
Abstract
Background and Purpose:
One of the more challenging portions of robot-assisted radical prostatectomy (RARP) is the urethrovesical anastomosis. Because of this, a unidirectional absorbable barbed suture (V-Loc™) has been used to complete the anastomosis with better efficiency and less tension. The effect of robotic needle driver manipulation on barbed suture is unknown. Therefore, the aim of this study is to determine whether robotic manipulation decreases the tensile strength and peak sliding force of V-Loc barbed suture.
Materials and Methods:
Fifty-six V-Loc sutures were compared with 56 Maxon sutures. All sutures were 3-0 caliber. Half of the sutures in each group were manipulated with a da Vinci® robot large needle driver five times over a 5 cm length of suture. The other half was not manipulated. Breaking force was determined by placing sutures in a Bose ElectroForce load testing device. For sliding force testing, 28 V-Loc sutures were manipulated in the same fashion and compared with 28 nonmanipulated V-Loc sutures. Peak force needed to make the suture slip backward in porcine small intestine was determined to be the sliding force. Scanning electron microscopy of the barbs before and after robotic manipulation was also performed.
Results:
The mean difference in breaking forces for manipulated vs nonmanipulated Maxon sutures was 4.52 N (P=0.004). The mean difference in breaking forces for manipulated vs nonmanipulated V-Loc sutures was 1.30 N (P=0.046). The manipulated V-Loc group demonstrated a lower peak sliding force compared with the nonmanipulated group (0.76 vs 0.88 N, P=0.199). Electron microscopy revealed minor structural damage to the barbs and suture.
Conclusion:
Tensile strength and peak sliding force of V-Loc suture is decreased by robotic manipulation. This is likely because of structural damage to the suture and barbs. This structural damage, however, is likely not clinically significant.
Introduction
The V-Loc suture is a unidirectional barbed suture composed of polyglyconate, a copolymer of glycolic acid and trimethylene carbonate, and is absorbed within 180 days. This suture allows for knotless wound closure and improved suturing efficiency, especially with tissues under tension. It was originally developed for superficial wound closure, especially in the plastic and reconstructive surgery realm where tissue is often under some degree of tension.
A key difference between open and laparoscopic technique is the repeated grasping of the suture itself during laparoscopic suturing. Ricchiutti and associates 4 demonstrated that robotic needle driver manipulation leads to diminished tensile strength of both braided and monofilament suture. It was noted in this study that da Vinci® robot (Intuitive Surgical, Sunnyvale, CA) large needle drivers could impart a crushing force of up to 17 N.
The package insert for V-Loc 180 specifically states: “Avoid crushing or crimping damage due to application of surgical instruments such as forceps or needle drivers.” Despite this, V-Loc 180 barbed suture use has become more widespread during RARP where it is customary to repeatedly grasp the suture with needle drivers. The effect of robotic needle driver manipulation on V-Loc suture strength and barb integrity is unknown. Therefore, the aim of this study was to determine whether robotic manipulation decreases the tensile and barb holding strength of V-Loc unidirectional barbed suture.
Materials and Methods
Suture preparation and robotic manipulation
Two separate experiments were designed to evaluate the effect of robotic needle driver manipulation on V-Loc suture. For each experiment, one subset of suture was subjected to robotic manipulation and one group was not manipulated in any way (control group). A jig was created to hold each suture in place atraumatically. A 5-cm length in the center of each suture was marked with permanent ink and in this area the suture was manipulated with a da Vinci robot large needle driver commonly used during RARP. The jaws of the needle driver were closed with full force onto the suture five different times spaced 1-cm apart. The nonmanipulated (control) sutures were also placed into the same jig and a 5-cm area was marked, but the suture was not manipulated with the robotic instruments in any way.
Load testing equipment
All the tests were performed using a BOSE ElectroForce® load testing device. The load cell for measuring forces had a range of 225 N. The electromagnetic actuator of the device permitted an axial travel of 6 mm, so for breaking force tests, preloads were applied to remove slack from the suture and begin elongation.
Breaking force test
The first experiment evaluated breaking force (tensile strength). Both V-Loc 180 and Maxon™ were tested. All sutures were 3-0 in caliber. Maxon (Covidien, Mansfield, MA) suture is a nonbarbed monofilament suture that is also composed of polyglyconate and has similar biologic behavior to V-Loc. Maxon was used as a control to determine if the presence of barbs had any effect on tensile strength. Both the Maxon and V-Loc sutures were divided into two groups: Manipulated vs nonmanipulated (Fig. 1).
