods
Participants
From July 1, 2007 to October 31, 2007, all patients needing PCNL for large renal and/or upper ureteral calculi were invited to participate in the study irrespective of number and size of stone, associated hydronephrosis, and/or renal insufficiency. Exclusion criteria for the study are given in Table 1. Patients needing a supracostal access were not excluded from the study. Preoperative patient evaluation included medical history, physical examination, urine culture, serum creatinine determination, sonography of urinary system, and intravenous urography. The data on preoperative pain and analgesic use was not available for analysis. Radiography of the kidneys, ureters, and bladder (KUB) was performed in patients with raised serum creatinine levels. All patients gave informed consent for the procedure. Flow of participants with details of excluded patients is shown in Figure 1.
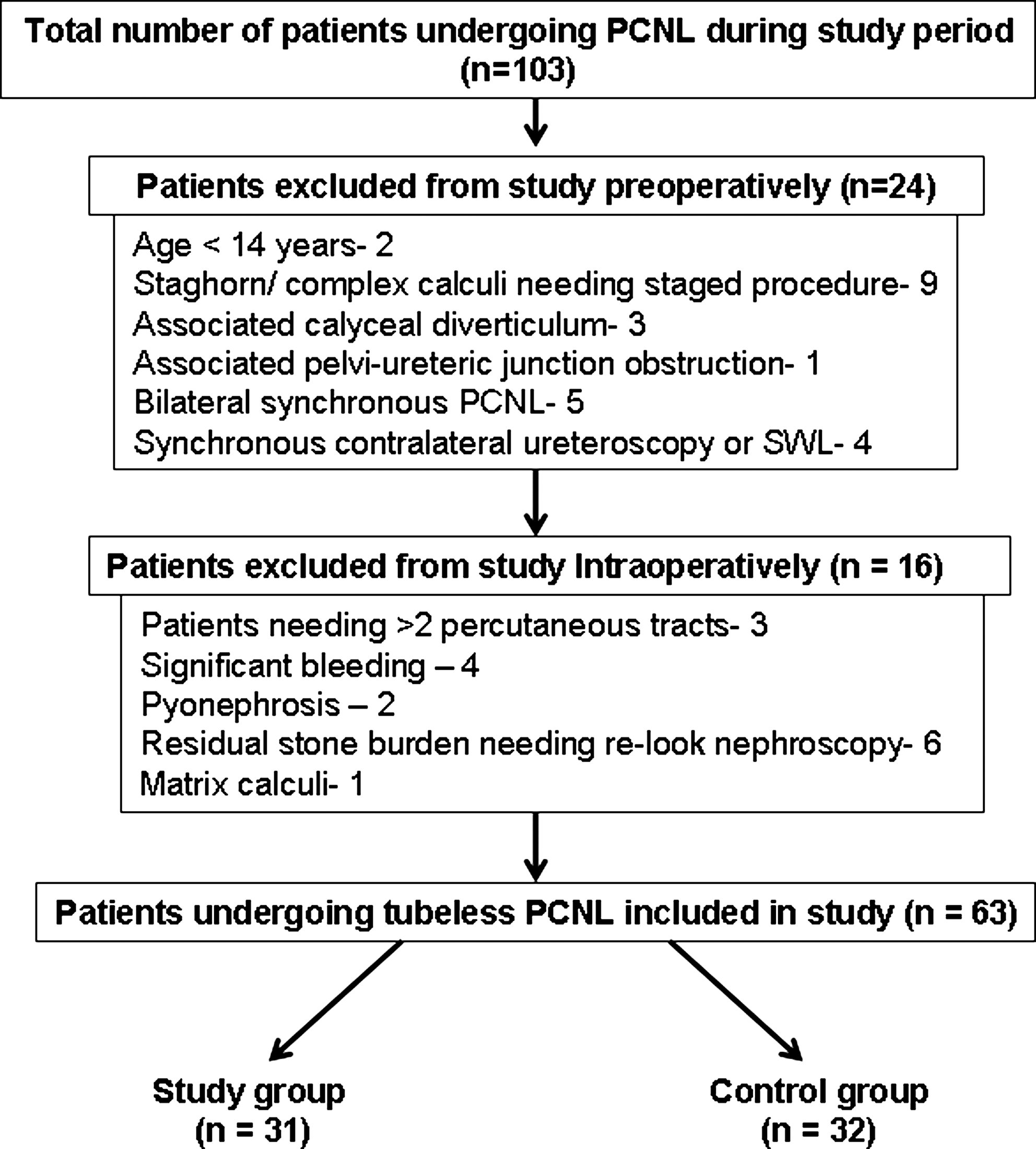
Flow of participants during study period.
