
Abstract
A Double-J stent may be used for ureteral injury because of a gynecologic procedure. Intravascular migration of a Double-J stent into the inferior vena cava as an uncommon complication of ureteral stent placement is reported. Percutaneous removal of the migrated stent was performed through the left femoral vein under angiographic and fluoroscopic guidance.
Introduction
Case Report
A 52-year-old woman with uncontrolled abnormal uterine bleeding underwent total abdominal hysterectomy 35 days before referral to our department. Ten days after operation, she experienced true urinary incontinence. Intravenous urography revealed iatrogenic left ureteral obstruction and hydroureteronephrosis. Although cystoscopy, left ureteroscopy, and ureteral Double-J stent placement were performed 15 days after surgery, urinary incontinence continued and gross hematuria occurred in this patient. On cystoscopy, the lower end of the Double-J stent was not seen, and stent location was indefinite on radiography of the kidneys, ureters, and bladder (KUB). Because of migration of ureteral stent to an unknown location, she underwent explorative laparotomy. Identification, reimplantation, and Double-J stent placement in the left ureter was performed during surgery. The previous Double-J stent was not found, and she was referred to our center for specialized management.
The patient had normal vital signs and body temperature, mild tenderness of the previous surgical scar, and normal laboratory test results except for hematuria and decreased red blood cells indices. KUB radiography exhibited right-side deviation of the migrated stent (Fig. 1). Ultrasonography specified an intravascular position of the Double-J stent. Noncontrast spiral CT scan revealed two Double-J stents (Fig. 2). One stent was in the left-side urinary system and the ectopic stent was in the venous vascular system. The lower end of the migrated stent was located in the left external iliac vein, the main part of the stent was in the inferior vena cava (IVC), and the upper end of the stent was located next to the right atrial inlet (Fig. 3). Venography of the iliac veins and IVC confirmed the location of the stent. Percutaneous removal of the migrated Double-J stent was performed through the left femoral vein by grasping the lower end of the stent under angiographic and fluoroscopic guidance and local anesthesia (Fig. 4).
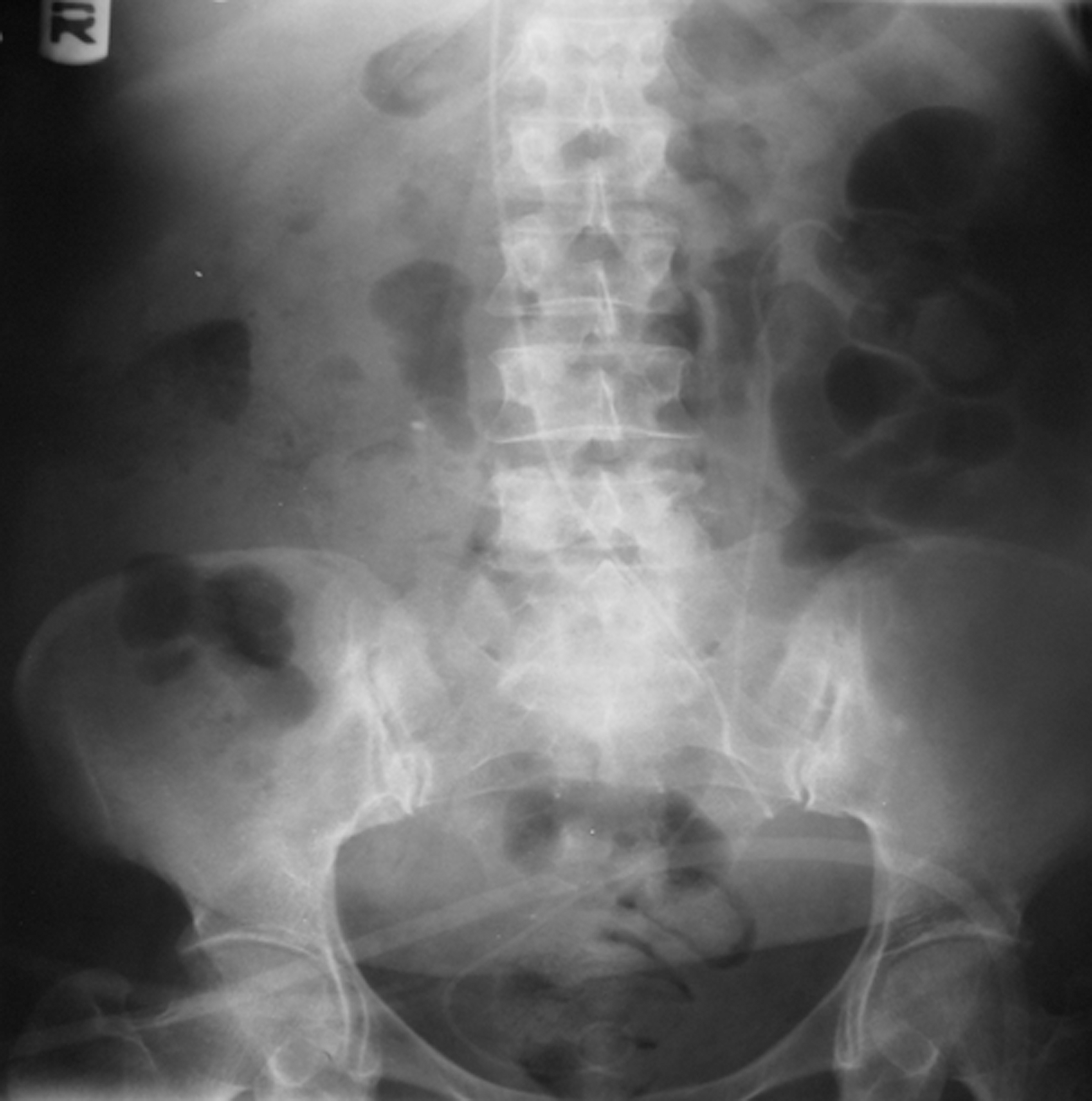
Radiograph of the kidneys, ureters, and bladder showing right-side deviation of the migrated Double-J stent.