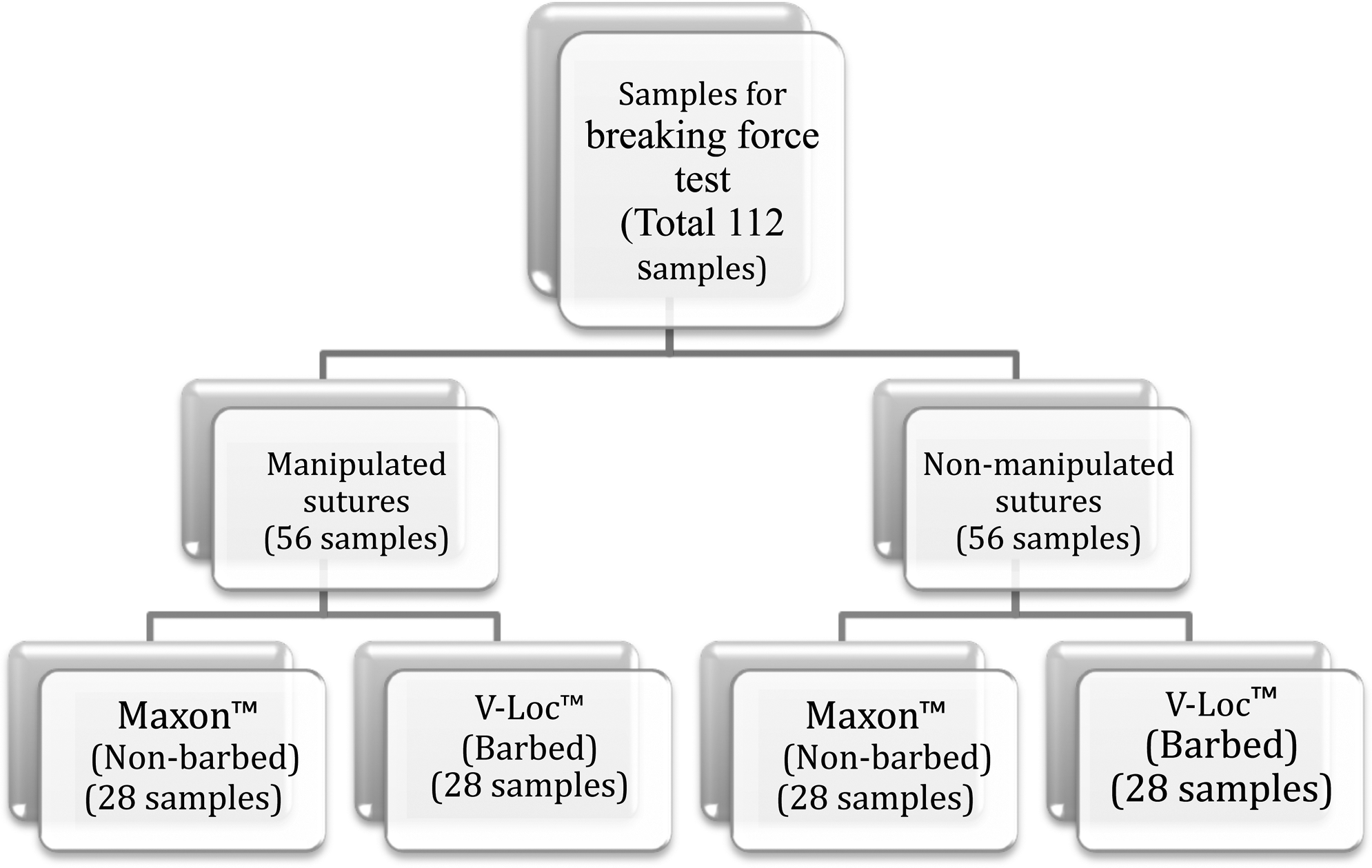
Distribution of samples for breaking force test of sutures.
Each suture sample was clamped and then a preload was applied (for Maxon samples, it was 35–40 N and for V-Loc samples, 25–30 N) followed by ramp loading. The difference in preload was based on preliminary testing that showed a difference in elasticity between the two sutures. This ramp was set to a value of 8 mm/s, and the suture samples were expected to rupture while this loading was being applied. The ramp force was then applied, and the greatest force achieved before suture breaking was electronically recorded for each suture. Figure 2 shows the sample held between the cylindrical custom-made fixtures. These fixtures were designed to ensure rupture only from tension—that is, without any stress concentration or trauma at the point of contact that might happen using conventional clamps.