Intervention
All PCNL were performed under general anesthesia by a single urologist (HNS). Percutaneous access was gained using an 18-gauge initial puncture needle under fluoroscopic control. A 0.038″ J-tip guidewire was parked in the pelvicaliceal system. Further tract dilation was performed using sequential telescopic metal dilators. A 30F Amplatz sheath was positioned in the collecting system. After initial nephroscopy, stone fragmentation was achieved with pneumatic lithotripsy, and fragments were then mechanically removed with grasping forceps. Flexible nephroscopy and/or additional tracts were used as and when necessary. After ensuring complete intraoperative stone clearance with fluoroscopy and endoscopy, a 6F Double-J stent was placed in an antegrade manner.
In the patients from the study group, 1.5 mg/kg of 0.25% bupivacaine was infiltrated with a 23-gauge needle circumferentially around the Amplatz sheath subcutaneously and in the parietal wall under fluoroscopic guidance to confirm that the needle depth matched the depth of the Amplatz sheath. No attempt was made to actively close the skin incision, and the wound was strapped with a tight occlusive dressing. In the control group, the Amplatz sheath was removed without any local infiltration of anesthetic agent, and a similar type of dressing as in the study group was applied. Because the procedure was performed under anesthesia and patients and the staff nurse evaluating postoperative pain were not aware of the local infiltration of bupivacaine, we think that there was no bias involved in the study.
Postoperative care and follow-up
The visual analogue scale was used to assess pain 4 hours after surgery and on postoperative day 1. It was not assessed more frequently in the present study. A staff nurse who was blinded to the randomization results obtained the pain score. Postoperative pain management was performed with 75 mg intramuscular diclofenac sodium or 50 mg tramadol hydrochloride as and when demanded by the patients. Hemoglobin estimation was performed on postoperative day 1. A chest radiograph was obtained in patients who needed supracostal access. Stone-free status was confirmed on postoperative day 1 with the help of KUB radiography and sonography of the urinary system. Patients were informed about findings of these imaging procedures; however, the effect of residual fragments on postoperative pain was not separately studied. Patients were discharged after removal of the urethral Foley catheter usually on postoperative day 1, once hematuria cleared.
The above radiologic investigations were repeated during follow-up at 1 to 2 weeks before stent removal. Success was defined as the patient being completely stone free or having a residual fragment ≤4 mm on the above investigations. Patients with larger residual stone fragments were subjected to shockwave lithotripsy before stent removal.
Study design
Objective
To test the hypothesis that “patient-reported pain and narcotic use could be further decreased after tubeless PCNL if the nephrostomy tract is infiltrated with local anesthetic.”
Sample size
A sample size of 30 persons per group was needed to show a 10% difference in postoperative pain score and analgesic requirement with a power calculation using [alpha]=0.05 and [beta]=0.20.
Randomization and blinding
A balanced block randomization process with block size of six patients was used for randomization. When a patient met all the criteria for a tubeless procedure at the end of PCNL, a sealed envelope was opened by a research fellow (RHS) to allocate the patient to either group. All patients and the staff nurses evaluating postoperative pain were blinded in our study.
Statistical methods
The Statistical Package for the Social Sciences (SPSS, version 12.0) was used to enter patients' demographic and perioperative data. Quantitative variables were analyzed using means (±standard deviation), and the independent sample t test (two-tailed) with 95% confidence interval was used to study the outcome between both groups. The chi-square test was used for the analysis of qualitative data that were expressed in the form of ratio. A P value<0.05 was considered statistically significant.
Results
During the study period, 103 patients underwent PCNL at our institute. Of these, 31 patients in the study group and 32 patients in the control group were available for analysis (Fig. 1). Patient demographics and intraoperative parameters in both groups were comparable (Table 2). The mean numbers of tracts needed in the study and control groups were 1.13±0.34 and 1.10±0.17, respectively. Supracostal access was needed in 65.7 % patients in the study group and 72.7 % patients in the control group.
