
Abstract
Background and Purpose:
Laparoscopic partial nephrectomy (LPN) has become a well-established treatment for patients with selected renal malignancies. As the skills of urologic laparoscopic surgeons have increased, more complex and larger tumors are now being approached in this manner. Laparoscopic heminephrectomy (LHN), defined as the resection of >30% of a kidney, is described in this article. Standardized nephrometry scoring is used to grade tumor complexity; complications, renal function, and perioperative outcomes are discussed.
Patients and Methods:
One hundred forty-five patients underwent minimally invasive partial nephrectomy. Parameters studied included patient demographics, tumor characteristics, operative time, estimated blood loss (EBL), length of stay (LOS), clamp time, change in renal function over time, and complication rate using the Clavien system.
Results:
Twenty-four patients underwent LHN. Patients who had LHN performed had significantly larger tumors (4.7 vs 2.6 cm, P=0.05) with higher nephrometry scoring (6.6 vs 5.0, P=0.007). On univariate analysis, both operative (176.0 vs 151.6 min, P=0.036) and clamp time (29.3 vs 21.9 min, P=0.003) were significantly increased. There was no difference in LOS, EBL, change of renal function over time, or complications.
Conclusions:
LHN is efficacious and feasible. Although both operative and clamp times were significantly increased, there was no significant impact on LOS, EBL, change in renal function over time, or complication rate.
Introduction
Most reports of complex LPN have focused on the management of tumors, which abut the renal collecting system or hilum. 5 –7 LPN has also been performed in other complicated scenarios, such as tumors in a solitary kidney, in patients with existing renal insufficiency, and tumors larger than 4 cm. In selected cases, a heminephrectomy technique is necessary for tumor resection. Most reports on laparoscopic heminephrectomy (LHN) involve resection for benign entities as mainly of nonfunctioning moieties of duplex kidneys in the pediatric population. 8,9 There is a paucity of data in the urologic literature on the use of LHN for tumor. In the few reports on LPN for large tumors, none consistently define what constitutes LHN or use standardized complications reporting to compare outcomes with standard LPN.
We report our experience with LHN, when we used this procedure as a true guillotine technique for large polar tumors or a large wedge resection in the interpolar regions of the kidney, resulting in resection of more than about a third (>30%) of the parenchyma in the affected kidney. In this report, we use standardized objective nephrometry scores to grade tumor complexity and the Clavien system to grade postoperative complications as well as assess long-term renal functional outcomes compared with a contemporary series of standard LPNs.
Patients and Methods