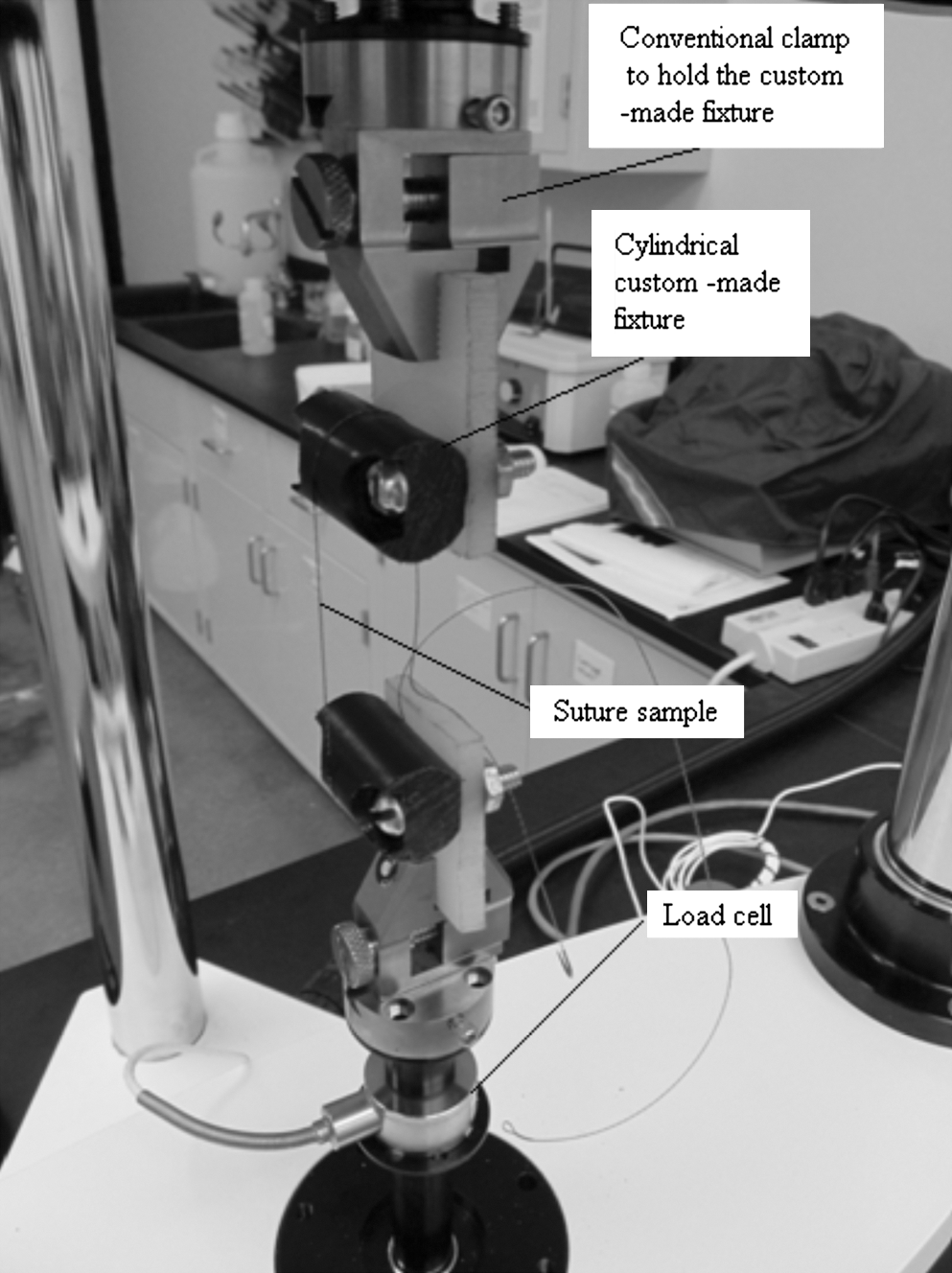
Suture sample held between custom-made fixtures for tensile breaking force text.