Chi-square test.
SD=standard deviation; VAS=visual analogue scale.
The visual analogue pain score at 4 hours and 24 hours for the study group was 2.66±1.07 and 2.23+0.50, respectively, while in the control group it was 5.15±1.52 and 3.22±1.11, respectively (P=0.000). There was a trend toward lesser analgesic requirement in the study group (94.8 vs 124.2 mg of diclofenac sodium). The difference, however, was not found to be statistically significant. There was no difference in the duration of postoperative catheterization, hospital stay, stone-free rates, and complications among the groups (Table 3).
The difference is statistically insignificant by chi-square test.
Few patients had more than one complications.
SWL=shockwave lithotripsy;postop=postoperative; AV=arteriovenous.
One patient in the control group had a preoperative hemoglobin value of <9 g/dL and needed blood transfusion postoperatively. Postoperative septicemia did not develop in any patient in either group and no patient needed angioembolization. One patient in the study group with staghorn calculus needed a supracostal tract through the 10th intercostal space. This male patient developed postoperative hydrothorax that needed drainage. Another patient in the control group had obliteration of the costophrenic angle on postoperative chest radiography, which was suggestive of hydrothorax that was managed conservatively.
A 67-year-old patient with diabetes, atherosclerosis, and ischemic heart disease was receiving antiplatelet medication. His antiplatelet medications were withheld for 5 days, after which he underwent tubeless PCNL with instillation of bupivacaine in the nephrostomy tract. On postoperative day 1, upper limb monoparesis developed. He was transferred to the intensive care unit and was given low-molecular weight heparin, after which he recovered in 48 hours.
No patients in either group had postoperative urine leakage or urinoma. Success rates are summarized in Table 3. At 3-month follow-up, three patients in the study group and two in the control group had residual fragments <4 mm on either radiography and/or sonography. They are receiving medical management for the fragments.
Discussion
Of all the minimally invasive and noninvasive treatment options that are available for renal calculi, PCNL appears to be the most invasive. It is not completely devoid of postoperative pain. It is the fear of this pain that contributes to patient anxiety before the procedure. 8 To know the current status of post-PCNL pain management, we reviewed the literature and identified five articles that evaluated the role of local infiltration of anesthetic agents in post-PCNL pain managment (Table 4).
- P<0.001
SP=local infiltration of normal saline and intravenous paracetamol infusion; LP=local infiltration of levobupivacaine and intravenous paracetamol infusion; LS=local infiltration of levobupivacaine and intravenous saline infusion.
In today's era, postoperative pain management should be considered an integral part of patient care. Andreoni and colleagues 9 addressed this issue for the first time in 2002. In a randomized trial, the authors noted that a single preoperative dose of subarachnoid spinal analgesia with morphine along with infiltration of the nephrostomy tract with bupivacaine was associated with a statistically significant decrease in the requirement of postoperative parenteral pain medication. Although the authors did not encounter any major complications in their study, they did mention the potential drawbacks of intrathecal administration of morphine. These include the possibility of respiratory depression, sedation, nausea, and vomiting. The remote possibility of these complications and the need for additional subarachnoid injection are the possible factors that limit widespread acceptance of this method in the urologic community.
Ugras and coworkers 5 studied the effect of postoperative pain on pulmonary functions after PCNL. They noted restricted ventilation secondary to pain after PCNL. To avoid possible complications of opiod use, the authors used multimodal pain management consisting of instillation of the local anesthetic ropivacaine and parenteral administration of metamizol on postoperative days 1 and 2. They noted better pain control and decrease analgesic requirement when ropivacaine instillation was combined with metamizol as compared to use of metamizol alone. This multimodal pain management strategy also improved pulmonary function after PCNL.
Keeping in mind various studies in other specialties such as general surgery, gynecology, and anesthesia describing the efficacy of local anesthetic infiltration in surgical incisions, Haleblian and associates 6 conducted a randomized controlled trial to assess the efficacy of the subcutaneous infiltration of bupivacaine at the nephrostomy site after PCNL. They also provided a brief description of the pharmacology of bupivacaine in their article. Because a small size nephrostomy tube was associated with less postoperative pain, the authors used a 10F nephrostomy tube in their patients. Although narcotic requirement decreased in the study group, the difference was not found to be statistically significant.
