
Abstract
Background and Purpose:
Despite clear trends toward minimally invasive surgery, information about laparoscopic partial nephrectomy (LPN) in Japan is sparse. We conducted a retrospective survey to clarify time trends for LPN and analyze surgical and oncologic outcomes.
Patients and Methods:
A nationwide survey was performed. Between 1998 and 2008, 1375 patients underwent LPN at 54 institutions. Complications, patterns of tumor recurrence, and recurrence-free survival were analyzed.
Results:
Renal pedicle clamping was used in 1031 (75%) cases, and renal cooling was performed in 64%. Median warm/cold ischemic time was 37/53 minutes. Median tumor size was 2.26 cm (interquartile range 1.6 to 2.7). Multivariate analysis identified total operative time, operative blood loss, and surgical margin status as independently associated with high grade (grade 3–5) urologic and nonurologic complications. Despite increases in central tumor, a trend was seen toward shorter warm/cold ischemic time in recent cases, and the overall complication rate did not change throughout the study period. With a median follow-up of 26 months for 1193 malignancies, recurrence occurred in 22 (1.7%) patients, including local recurrence in 7 (0.5%), lung in 8 (0.7%), lymph nodes in 2 (0.1%), and bone in 4 (0.3%). Of the 26 cases with positive surgical margins, local tumor recurrence occurred in only one.
Conclusions:
This is the first nationwide survey of LPN in Japan to be reported. LPN could be performed with acceptable positive margins and complication rates. Most tumor recurrences occur as metastases, and surgical margin status appears to have little impact on oncologic outcomes.
Introduction
In an effort to reduce patient morbidity, urologic surgeons have adapted the minimally invasive technique of laparoscopy to kidney removal. Laparoscopic partial nephrectomy (LPN) is associated with somewhat greater ischemia time and postoperative complications compared with OPN. 7 Several technical modifications for LPN have recently been introduced, resulting in improved outcomes and wider adoption. 8,9 Few reports, however, have examined long-term oncologic outcomes for LPN. 10
Despite a drastic trend toward minimally invasive surgery, data on the prevalence of LPN in Japan and surgical outcomes are sparse. To obtain such information, we conducted a nationwide survey.
Patients and Methods
The Institutional Review Board approved retrospective data collection and reporting of the results for this study. A nationwide survey was performed by the Japanese Society of Endourology LPN study group. A survey was sent to all 473 urologists (228 institutes) certified by the Endoscopic Surgical Skill Qualification System in Urological Laparoscopy. 11 The system was established in 2003 and was designed to certify urologists who have the capability to complete laparoscopic nephrectomy or adrenalectomy safely and appropriately by their own efforts. 11 Institutes in which more than 10 cases of LPN had been performed at the time of survey were eligible for the study. We retrospectively reviewed 1375 patients who underwent LPN between December 1998 and December 2008.
Baseline renal function was evaluated by serum creatinine measurements and calculation of estimated glomerular filtration rate (eGFR), the latter based on the Japanese Society of Nephrology Chronic Kidney Disease Initiative equation: GFR (mL/min/1.73 m2)=194×serum creatinine−1.094×age−0.287×0.739 (if female). 12 Because LPN with pedicle clamping was introduced in Japan around 2002 and the number of LPNs markedly increased from 2007, we divided the 1375 patients into three chronological eras: Era 1, 147 cases from December 1998 to December 2002; era 2, 624 cases from January 2003 to December 2006; and era 3, 604 cases from January 2007 to December 2008.
All complication events occurring within 30 days after surgery were included in the study. A five-tiered classification scheme based on the National Cancer Institute Common Toxicity Criteria (NCI-CTC), version 2.0, was used to grade the intensity of therapy needed for each complication, including: Grade 1, mild adverse event; grade 2, moderate adverse event; grade 3, severe and undesirable adverse event; grade 4, life-threatening or disabling adverse event; and grade 5, death related to adverse event. 13
Uni- and multivariate logistic regression analyses were used to evaluate variables associated with experiencing a complication, with separate analyses conducted for the outcome of high-grade (grade 3–5) complications. Continuous variables were reported as mean (standard deviation) and range or as median and interquartile range, as appropriate. The Student t test and the Wilcoxon rank sum test were used to compare continuous variables, as appropriate. The Pearson chi-square test was used to compare categoric variables. The Kaplan-Meier method was used to calculate survival functions, and differences were assessed with the log rank statistic. Univariable and multivariable logistic regression models addressed time after surgery. Statistical significance in this study was set as P=0.05. All reported P values were two-sided, and analyses were performed using JMP9® software (SAS Institute, Cary, NC).
