
Abstract
Background and Purpose:
The optimal management of renal and ureteral calculi in transplanted kidneys is not well defined. Although larger (>1.5 cm) stone burdens are generally treated with percutaneous nephrolithotomy (PCNL), smaller stones may be reasonably approached with retrograde or antegrade ureteroscopy (URS). We report our multicenter experience with URS for transplant lithiasis.
Patients and Methods:
URS performed for stone disease within a transplanted kidney were retrospectively identified at three stone-referral centers between 2006 and 2011. Demographic and disease parameters were recorded, as were perioperative and postoperative details.
Results:
Twelve patients underwent URS for a calculus in a transplant renal unit and/or ureter. For retrograde procedures (7), access to the ureteral orifice was facilitated by the use of a Kumpe catheter; a two-wire (safety and working guidewire) technique was used. For antegrade procedures (5), the ureteroscope was passed into the kidney using a two-wire technique without tract dilation. All stones but one necessitated holmium:yttrium-aluminum-garnet laser lithotripsy with extraction of stone fragments. All patients were stone free on postoperative imaging except for one patient with a 2-mm fragment that was observed. Stone analysis included calcium oxalate (6), calcium phosphate (4), and struvite (1).
Conclusion:
Antegrade and retrograde URS are safe and effective treatments for patients with simple stone burdens in a transplanted kidney. Although retrograde access to the ureter can be challenging, specialized techniques and modern endoscope technology facilitate this process. Antegrade URS for small stone burdens can be performed safely and effectively without tract dilation.
Introduction
To better define the feasibility and effectiveness of URS management of transplant stones, we performed a multi-institutional study of patients who were undergoing antegrade or retrograde URS management of this condition.
Patients and Methods
All patients with a history of renal transplant and nephrolithiasis or ureterolithiasis undergoing URS treatment between the years 2006 and 2011 were eligible for inclusion. URS procedures were defined as nondilated antegrade approaches or transurethral retrograde approaches. Preoperative, intraoperative, and postoperative parameters were recorded via a standardized methodology.
Technique for nondilated antegrade URS
In all cases, percutaneous access to the transplant collecting system was obtained in advance of the URS procedure. In the operating room, the patient was placed in the supine position. Nephrostography was performed through the existing nephrostomy drain, and then a flexible tip hydrophilic guidewire was advanced into the collecting system via the nephrostomy. This wire was directed down the ureter into the bladder with the assistance of an angiographic catheter, and the hydrophilic guidewire was exchanged for a nitinol or Amplatz superstiff guidewire (Fig. 1). A second nitinol guidewire was then placed as a “safety wire” with the use of a coaxial catheter. No formal balloon dilation of the nephrostomy tract was performed.
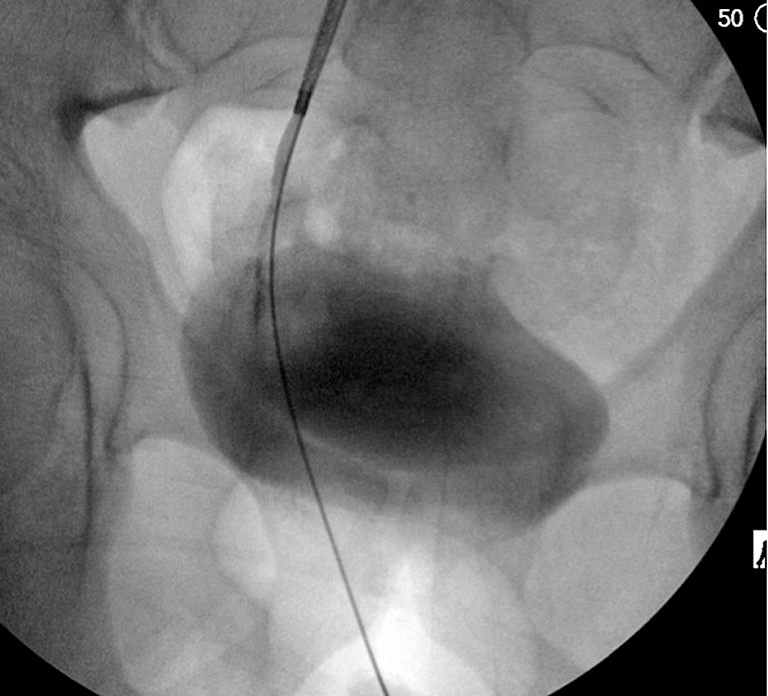
Fluoroscopic image of antegrade guidewire access through the collecting system into the bladder.