Review of our institutional minimally invasive surgical database identified 145 patients who underwent minimally invasive PN (laparoscopic or robotic) by a single surgeon (RG) between 2002 and August 2010. Robot-assisted PN was initiated in January 2010, accounting for eight of the LPN and two of the LHN cases. Twenty-four cases of LHN were identified. In addition, the records of all patients were retrospectively reviewed. A LHN was defined as a complete upper or lower pole PN or a large interpolar tumor resection with a resultant loss of >30% of renal parenchymal tissue (Figs. 1A, 1B).
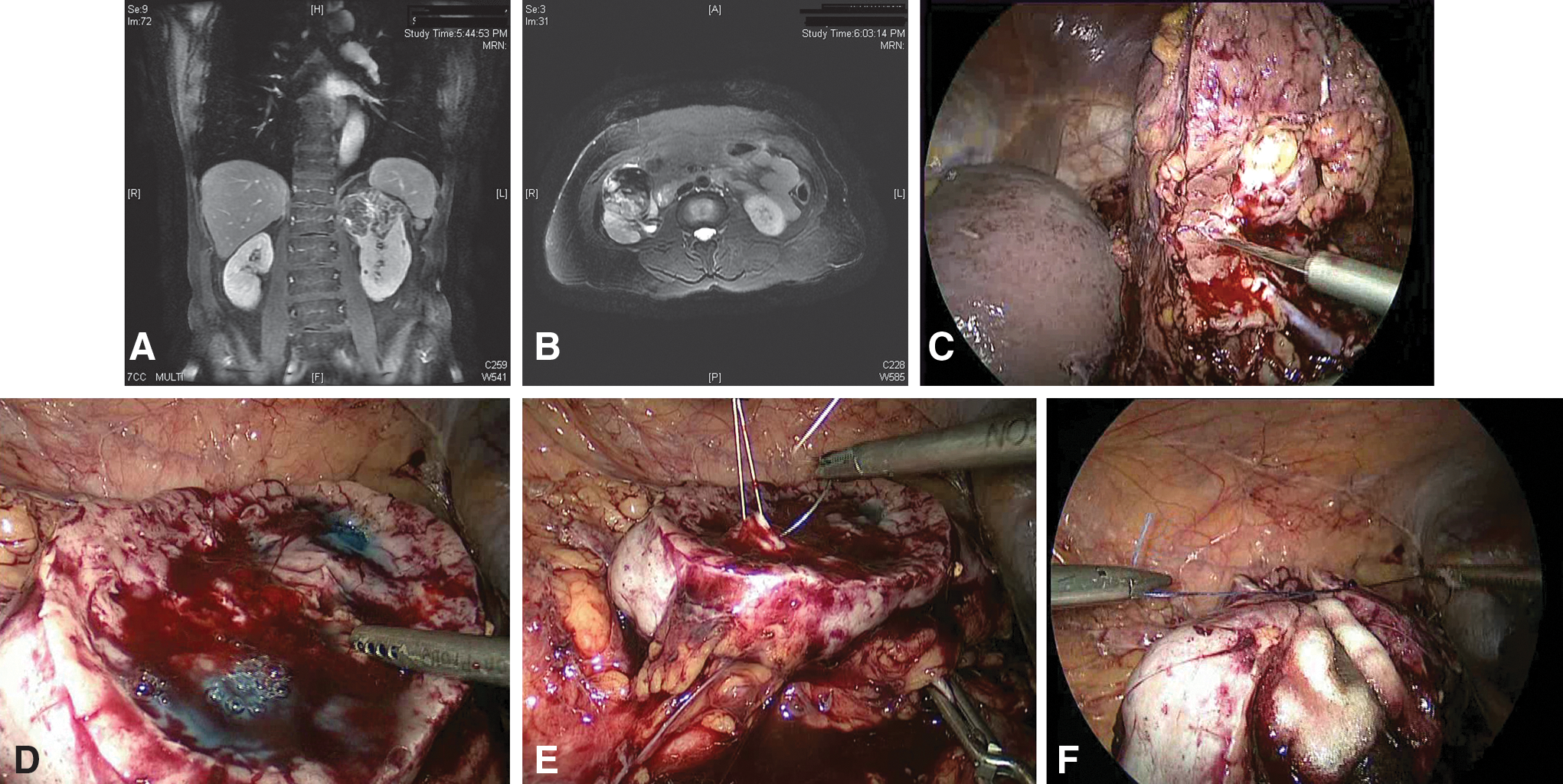
Each kidney was approached via a transperitoneal approach. Hand-assisted surgery was not used in this series. Once the kidney was mobilized and the hilar vessels were dissected, laparoscopic ultrasonography was used to delineate the extent and depth of the renal mass and mark the parenchymal margins for resection. The renal artery(s) and vein(s) were clamped, and dissection of the mass was performed with cold laparoscopic scissors. In large polar resections, a transverse guillotine resection was employed (Fig. 1C).
Because of the location and size of the tumors, the collecting system was entered in all LHN cases. The collecting system was closed using a running absorbable suture at all points of entry. In cases where the tumor abutted the renal hilum and/or extensively involved the renal sinus, with multiple collecting system entries, preoperative retrograde ureteral catheters were placed cystoscopically. Retrograde perfusion of diluted indigo-carmine solution was performed identifying all points of entry into the collecting system, which were then repaired. Floseal® was then applied to the tumor crater for additional hemostasis. The renal parenchymal defect was then closed using absorbable sutures over a hemostatic bolster roll made of oxidized cellulose polymer (Surgicel®) and absorbable gelatin sponge (Gelfoam®) in an interrupted fashion (Figs. 1D, 1E, 1F). In selected cases, a Double-J stent was placed either preoperatively when anticipated or intraoperatively before parenchymal closure. Tisseel® fibrin sealant and a Surgicel blanket were placed over the repaired defect as needed.
Parameters studied included patient demographics, tumor characteristics, operative time, estimated blood loss (EBL), length of stay (LOS), clamp time, change in renal function over time, and complication rate using the Clavien system. 10 Estimated glomerular filtration rate (GFR) was calculated using the abbreviated Modification of Diet in Renal Disease (MDRD) study equation. Postoperative complications were defined as those occurring within 30 days of surgery, including readmission to the hospital. Nephrometry scores, as previously described by Kutikov and Uzzo, 11 were also calculated for all renal tumors. This standardized reporting system is based on cross-sectional imaging and uses (1) tumor diameter, (2) exophytic or endophytic properties, (3) nearness of the tumor to the collecting system, (4) anterior or posterior tumor, (5) location relative to polar lines, and (6) whether the tumor is hilar to give an objective score (of 12) for each tumor. All images were reviewed by one independent scorer to decrease variability and increase objectivity.