Results
Patient demographics
Of the 228 institutes to which surveys were sent, 54 (23.7%) participated in the study, and a total of 1375 patients were enrolled. All of the hospitals that participated were teaching centers certified by the Japanese Urological Association. The median number of cases reported by center was 27 (range 10–102). The median age at the time of LPN was 60 years (range 16–88 y). Distributions of baseline characteristics are summarized in Table 1. Basic characteristics were similar between the three eras with the exception of the American Society of Anesthesiologists score and frequency of diabetes mellitus. Cold ischemic partial nephrectomy (PN) was performed for 657 (48%) cases; 59% of kidneys were cooled with ice-cold saline using an irrigation device, and 41% of kidneys were cooled with ice introduced via a laparoscopic port. A total of 275 (21%) patients had eGFR <60 mL/min/1.73 m2. Patients in the most recent era showed a higher frequency of comorbidity. The number of patients undergoing LPN each year increased with each successive era (Fig. 1).
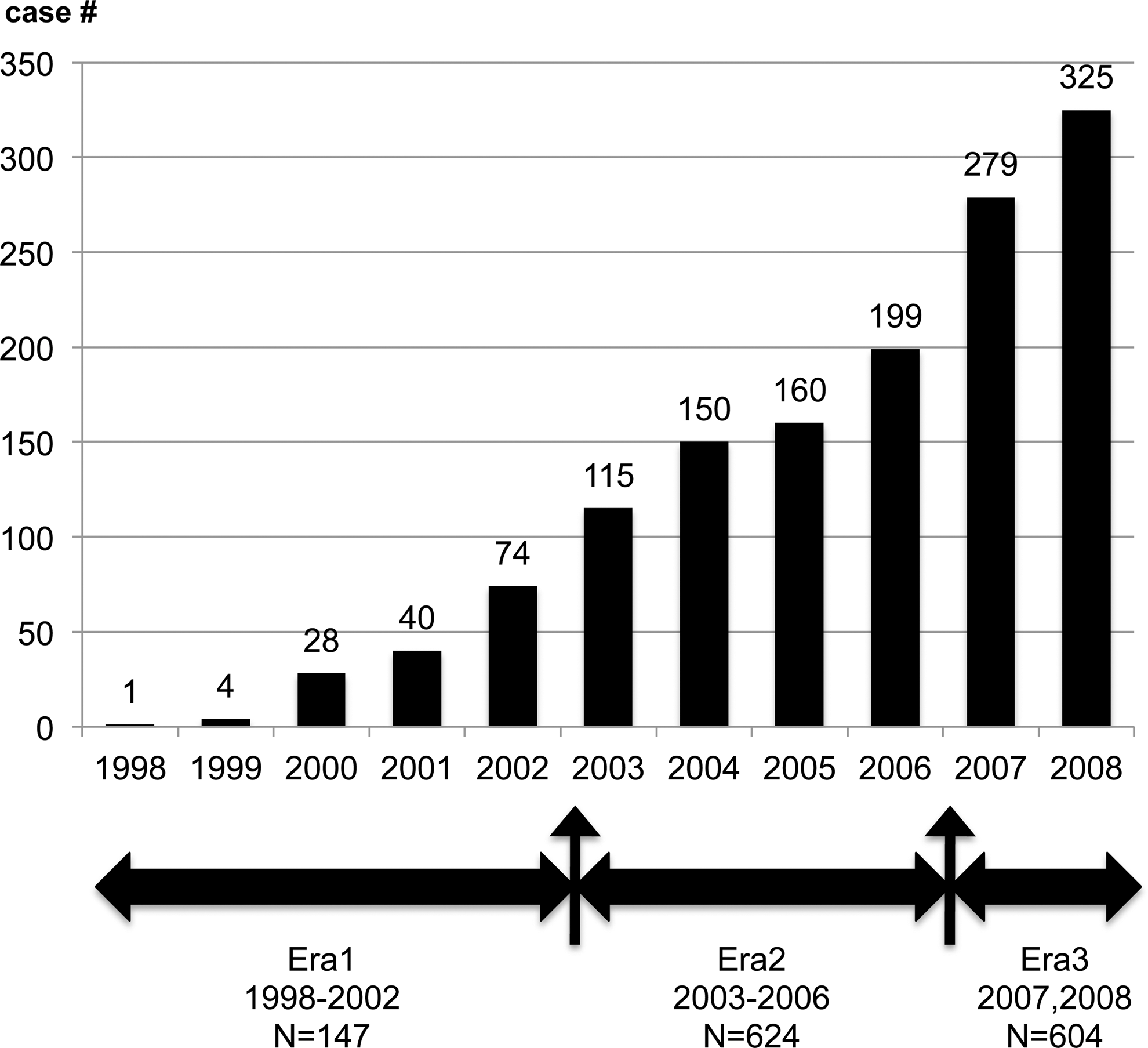
Patients undergoing laparoscopic partial nephrectomy per era.