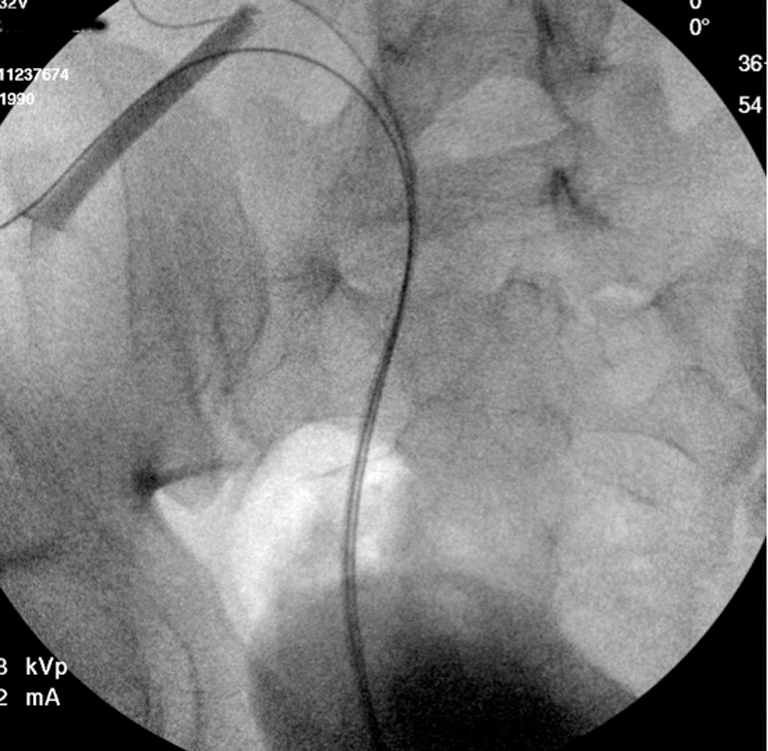
The flexible ureteroscope was advanced over the working wire into the transplant collecting system with fluoroscopic guidance (Fig. 2). Once stone material was identified, it was extracted intact or fragmented with holmium:yttrium-aluminum-garnet (Ho:YAG) laser lithotripsy. Active extraction was used to remove all fragments or fragments were guided and/or irrigated into the bladder. In cases of multiple fragments, a ureteral access sheath was used at the discretion of the treating surgeon; it was placed over the working wire, and fragments were extracted through the sheath (Fig. 3). Nephrostography was performed to confirm stone clearance as well as the absence of extravasation and distal ureteral obstruction. The nephrostomy drain was then removed.

Fluoroscopic image of antegrade flexible ureteroscopy into the collecting system.
Fluoroscopic image of ureteral access sheath placement into the collecting system for stone extraction.
Technique for retrograde access
The patient was placed in a dorsal lithotomy position, rigid cystoscopy was performed, and the heterotopic ureteral orifice visualized. An angle-tipped angiographic catheter—eg. a Kumpe or Berenstein catheter—was used as needed to advance a flexible tipped guidewire retrograde into the renal collecting system under fluoroscopic guidance. A safety wire was then positioned with either a dual-lumen or coaxial catheter, and the flexible ureteroscope was advanced over the working guidewire to the location of the stone. Balloon dilation of the ureteral orifice was not used. Stone fragmentation and removal were performed with standard ureteroscopic techniques, and lithotripsy was performed with the Ho:YAG laser in all cases. Ureteral access sheaths were used at the discretion of the treating surgeon. In all cases, ureteral stents were placed at the conclusion of the procedure.
Results
Twelve patients were identified for inclusion in the study; all patients harbored single or multiple calculi within the transplanted renal unit or transplanted ureter. Table 1 details demographic and stone-specific data. The majority of patients had a diagnosis of stone-related obstructive uropathy (Table 2).
Two patients had both ureteral and intrarenal stones.
URS procedures performed included seven retrograde procedures and five antegrade procedures. All but one procedure necessitated Ho:YAG laser lithotripsy with extraction of stone fragments. For all of the antegrade procedures, nephrostomy drains were replaced at the conclusion (8F pigtail tubes), and for all retrograde procedures, 6F ureteral Double-J stents were placed. Ureteral stents were removed 1 week postoperatively via outpatient cystoscopy, as were nephrostomy drains after confirmatory nephrostography. Postoperative complications developed in two patients who underwent an antegrade approach; in the first, a nephrocutaneous fistula developed hat closed spontaneously with conservative management and in the second, ureteral stent encrustation necessitated percutaneous extraction.
Follow-up data were available in 11 of 12 patients. All patients but one were stone free on postoperative imaging including eight by renal ultrasonography, two by CT, and one by nephrostography. One patient had a 2-mm lower-pole fragment on CT scan that was observed based on a discussion of risks and benefits of observation vs treatment. Follow-up transplant renal ultrasonography at 18 months postoperatively did not detect any stones or hydronephrosis in this patient. Evidence of ureteral stricture, hydronephrosis, impaired renal function, or stone recurrence at a mean follow-up of 14 months (range 3–46) was not seen in any patient. Stone analysis included calcium oxalate (6), calcium phosphate (4), and struvite (1); analysis was not available in one patient.
Discussion
Our present study demonstrates the safety and efficacy of URS for treatment of patients with small renal and ureteral stone burdens within transplanted kidneys. Using both retrograde and antegrade approaches, we were able to successfully clear stone burden from transplanted kidneys without major complications. The antegrade approach was used when a nephrostomy tube had been previously placed for temporization of infection or renal dysfunction, because this provided a straightforward route to the kidney and ureter, and retrograde approaches were used in the other cases. Although PCNL remains the preferred treatment for larger stones, URS is emerging as a preferred approach for smaller stone burdens in these patients.