Both univariate (Student t test, chi-square) and multivariate analyses (linear regression) were conducted comparing outcomes in our LHN and standard LPN cases. Differences between the groups was considered significant at P<0.05. Factors controlled for in multivariate analysis were Charlson Comorbidity Index Score (CCS), body mass index (BMI), sex, race, and age at surgery. The primary outcome for this study was oncologic outcome related to margin status at the time of surgery and recurrence rate. The secondary outcome was renal functional change after surgery.
Results
Patient characteristics are shown in Table 1. There were no significant differences in the groups with regards to age, race, sex, CCS, BMI, or tumor location. Unsurprisingly, nephrometry scores were significantly greater in the LHN vs LPN group (6.6 [5.8–9.0] vs 5.0 [3.0–7.0], P=0.007). Tumor size was also significantly higher in the heminephrectomy group, and T stage was significantly different between groups. There were no positive surgical margins or local recurrences noted in either group.
Refers to significant results, P<0.05
LPN=laparoscopic partial nephrectomy; LHN=laparoscopic heminephrectomy; BMI=body mass index; CCS=Charlson Comorbidity Index Score; GFR=glomerular filtration rate.
On univariate analysis, both mean operative time (176 min vs 152 min, P=0.036) and clamp time (29.3 min vs 21.9 min, P=0.03) were significantly increased with LHN compared with LPN. However, EBL, LOS, and change in renal function were no different when comparing the two (Table 2A). The average follow-up to determine change in renal function was 17 months (interquartile range 4–33.7) in the LHN group and 23 months (6–23) in the LPN group.
On multivariate analysis (Table 2B), controlling for CCS, BMI, sex, race, and age at surgery, clamp time was significantly greater by 7.0±2.5 minutes (standard error of the mean) (P=0.006). There was no increase in the overall rate of complications in this group of patients (P=0.271) (Table 3). There were no deaths or life-threatening complications.
Refers to significant results, P<0.05
LHN=laparoscopic heminephrectomy; LPN=laparoscopic partial nephrectomy; MDRD=Modification of Diet in Renal Disease.
LPN=laparoscopic partial nephrectomy; LHN=laparoscopic heminephrectomy.
Grade IIIa complications in the LPN group included three patients who needed angiography and embolization for either pseudoaneurysm formation or bleeding postoperatively. Grade IIIb complications included five patients who needed ureteral stent placement for persistent urinary leakage from the repair and one patient who needed a reoperative nephrectomy for hemorrhage. Grade IIIa complications in the LHN group included one patient who needed angiography for a postoperative pseudoaneurysm. Grade IIIb complications included one patient who needed ureteral stent placement for persistent urinary leakage from the repair. Two patients needed the procedure converted to open surgery secondary to a technically difficult operation.
Discussion
In the past, large, endophytic and hilar tumors of the kidney have been managed with RN or open PN. This has been because of the concern over the potential resectability of the tumor in the case of RN or concern over the feasibility of renorraphy in PN. As urologic laparoscopic skills and techniques have improved, however, it is now feasible to approach many of these more complex lesions via a minimally invasive approach. 5 Recently, Porpiglia and associates 12 described a series of LPN for large renal masses in experienced hands. This was a multi-institutional European study, which studied the outcomes of LPN for tumors 4 to 7 cm in diameter with a mean tumor size of 4.7 cm. It was determined that a LHN, defined as >30% kidney resection, was performed in 11/63 (17%) cases. Perioperative outcomes such as operative time (152 min), warm ischemia time (25.7 min), EBL (230 mL), and a complication rate of 26% were in line with the current study. It was determined that this is an acceptable method for surgeons with experience; however, there were increased complication rates in those patients with more endophytic tumors. A significant limitation of this was incomplete data because of the multi-institutional nature of this study and no standard definition of complexity and complications reporting.
Gill and colleagues 5 also have published data regarding LPN in a series of 25 patients with complex LPNs characterized by hilar tumors. Mean tumor size was 3.7 cm. Perioperative outcomes included EBL (231 mL), warm ischemia time (36.4 min), and operative time (216 min). Complications were recorded in 20% of patients. Renal scans were obtained at 1 month postoperatively, but no long-term renal functional outcomes were determined.