Sliding force test
Only V-Loc barbed sutures were used in this test. Manipulated sutures were compared with nonmanipulated sutures to determine if the barb holding force was reduced by robotic manipulation (Fig. 3).

Distribution of samples for pig tissue sliding force test.
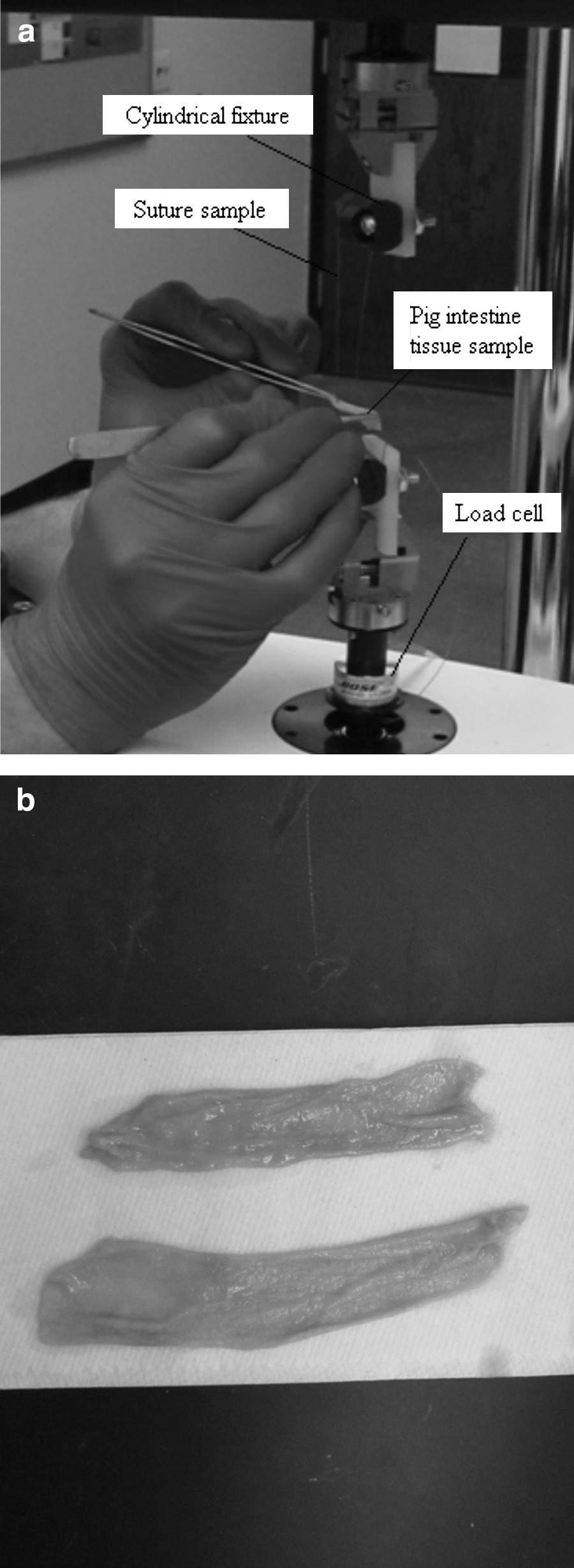
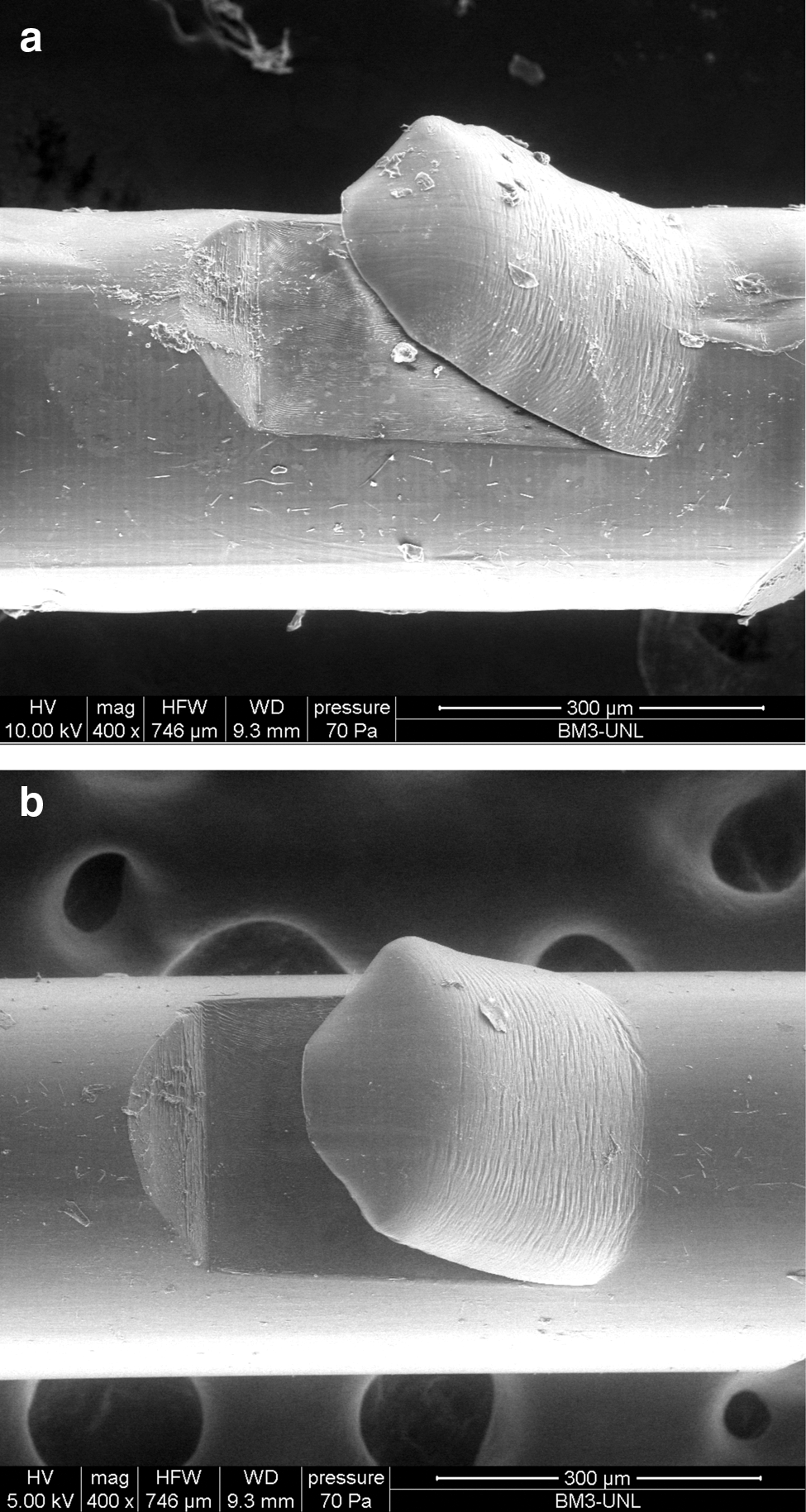
The free end of the V-Loc suture sample was clamped to the BOSE ElectroForce active load cell arm using the same cylindrical custom fixture. The needle was then passed through a section of detubularized fresh porcine small intestine. The needle end was then secured to the opposite passive effector of the load cell. The load on the suture was then tared (zero load condition). Forceps were used to move the porcine small intestine in the direction opposite of the barbs in a vertical fashion. The same person performed all the sliding force tests (KC). The same segment of porcine intestine was used to test a manipulated and nonmanipulated V-Loc suture, but in different locations on the same segment to reduce the possibility of the segment of small bowel affecting the measured sliding force. The peak force that allowed the tissue to “break free” and slide was recorded as the sliding force (Figs. 4a and 4b).
Data analysis
All data were collected electronically and in graph form by the BOSE ElectroForce load testing device software. Sample size was determined by a power analysis with a beta of 0.05 (95% power). Standard t tests were performed to determine if the robotic manipulation created any significant difference in the breaking force or sliding force values. In each case, equal variance values were assumed. A P value of <0.05 was considered statistically significant.
Results
Breaking force test
As expected, the manipulated sutures exhibited a point of failure in the region of the robotic needle driver assault. The nonmanipulated sutures tended to break in random areas outside of the marked area in the center of the suture. Overall, V-Loc demonstrated a lower mean breaking force compared with Maxon.
