
Abstract
Surgical absence of the prostate can make placement of fiducial markers difficult, because anatomic landmarks are distorted and there is a paucity of substantial tissue to hold fast the markers. We describe a method for improving the accuracy of fiducial marker placement for the purpose of salvage or adjuvant external beam radiation therapy for prostate cancer in patients who have undergone radical prostatectomy. To assist with identification of the urethrovesical junction and to facilitate placement of the markers, a Foley catheter was placed and the balloon was inflated. Gentle traction on the catheter seated the balloon at the bladder neck to echographically define the anatomy of the urethrovesical junction. Next, a rectal ultrasound probe was inserted into the rectum, allowing visualization of the region of the urethrovesical junction. Fiducial markers were then placed bilaterally in the detrusor muscle at the bladder neck or in the periurethral tissue using the applicator needle. The treating radiation oncologist verified that marker placement was suitable for assisting with radiation therapy in all cases. Preradiation pelvic imaging verified that markers were not in the bladder or urethral lumen, and there were no patient complaints of voiding out the markers with urination.
Introduction
Our close collaboration with the Department of Radiation Oncology has determined that, ideally, two markers should be placed at the urethrovesical junction (UVJ), one on the right and one on the left, so that there is enough space between them to avoid an additive effect of the 10% dose decrease (shadowing effect) in the immediate vicinity of each marker with protons (not an issue with photons). Two additional markers should be placed more superiorly in the area of the proximal seminal vesicles, separated to the right and left of midline. This is important because the motion of the prostate bed is different at the level of the UVJ and more superiorly in the seminal vesicular area in postprostatectomy patients. For patients treated with protons, markers on the left and right should also be staggered in the superior to inferior direction so that they do not overlay one another on a lateral “beams-eye view” projection.
Technique
Before planned salvage or adjuvant photon or proton radiation therapy for prostate cancer, gold fiducial markers were placed at the request of the radiation oncology department. To assist with identification of the UVJ and to facilitate placement of the markers, a Foley catheter was placed, and the balloon was inflated with 10 mL sterile water. Next, a rectal ultrasound probe was inserted into the rectum; while gentle traction on the catheter seated the balloon at the bladder neck to echographically define the anatomy of the UVJ (Fig. 1). Approximately 2 mL of 1% lidocaine were injected at the intended sites of marker insertion using a 22-gauge spinal needle. One or two markers were then placed on each side in the detrusor muscle at the bladder neck or in the periurethral tissue using the applicator needle (Fig. 2). The rectal ultrasound probe and Foley catheter were then removed.

Sagittal transrectal ultrasonographic view of the Foley catheter seated at the urethrovesical junction (UVJ).
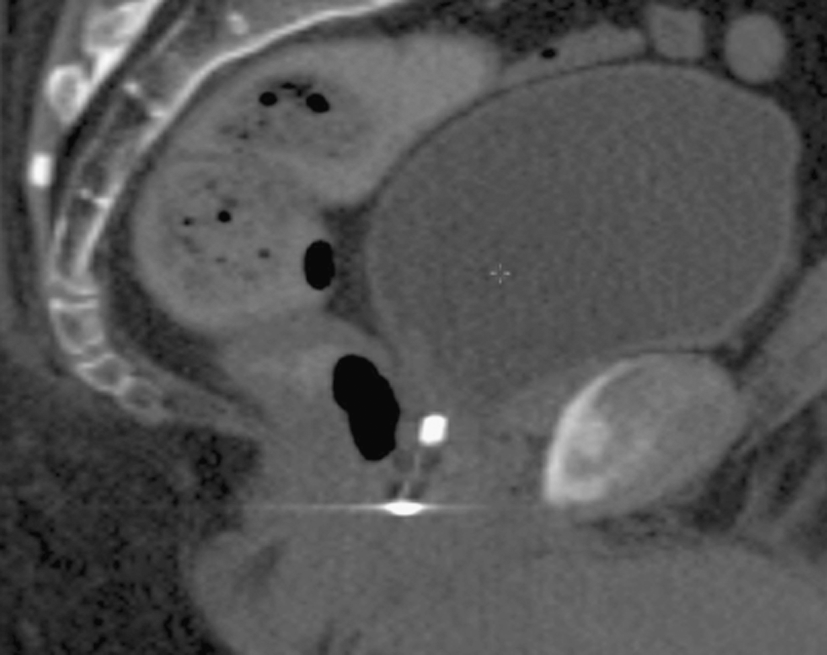
Sagittal noncontrasted computed tomographic view of fiducial markers placed at the level of the urethrovesical junction and membranous urethra.
With Institutional Review Board approval, the medical record was reviewed to identify patients who had undergone fiducial marker placement in this manner before planned photon and or proton adjuvant or salvage therapy for prostate cancer at our institution since 2007. Thirty-one patients had markers placed in this fashion. The treating radiation oncologist verified that marker placement was suitable for assisting with radiation therapy in all cases. Preradiation pelvic imaging verified that markers were not in the bladder or urethral lumen, and there were no patient complaints of voiding out the markers with urination, consistent with the literature regarding minimal migration of fiducial markers in the postprostatectomy setting. 1
Discussion
This technique is easily incorporated into the procedure for placing fiducial markers in the postprostatectomy setting. It adds minimal cost and discomfort to the procedure, while significantly facilitating this often very frustrating procedure by quickly and definitively identifying the UVJ. This technique can be recommended to all urologists who place fiducial markers in the postprostatectomy setting.
Footnotes
Disclosure Statement
No competing financial interests exist.