Møiniche and colleagues 10,11 found similar findings in a systematic review. In this review, postoperative pain scores, time to first analgesia demand, and total analgesic requirement were compared in patients in whom the incision site was infiltrated with local anesthetic after cholecystectomy, abdominal hysterectomy, inguinal hernia, and various abdominal surgeries. It was found that local anesthetic to the incision site yielded effective analgesia for a 2 to 7 hour period only for inguinal hernia operations. Thus, effective postoperative analgesia could not be achieved for other types of surgeries.
Dalela and coworkers 12 emphasized that “most of the pain at the time of PCNL is experienced during dilatation of the renal capsule and the parenchyma as it is richly innervated by pain-conducting neurons.” 12 They presented a series of PCNL performed using their technique of local anesthesia that included a renal capsular block. Adapting a similar hypothesis, Jonnavithula and colleagues 7 infiltrated 20 mL of 0.25% bupivacaine, under fluoroscopy guidance, with a 23-gauge spinal needle (10 cm length) along the nephrostomy tube at 6 o'clock and 12 o'clock positions (10 mL in each tract), including renal capsule, muscles, subcutaneous tissue, and skin. It was their assumption that all these structures contribute to development of postoperative pain. In a randomized controlled study, they found their technique to be associated with significant reduction in pain scores and analgesic requirement without any complications.
Contrary to the above findings, Gokten and associates 8 infiltrated 20 ml of 0.25% levobupivacaine through the entire nephrostomy tract, which included skin, subcutaneous tissue, and muscles, just before puncture of PCNL. In spite of using preemptive analgesia, they failed to show any major advantage of local anesthetic infiltration over a saline infiltration. Only when they combined intravenous infusion of paracetamol with local infiltration of levobupivacaine, they found lower postoperative pain scores and opiod requirement. The lack of efficacy of the local infiltration of levobupivacaine alone in reducing postoperative pain can be explained by the fact that local anesthetic infiltration was performed before making a puncture for PCNL. Hence, there is a possibility that the final PCNL tract may not pass through the initial local anesthetic injection site. Similarly, the exact depth of infiltration and the method of infiltration are not mentioned by the authors. It is a theoretical possibility that the renal capsule and deeper muscles layers may not be infiltrated by local anesthetic.
It is generally accepted that patients who need supracostal access are more likely to have postoperative pain and need more analgesics than those who need infracostal access. In the present study, 74.6% of patients had supracostal access (Table 2). We have not performed any subgroup analysis to see whether infracostal vs supracostal PCNL pain control would make the results different. This issue, however, is subject matter of future studies.
In the present study, we attempted local infiltration of the nephrostomy tract, including the renal capsule, under fluoroscopy guidance in patients undergoing tubeless PCNL. Because this was performed with the Amplatz sheath in place, we believe that the local anesthetic drug would have had its effect even on the renal capsule and deeper muscle layers. To our knowledge, this is the first study using this method for postoperative pain management in tubeless PCNL. Because nephrostomy tubes are the potential cause of postoperative pain and discomfort, we avoided the same in the present study.
In addition, we infiltrated the nephrostomy tract with bupivacaine to minimize pain resulting from tissue trauma occurring during PCNL. We noted that nephrostomy tract infiltration with bupivacaine is highly effective and a safe technique of postoperative pain management for patients undergoing tubeless PCNL. From the literature review, it is still not clear whether local infiltration of an anesthetic agent should be reinforced with additional measures to minimize postoperative pain and opiod requirement, especially in patients undergoing standard PCNL with insertion of a nephrostomy tube at the end of the procedure.
Since 2005, we started performing tubeless PCNL by replacing the postoperative nephrostomy tube with indwelling ureteral stents. As proposed by Zilberman and coworkers, 13 it has now become a standard of care in our practice. We are now routinely infiltrating nephrostomy tracts with bupivacaine postoperatively in all our patients undergoing PCNL—either tubeless or standard procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.