body mass index=mass (kg) / (height(m))2.
eGFR (mL/min/1.73m2)=194×Serum creatinine−1.094×Age−0.287×0.739 (if female).
eGFR less than 60 ml/min/1.73m2.
SD=standard deviation; IQR=interquartile range; BMI=body mass index; ASA=American Society of Anesthesiologists; eGFR=estimated glomerular filtration rate; CKD=chronic kidney disease.
Perioperative outcomes
The retroperitoneal approach was used in 893 (65%) cases. Pedicle clamping was used in 1031 (75%) cases, and renal cooling was performed in 64% of cases. Median operative time was 245 minutes (Table 2). In era 1, 83% of LPNs were performed without clamping, with three-quarters performed using microwave coagulation 14,15 and the others performed using methods such as bipolar electrocoagulation and ultrasonic scalpels.
Hand-assisted Laparoscopic Surgery (transperitoneal approach).
tumor in middle-third of kidney.
LPN=laparoscopic partial nephrectomy; SD=standard deviation; IQR=interquartile range.
To ensure pelvicaliceal repair, a ureteral catheter was inserted cystoscopically into the affected renal pelvis in 910 (66%) patients, and the total operative time included time for catheter insertion. Median warm ischemia time progressively shortened, at 50 minutes, 38 minutes, and 35 minutes in eras 1, 2, and 3, respectively. Median cold ischemic time, including an initial cooling time of about 10 minutes, was 58 minutes, 55 minites. and 50 minutes, respectively. Mean eGFR at baseline and 12 months after LPN were 74.1 and 65.8 mL/min/1.73 m2, respectively, and the difference was significant (P<0.0001). LPN was successfully completed as planned in 1271 (92.6%) patients. Conversion to OPN, open nephrectomy, and laparoscopic nephrectomy occurred in 69 (5.0%), six (0.4%), and 27 (2.0%) cases, respectively.
Early complications
Table 3 lists urologic complications. Grade 3/4 urologic complications comprised renal insufficiency in four (0.3%)/2 (0.2%), urine leakage in 34 (2.5%)/24 (1.7%), hematuria in 182 (13.8%)/17 (1.3%), and hemorrhage in 115 (8.7%)/31 (2.3%) cases. Postoperative hemorrhage was seen in 40 (2.9%) cases, 14 (1.0%) of which necessitated transcatheter arterial embolization. Blood transfusion was needed in 21 (1.5%) patients. With regard to nonurologic complications, grade 3–5 complications arose in four patients, comprising one pulmonary embolism, one ascending colon injury on insertion of the port, one cerebral infarction, and one air embolism that occurred during the use of fibrin glue (Bolheal,® The Chemo-Sero-Therapeutic Research Institute, Kumamoto, Japan) and resulted in death (grade 5) on postoperative day 7.
All complications were classified based on the NCI-CTC version 2.0.
On univariate analysis, body mass index, hypertension, tumor diameter (cm), total operative time (min), operative blood loss (mL), caliceal suturing, and surgical margin status were significantly associated with high-grade (grades 3–5) complications (Table 4). Factors that lacked significance were age, sex, hyperlipidemia, preoperative renal function (creatinine, eGFR), indication of LPN, solitary kidney, renal cooling, pedicle clamping.
BMI=body mass index; CKD=chronic kidney disease.
On multivariate analysis, total operative time (min), operative blood loss (mL), and surgical margin status were independently associated with grade 3 to 5 complications.
Pathologic findings and oncologic outcomes
Of the 1375 LPN in our dataset, 182 (13.2%) were associated with benign lesions, including angiomyolipoma in 109 (7.9%), oncocytoma in 30 (2.2%) and others in 43 (3.1%). Malignant histology was found in 1193 (86.8%) cases, including clear cell carcinoma in 1049 (76.3%), papillary carcinoma in 95 (6.9%), chromophobe carcinoma in 36 (2.6%), and others in 13 (0.9%).