Noncontrast computed tomography reveals two Double-J stents.

Computed tomography shows intravenous (intracaval) position of the migrated Double-J stent.

Percutaneous removal of migrated Double-J stent through the left femoral vein.
The patient was discharged in a well condition with mild anemia 2 days after removal of the stent. Although she had deep vein thrombosis 7 days after discharge because of the prolonged intravascular foreign body and underwent specific therapy, she had no urologic problem and other complication. The inserted ureteral stent was removed on postoperative week 4 and retrieval of the urinary system was successfully achieved.
Discussion
Iatrogenic ureteral injuries happen mostly in the lower third of the ureter and are mainly from urologic and gynecologic procedures. 1 The ureter may be injured during abdominal hysterectomy because of nearness to the cervix. Several surgical techniques are performed for repair of the injured ureter. Endoscopic placement of a Double-J stent can be considered as an initial endourologic therapeutic intervention, especially in incomplete ureteral injury. 1 In addition, the ureteral stent is used for continuation of urinary flow and prevention or removal of obstruction and injury before or after ureteral surgery.
Today, urologists easily perform endoscopic retrograde positioning of a ureteral Double-J stent. Use of a ureteral stent, however, may be accompanied by complications, such as lower urinary tract symptoms, loin pain, hematuria, urinary tract infection, vesicoureteral reflux, malposition, migration, luminal obstruction, encrustation, ureteral erosion or necrosis and fistulization, and fractured or forgotten stent. 2
Michalopoulos and associates 3 reported pulmonary thromboembolism from migration of a stent into the heart and left pulmonary arterial system after pyelolithotomy and antegrade insertion of a pigtail ureteral stent. 3 We report malposition and intravascular migration of a Double-J stent into the IVC as a rare complication of endoscopic retrograde ureteral stent placement.
With prevalent use of a ureteral stent in several urologic problems and interventions, attention to safe and correct insertion of the stent is necessary. Although insertion of a ureteral stent is simply performed, serious complications may occur during and after this procedure. Radiologic imaging is a proper monitoring method for early detection and immediate retrieval of position and probably complication of the stent. It is better to achieve ureteral stent placement under fluoroscopic guidance. In the absence of fluoroscopy, intraoperative and postoperative KUB radiography is beneficial for confirmation of the suitable placement of the ureteral stent. Also, use of a guidwire can be considered for better insertion and safer passing of a ureteral stent. Attention to quality, integrity, and proper size of the stent before placement and abnormal or uncommon patient signs and symptoms are useful for prevention, early diagnosis, and management of ureteral stent complications.
Footnotes
Disclosure Statement
No competing financial interests exist.