In the only other series besides our current report that specifically addressed outcomes for patients undergoing LHN, this procedure was performed in 41 patients and compared to a cohort of patients who underwent LPN. 13 This was a single-center series, which used a similar definition of heminephrectomy. Mean tumor size was 3.7 cm in LHN vs 2.3 cm in LPN group. Patients had comparable operative times and EBL. Warm ischemia times, however, were longer in the LHN group (39 vs 33 min). Tumors were more centrally located, deeply infiltrating, and necessitated larger parenchymal resections in the LHN group. At the time of that report, however, no standardized methods of tumor complexity reporting (nephrometry scores) was available. The authors used subjective assessments of complexity on preoperative cross-sectional imaging. The overall complication rate was 20% vs 17%; however, again, no standardized system was used to grade these complications. Postoperatively, serum creatinine values were similar between the LHN and LPN groups, but long-term change in renal function was not determined and in general, unlike our current study, renal function was not assessed using the MDRD equation.
Our series of LHN shows that, in experienced hands, large complex tumors, often abutting the collecting system, renal sinus, or hilum can be managed with a laparoscopic approach even when a >30% of resection of renal parenchyma is necessary. Our results are comparable to previous studies of either complex LPN or LHN. In contrast with previous studies, our data add standardized complication reporting, nephrometry scoring, as well as long-term renal functional outcomes. The only significant variables that differed in this series were operative and clamp time; however, there were no differences when comparing EBL, LOS, or change in renal function over time. The overall rate of complications did not differ significantly when comparing LHN and LPN. Because of the small numbers, an analysis of the severity of complications could not be performed.
Extensive collecting system entry in this series of LHN did not translate into a higher urinary leak rate. Given the deep parenchymal resection and theoretically division of deep segmental vessels, hemorrhage and transfusion rates were not different with standard LPN. Some technical points merit mention in performing LHN. Complete mobilization and definition of circumferential tumor resection margins and use of intraoperative ultrasonography are key. Use of preoperative retrograde infusion of diluted indigo carmine, use of ureteral stents after the completion of the resection, and control of larger segmental vessels during resection of the tumor with Hem-o-lok clips or figure of eight sutures are significant maneuvers to prevent complications. Polar vessels or vessels that clearly supply the parenchymal segment being resected can and should be individually controlled and ligated.
Because most tumors involved major segmental vessels, nonischemic partial nephrectomy was not considered. Also, because of the extent of parenchymal resection, the size of the tumor crater and the often irregular contour of the deep parenchymal margin of the tumor mass, four quadrant tumor crater frozen section biopsies are helpful to ensure negative margins. In cases of massive upper pole tumor burden in which the adrenal gland is effaced, en-bloc adrenalectomy with upper pole LHN can be performed as also reported by others. 14 Finally, if possible, consideration of resection angles is important to ensure that the parenchymal edges of the resultant tumor crater can be easily approximated for a hemostatic closure.
Limitations of this study include the retrospective nature of the study. In addition, the experience of the surgeon has changed over time. As a result, the majority of procedures for the more complex tumors were performed toward the end of the series. Although the number of LHN is relatively small and this may lead to limitations of our analyses, it is in line with previous studies of complex renal masses managed with LPN. Prospective multi-institutional studies will be needed to further investigate the feasibility and outcomes of patients with large complex renal tumors undergoing LPN.
It is important to state that in appropriately selected patients, nephron-sparing surgery is the ultimate goal of the surgical intervention. The feasibility of LHN points out the fact that a minimally invasive option is available to emulate open nephron-sparing surgery to complete this complex surgical task with acceptable renal functional outcomes. Studies have determined that patients undergoing RN have a significantly higher risk of development of chronic kidney disease than those undergoing partial nephrectomy. 15,16 Therefore, laparoscopic RN should not be used as the only minimally invasive alternative for these tumors. When the laparoscopic experience is available, LHN can be safely attempted. If that expertise is not available, however, open PN when feasible has to be used as the more appropriate option for nephron preservation. Laparoscopic RN should only be used when minimally invasive or open PN is not feasible.
With the advent of robotic technology and its increasing use in minimally invasive urologic surgery, more surgeons comfortable with this technique may opt to perform renal surgery in this manner. As opposed to traditional laparoscopic methods, robot-assisted surgery reduces the complexity of dissection and renal reconstruction through the use of magnified stereoscopic visualization and fully articulating instruments. 17 In addition, adjunct technologies, including improved intraoperative ultrasonography and preoperative imaging at the console for review, allow for better surgical planning and execution. As this technology becomes more widespread for use in PN, future studies will need to address the ultimate functional and oncologic outcomes of this new technique.
Conclusion
LHN for large, complex tumors necessitating major parenchymal resections is feasible and efficacious compared with routine LPN. Although LHN is associated with increased operative and warm ischemia times, there was no impact on LOS, EBL, or long-term renal function. In addition, LHN and routine LPN had comparable complication profiles. In experienced hands, LHN and resultant renal reconstruction can be safely performed for appropriately selected patients.
Footnotes
Disclosure Statement
No competing financial interests exist.