With a median follow-up of 26 months for 1193 patients with malignant histology, recurrence occurred in 23 (1.7%) patients (Fig. 2), including local recurrence in seven (0.5%), lung in eight (0.7%), lymph nodes in two (0.1%), and bone in four (0.3%). Tumor recurrence rate according to tumor size was 0.0% for 0 to 1.0 cm tumors (n=14), 0.3% for 1.1 to 2.0 cm (n=382), 0.8% for 2.1 to 3.0 cm (n=524), and 0.8% for tumors >3 cm (n=247). On univariate analysis, tumor size was not significantly associated with recurrence rate (P=0.145). Positive surgical margins were observed in 26 cases, in which 22 (85%) involved malignancy; eight were converted to laparoscopic RN, and recurrence occurred in only one case.
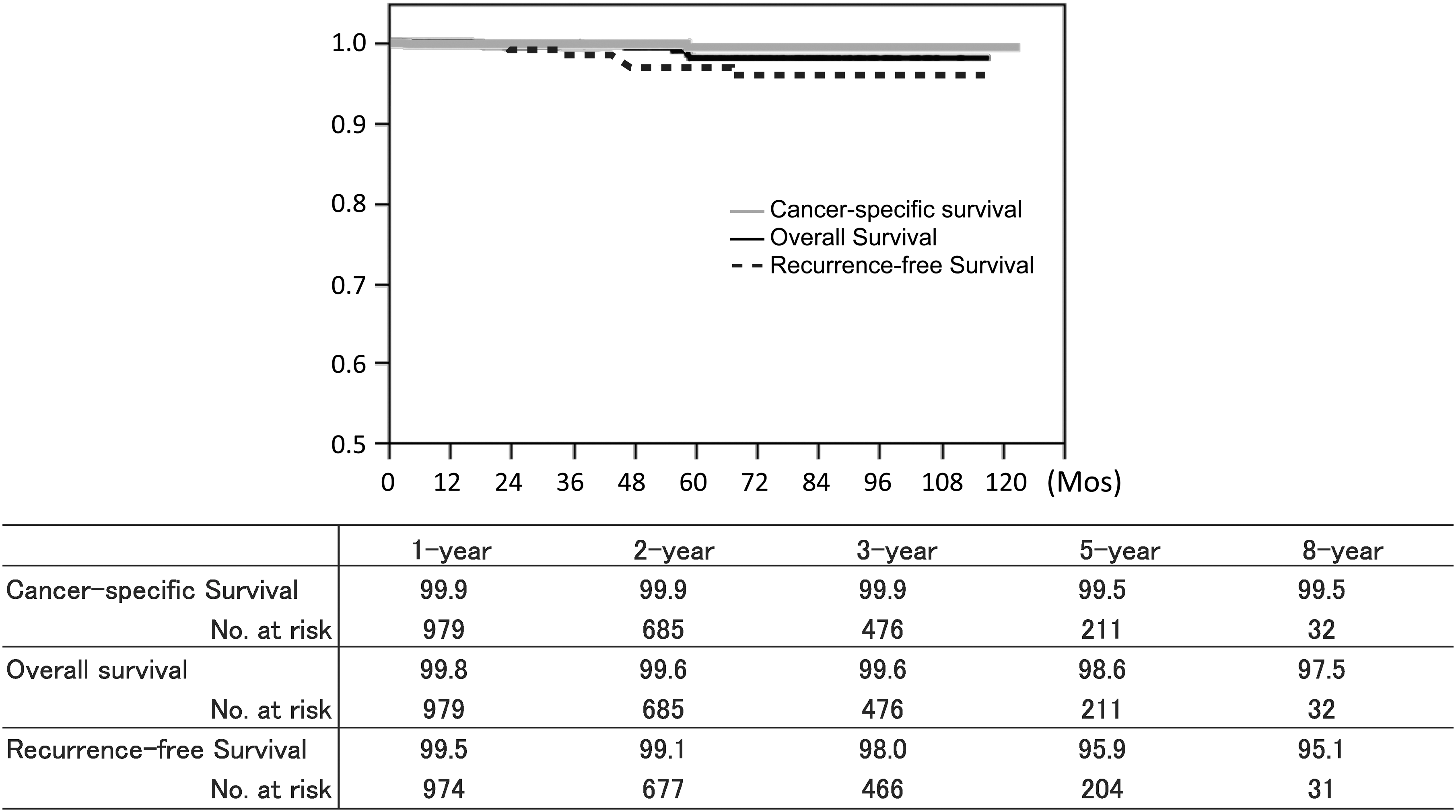
Survival in 1193 patients with malignant history.