Robotic manipulation of Maxon (non-barbed) sutures significantly decreased the mean breaking force. The mean difference in breaking forces for manipulated vs nonmanipulated Maxon sutures was 4.52 N (standard deviation [SD]=6.74, P=0.004). A 95% confidence interval (CI) about mean difference in breaking force was 1.91, 7.14. Similarly, robotic manipulation of V-Loc (barbed) sutures also significantly decreased the mean breaking force. The mean difference in breaking forces for manipulated vs nonmanipulated V-Loc sutures was 1.30 N (SD=3.42, P=0.046). A 95% CI about mean difference in breaking force is −0.02, 2.63 (Fig. 5).
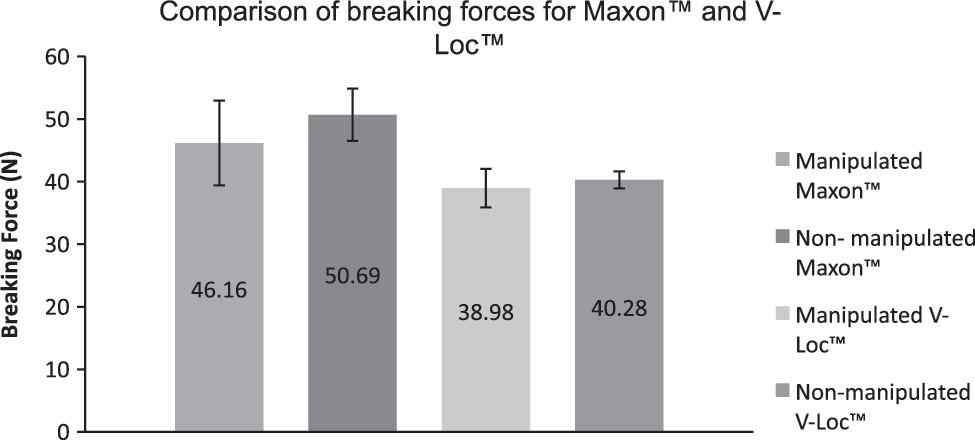
Results of tensile strength in manipulated vs nonmanipulated sutures.
Sliding force test
The manipulated V-Loc group demonstrated a lower peak sliding force compared with the nonmanipulated group (0.76 vs 0.88 N). This difference, however, was not statistically significant (mean difference=0.12, SD=0.49, P=0.199) (Fig. 6).
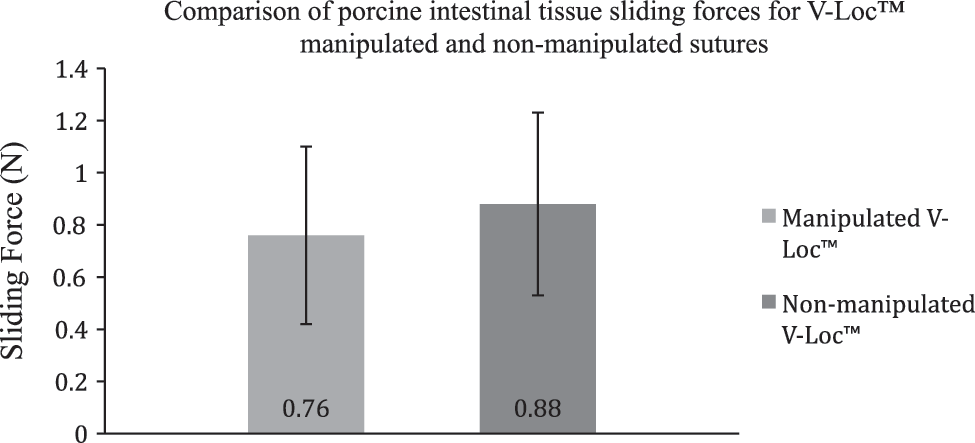
Sliding force test results.
Scanning electron microscopy results
To further characterize the effect of robotic manipulation on V-Loc suture, scanning electron microscopy was performed on both manipulated and nonmanipulated suture. Microscopic structural damage to the suture in the area of the robotic manipulation was evident. Manipulated areas of the suture demonstrated minor crush effect involving both the suture and barb structure (Figs. 7a and 7b). This directly correlates to the finding of decreased breaking force and sliding force of manipulated barbed suture.
Discussion
V-Loc 180 is an absorbable unidirectional barbed suture that has been adopted by many urologists for completing the urethrovesical anastomosis during RARP. It is important to realize, however, that the suture was not originally intended for this purpose. The package insert specifically states not to “crush” or “crimp” the suture material because presumably it could affect its integrity. During laparoscopic or robot-assisted prostatectomy, however, the suture itself is repeatedly grasped with the needle drivers. Therefore, it is important that the mechanical characteristics of the suture after robotic instrument manipulation be well understood.