URS for transplant lithiasis has clearly benefited from advances in both surgical technology and surgical technique. Until recently, reports on the URS approach to transplant stones have been scarce; the most commonly reported approaches to such stones have been either SWL or PCNL. As endoscopes have become increasingly miniaturized and deflectable, however, ureteral dilation has become unnecessary, and all portions of the intrarenal collecting system can be accessed in a straightforward manner.
We left nephrostomy tubes in place at the conclusion of our antegrade procedures with nephrostography at 1 week postoperatively to confirm drainage and absence of extravasation. While this step might be omitted with a “tubeless” approach, including placement of a ureteral stent at the end of the case, we preferred the additional assurance of nephrostomy drainage and confirmation of drainage in these patients with a solitary renal moiety.
There have been few reported experiences with URS for the treatment of stones in transplanted kidneys. Del Pizzo and associates 11 reported on four patients undergoing semirigid retrograde URS for treatment of transplant stones. Three patients had 3 to 4 mm stones that were impacted in the distal ureter, and one patient had a 3-mm calculus on exposed nonabsorbable suture at the ureteral orifice. As with our experience, access to the ureter was facilitated with angled catheters and hydrophilic wires. Unlike in our series, though, the transplant ureteral orifice was balloon dilated to 10 mm with a high-pressure balloon dilator. Likely this important difference is a consequence of the more miniaturized and flexible endoscopes that are presently available, but were not available over a decade ago when this article was published.
SWL has also been used for treatment of smaller stone burdens in transplanted kidneys and has been reported to be safe and effective. 7 –9 One important disadvantage of SWL of transplant kidneys is the position of the kidney within the bony pelvis, which may limit visualization of stones on fluoroscopy as well as mitigate the propagation of shockwave energy. Prone positioning may counter these disadvantages. An additional disadvantage of SWL is the need for multiple treatment sessions: While Challacombe and colleagues 7 reported successful treatment in allograft stones with a mean size of 8.1 mm, 8 of 13 patients needed multiple SWL procedures. 7 Although some authors advocate for SWL for 5 to 15 mm transplant renal stones, 10 our experience with URS suggests that this endoscopic approach is a viable treatment modality as well.
Larger stone burdens within transplanted kidneys have been successfully treated with PCNL, for which greater invasiveness is thought to be justified by maximal stone clearance. 5,6 The superficial position of the kidney generally enables straightforward percutaneous access using ultrasonographic or CT guidance; however, there have been reports of bowel injury, allograft renal artery, and arteriovenous fistulae after transabdominal access. 5,11 Other reported concerns with PCNL in a transplanted kidney have included perirenal fibrosis impeding tract dilation and limited mobility of the kidney during rigid nephroscopy, 3 although other series have not reported difficulty with these aspects. 5,12 Dilation has been performed with Amplatz dilators up to 28F and with balloon catheters up to 30F without reported sequelae. Taking this evidence into account, PCNL is likely the most appropriate intervention for large volume or complex calculi, but may be excessively morbid for smaller volume stones.
Previous reports have suggested that stones occurring in transplanted kidneys are composed predominantly of calcium oxalate, which is consistent with our experience. 10,13 Patients who have undergone renal transplantation are at risk for development of a number of lithogenic conditions, including tertiary hyperparathyroidism, hypercalciuria, hypocitraturia, hyperuricosuria, chronic urinary tract infection, urinary stasis, and nidus such as nonabsorbable suture. 13 Medications including steroids (hyperuricemia, hypercalciuria) and cyclosporine (hyperuricosuria) may increase risk of stone formation as well. Identifying causal factors may help to decrease risk of stone recurrence; thus, metabolic evaluations should be considered in these patients.
As was our experience, others have also reported excellent functional outcomes after treatment of transplant lithiasis. 7,14 Although limitations of these studies prohibit definitive conclusions about treatment safety and long-term effects, no graft failure attributable to surgery has been reported. It may be that techniques with which a practitioner has greatest familiarity are advised.
Limitations of our study include retrospective design and a small number of patients, which reflect the low prevalence of transplant stone disease. This number was the result of pooled data from three high-volume stone disease centers. In addition, the procedures were performed by experienced endourologists, and the technical challenges of URS within the altered anatomy of a transplanted kidney may be prohibitive for less experienced surgeons.
Conclusion
Kidney stones occurring in transplanted renal units are an uncommon but serious and potentially morbid medical condition. In our study, which is the largest experience with URS for transplant lithiasis, we found that this approach is both safe and efficacious. There is little controversy that PCNL is the most appropriate treatment for patients with large or complex stone burdens in transplanted kidneys. In our experience, however, URS is a competitive technology to SWL for smaller stone burdens: We experienced no major complications, and all patients were cleared of their symptomatic stones.
Footnotes
Disclosure Statement
No competing financial interests exist.