Nine patients died during the study period. After excluding the patient who died 7 days postoperatively because of pulmonary embolism, the remaining eight cases were analyzed. Mean time to death after LPN was 39 months. Two patients died from kidney cancer; one in whom lung metastases had been identified preoperatively died 59 months after LPN, and one died 4 months after surgery because of intraperitoneal recurrence. Four patients died from other malignancies (Fig. 2).
Discussion
PN was initially reserved for absolute indications such as patients with a solitary kidney, renal insufficiency that would likely result in the need for dialysis, or inheritable forms of renal cancer. PN, however, is now considered the treatment of choice for most clinical T1 renal masses, even in patients with a normal contralateral kidney. With advances in laparoscopic instrumentation and greater dissemination of expertise, LPN is now often performed using the same surgical techniques as its open counterpart, such as vascular control, 9 renal hypothermia, 8 watertight closure of the collecting system and capsule, and use of surgical bolsters. With these advances, LPN has gained popularity as a less-invasive procedure for small renal tumors. In particular, patients with small peripheral lesions who meet the criteria for OPN should be considered for LPN.
To facilitate standardized comparisons among cohorts, we classified complications based on NCI-CTC, version 2.0. This allowed systematic and comprehensive reporting of surgical complications by standardizing definitions of complication events and enabling clear comparison of the frequency and severity of events among various series. 16 We compared our LPN data with reported series that had used the same standardized NCI-CTC reporting method. 17 All-grade complication rates were 8% to 18% and 27% for urologic complications, and 11% to 15% and 2% for nonurologic complications in previous reports and the present study, respectively.
The present study appeared to have higher rates of low-grade hematuria and intraoperative hemorrhage, but this cohort included many institutes, and some events might have been overclassified in the retrospective chart review, especially for hematuria and intraoperative hemorrhage. Regarding high-grade events, the present data were comparable to other reports. Postoperative hemorrhage is arguably the most important urologic complication after OPN or LPN. The incidence of hemorrhage is 1.4% to 7.9% after OPN 5 and 2.1% to 6% after LPN. 16,18 Our retrospective cohort contained our initial experience, but the postoperative hemorrhage rate was 2.9% and the urine leakage rate was 2.5%, both of which were comparable to that of previous studies.
On multivariate analysis, only total operative time (min), operative blood loss (mL), and surgical margin status were independently associated with all types of complications. These results were expected, because intraoperative bleeding makes the procedure difficult to perform.
With regard to conversion rate, LPN showed the highest rate (3.9%) among the various procedures, but this rate was still comparable to those for cryoablation (3.5%) and laparoscopic RN (3.0%). 19 In addition, Breda and associates 20 reported the results of 855 LPNs from 17 centers and identified a 2.4% positive margin rate. Our conversion rate was slightly higher (7.4%), but the positive margin rate was only 2%, a figure comparable to previous studies.
As for oncologic outcomes, previous reports have suggested that the presence of a positive surgical margin has no impact on overall or cancer-specific survival for patients treated using PN. 21,22 Reported positive surgical margin rates have varied from 2% to 6% in contemporary OPN and LPN series, while recurrence rates range between 0% and 6%. 23,24 Several reasons might explain such low rates of local recurrence. First, false-positive margins can occur during tissue processing, and even legitimate microfoci of residual cancer cells may never result in clinical recurrence if adequately treated by intraoperative fulguration or application of an argon beam to the tumor base. Second, because the average annual growth rate of radiographically visible but small renal masses is 0.28 to 0.42 cm, 25,26 residual cancer cells may need many years to become clinically apparent. Third, among the cases with tumor recurrence, local recurrence alone developed in only five (23%), and metastasis with or without local recurrence developed in others, indicating that the majority of cases in which recurrence developed already had micrometastases present by the time of surgery. These results should encourage urologists to perform PN, even if the anticipated resection margin is close and the tumor abuts the collecting system or renal hilum.
In this survey, no recurrence was observed for tumors ≤1 cm in diameter. Although no significant difference was seen, tumors >2 cm in diameter had a tendency to recur more frequently than those ≤2 cm in diameter.