The current study demonstrates a significant decrease in breaking force of both barbed and nonbarbed monofilament suture after robotic manipulation. This finding is similar to previous studies showing a decrease in tensile strength of braided and monofilament suture after robotic assault. 4 The same results and suture damage have been demonstrated with laparoscopic needle drivers as well. 5
Interestingly, the barbed V-Loc suture demonstrated a lower overall breaking force compared with nonbarbed monofilament suture. While the mean difference in breaking force was significant for manipulated vs nonmanipulated V-Loc suture, the magnitude of this decrease was less for V-Loc compared with Maxon. Therefore, while V-Loc inherently is not as strong as its nonbarbed monofilament cousin, it appears to be less affected by robotic instrument damage. It should also be noted that the barbs are cut into the suture structure, therefore decreasing the suture diameter at the site of the barbs. This could account for the lower overall breaking force for V-Loc compared with Maxon, despite being the same 3-0 caliber suture.
The observed decrease in tensile strength after robotic manipulation can lead to suture breakage during the anastomosis. This could lead to anastomotic leaks and associated problems with strictures, ileus, and infection. Careful attention should be placed on suture tension during the anastomosis. Unfortunately, with the current robotic system, tension must be assessed by visual cues because of a lack of haptic feedback. Such damage to the suture can likely be decreased by not forcefully clamping the jaws of the needle driver closed when handling the suture. In addition, the suture should be handled by the needle whenever possible to prevent unnecessary damage to the suture material.
In the current study, the suture was clamped five times with the robotic needle driver over a 5-cm length. During a typical RARP, we have anecdotally grasped the suture >20 times during an anastomosis over almost the entire length of suture. Hirano and colleagues 6 demonstrated that grasping a suture three times with a large robotic needle driver causes more damage than just one time. It is unclear, however, whether the decreased suture integrity becomes worse each time it is grasped or if it matters more whether it is repeatedly grasped in the same area.
The unique barbed structure of the V-Loc suture also appears to be affected by robotic needle driver manipulation. The damage to the barbs did result in a lower sliding force, but this mean decrease in force was not statistically significant. In this current study, however, the needle driver assault was a simple static maneuver of only closing the jaws on the suture. In vivo, the instrument may slide along the suture, which theoretically could produce more structural damage to the barbs and possibly further decrease barb sliding force.
Fortunately, this decrease in barb sliding force after robotic manipulation is likely not clinically significant either. Several authors have reported series of RARP urethrovesical anastomoses using barbed suture showing them to be safe and effective. Sammon and coworkers 3 recently reported their prospective randomized trial of 33 V-Loc anastomoses vs 31 Monocryl™ (Ethicon, Sommerville, NJ) anastomoses. They found no difference in anastomosis quality or leak rates, but did note a shortened anastomosis time with the barbed V-Loc suture. More than 600 RARP urethrovesical anastomoses had been performed using V-Loc at the time of their publication. Polland and associates 7 found no difference in anastomotic leak rates or incontinence after 6 months follow-up between V-Loc and standard monofilament urethrovesical anastomosis during RARP.
While the decreased strength and sliding force of V-Loc suture after robotic manipulation may not be clinically significant, it is still clinically relevant. As noted above, previous publications have shown decreased tensile strength of monofilament and braided suture after robotic manipulation, but this is the first description of the mechanical characteristics of barbed suture used during robot-assisted surgery. Because this barbed suture is directly grasped with needle drivers during robotic surgery, it is especially important to document that the barb integrity and sliding force are not significantly altered by robotic manipulation.
Conclusion
Robotic manipulation of V-Loc 180 absorbable barbed suture significantly decreases the breaking force of the suture. In addition, V-Loc suture has a lower mean breaking force than standard nonbarbed monofilament suture. Therefore, care must be taken during robotic urethrovesical anastomosis to prevent suture damage and breakage. Furthermore, while the barbed structure of the suture appears to be damaged by robotic instrument manipulation, this damage is likely not clinically significant. Barbed suture will likely become more widely used in the future for robotic urethrovesical anastomoses as a result of this and other recent studies.
Footnotes
Acknowledgment
Product and financial support for testing was provided by Covidien.
Disclosure Statement
This project was supported by a research grant from Covidien.