The limitations of our study include the retrospective nature of the data analysis. Each institute has different indications for LPN, so some selection bias likely contributed to the observed differences in rates of complications among institutes. Because the data were based on findings from only 54 institutes, however, some bias might be associated with the results. Because our survey was sent to only urologists certified by the Endoscopic Surgical Skill Qualification System in Urological Laparoscopy, the results are considered to represent the contemporary status of LPN in Japan. Although we should report surgical complications using the Clavien system, 27 we planned this study on 2008, and at that time NCI-CTC, version 2.0, was used as a recommended PN reporting criteria. 17 For the same reason, we could not report anatomic tumor characteristics according to the R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score 28 or PADUA (preoperative aspects and dimensions used for an anatomical) score. 29 A prospective study needs to use the scoring system that is an important predictor of perioperative complications and oncologic outcomes.
The present study is unique in that renal cooling was used in about half of the cases. Renal cooling, either by ice or ice-cold saline, has been widely used for LPN in Japan. The limitation, however, is the lack of detailed data on the methods of renal cooling and on split renal function, and of a group receiving OPN. We were thus unable to fully elucidate the impact of LPN alone or LPN with renal cooling on renal function in comparison with open surgery. Becker and colleagues 30 suggested that renal scintigraphy with 99mTc-mercaptotriglycylglycine is currently the best method for exact determination of renal function loss after tissue resection and ischemic injury. A prospective multi-institutional study comparing the impact of LPN or OPN on split renal function is ongoing and will provide an accurate reflection of the functional status of the operated kidney.
Conclusions
LPN is a challenging surgery necessitating advanced laparoscopic techniques. Using a large cohort and standardized NCI-CTC reporting system, we demonstrated that LPN could be performed with positive margins and complication rates comparable to those of previous studies. Standardization of data reporting will allow for more objective assessment of changes in technique as well as improved comparison of alternative treatment strategies. Most of the tumor recurrences occurred as metastases with or without local recurrence, and surgical margin status appears to have little impact on oncologic outcome.
Footnotes
Acknowledgment
Funding from the Japanese Society of Endourology. The following list represents contributors and institutions involved in this study: Dr. Watanabe S. of Saiseikai Kumamoto Hospital, Dr. Sazawa A. and Dr. Nonomura K. of Hokkaido University, Dr. Matsuura S. of Sendai Shakai Hoken Hospital, Dr. Kondo T. of Tokyo Women's Medical University, Dr. Kawauchi A. of Kyoto Prefectural University, Dr. Nomoto T. of Tokai University, Dr. Hattori R. of Nagoya University, Dr. Hamasaki T. and Dr. Kondo Y. of Nippon Medical School Hospital, Dr. Tanaka K. of Kobe University, Dr. Kobayashi K. and Dr. Mita K. of Hiroshima University, Dr. Nakagawa K. of Keio University, Dr. Yoshimura K. of Kyoto University, Dr. Sasamoto H. of Kitasato University, Dr. Kato T. and Dr. Tomita Y. of Yamagata University, Dr. Kouda S. of Kure Medical Center and Chugoku Cancer Center, Dr. Makiyama K. of Yokohama City University, Dr. Okegawa T. of Kyorin University, Dr. Terai A. of Kurashiki Central Hospital, Dr. Naya Y. of Chiba University, Dr. Ujiie T. and Dr. Nishimura K. of Osaka Rosai Hospital, Dr. Sakamoto W. of Osaka City General Hospital, Dr. Tsujihata M. of Osaka University, Dr. Okasyo K. and Dr. Okumura K. of Tenri Hospital, Dr. Zakoji H. of Yamanashi University, Dr. Obara T. and Dr. Habuchi T. of Akita University, Dr. Kan M. and Dr. Tanimoto S. of Ehime Prefectural Central Hospital, Dr. Inokuchi J. and Dr. Seiji N. of Kyushu University, Dr. Takei F. and Masumori N. of Sapporo Medical University, Dr. Ito K. and Asano T. of National Defense Medical College Hospital, Dr. Kameoka H. of Hoshi General Hospital, Dr. Narita M. of Shiga University, Dr. Izaki H. and Dr. Kanayama H. of Tokushima University, Dr. Inagaki T. of Wakayama Medical University, Dr. Kobayashi M. of Isesaki Municipal Hospital, Dr. Hosomi M. of Osaka General Medical Center, Dr. Ishizuka O. of Shinshu University, Dr. Takagi H. and Dr. Yamamoto Y. of Kurashiki Medical Center, Dr. Taguchi I. and Dr. Kawabata G. of Kansai Rosai Hospital and Dr. Suenaga T. and Dr. Kakehi Y. of Kagawa University.
Disclosure Statement
No competing financial interests exist.