
Abstract
Transurethral resection of bladder tumor (TURBT) is the standard of care for initial bladder tumor management. In response to its shortcomings, we propose an alternative technique for tumor resection and retrieval: The endoscopic snare resection of bladder tumor (ESRBT). Eleven tumors managed by ESRBT were reviewed retrospectively. Via cystoscopy, tumors were resected en bloc with an electrosurgical polypectomy snare and retrieved transurethrally. Safety and efficacy were assessed by clinical and pathologic outcomes. ESRBT was highly effective for appropriate tumors. Tumor size and location varied: Two small, six medium, three large; six lateral wall, two dome, two trigone, one posterior wall. Half of initial urothelial carcinoma specimens contained muscle. There were no intraoperative or postoperative complications (mean follow-up: 17 mos; range 10–25 mos). ESRBT is a feasible technique for the resection of pedunculated bladder tumors. It offers evident and theoretical advantages over TURBT and may augment bladder tumor management. Further study is needed.
Introduction
Despite its shortcomings, the basic technique of TURBT has changed very little since the introduction of the first resectoscope in 1931. 7 Traditional TURBT is performed in a piecemeal fashion with sequential swipes of the resectoscope. This “incise and scatter” method causes bleeding, impairs visualization, and most importantly, violates the basic oncologic surgical principle of en bloc resection. 8 It has been suggested that by scattering and potentially seeding tumor throughout the bladder, TURBT may contribute to the high recurrence rates seen in bladder cancer. 7,9
Several promising alternative techniques, including en bloc and snare resection, have been proposed to address these problems; however, none has gained wide acceptance or adaptation. 7,10 –14
We present endoscopic snare resection of bladder tumor (ESRBT), an en bloc method of transurethral resection and specimen retrieval using an electrosurgical polypectomy snare and mesh net.
Technique
Records of nine consecutive patients (11 bladder tumors) who were treated by ESRBT between November 2009 and December 2010 were reviewed retrospectively. Bladder tumors were diagnosed preoperatively on office cystoscopy. Inclusion criteria included patients with a first-time diagnosis of bladder tumor. Exclusion criteria included patients with sessile tumors or those referred for re-staging TURBT. The series represents a single-surgeon experience at a university teaching hospital. The surgeon's referral base consists mainly of complex cancer cases; hence, the infrequency of simple papillary tumors in the series (Fig. 1).

Step-by-step illustration of endoscopic snare resection of bladder tumor (ESRBT). A pedunculated bladder tumor is identified
• Under cystoscopic guidance, the bladder tumor is identified.
• The snare is advanced through the scope's working port and into the bladder.
• The snare loop is opened, lassoed around the tumor, manipulated down to and completely around the base of its stalk, and gently tightened. Special attention is paid to ensure that uninvolved bladder mucosa is excluded from the snare's loop.
• Gentle traction and cutting current (80–120 V) is applied to the snare, amputating the tumor stalk at its base. The tumor is allowed to fall to the bladder floor.
• The resection site is inspected for bleeding (generally little or none).
• The tumor is retrieved by one of two methods, either directly with the snare (small tumors) or with an endoscopic mesh net (medium and large tumors).
- With the tumor secured in the snare, the snare and scope are withdrawn from the bladder together.
- Alternatively, the bladder tumor is resected and allowed to fall to the bladder floor. An endoscopic retrieval net is advanced through the scope's working port into the bladder and opened. The tumor is easily captured in the net. The net and scope are withdrawn from the bladder together. Note: Before developing the net method of specimen retrieval, if the specimen was too large to remove en bloc, it was bisected with the snare's electrocautery and then removed in separate pieces.
• The tumor base is biopsied with a rigid cold cup biopsy forceps.
• The biopsy site is fulgurated with a Bugbee electrode.
Equipment
• 21F rigid cystoscope
• 7F monopolar polypectomy snare
• Multipurpose endoscopic mesh net
• Rigid biopsy forceps
• Bugbee electrode
• Power supply and cords
• Resectoscope (no longer used)
Role in Urologic Practice
Results
A total of 11 tumors from nine patients were treated by ESRBT, including 8 papillary urothelial carcinoma (UC), 2 metastatic melanoma, and 1 metastatic renal-cell carcinoma. All tumors were resected en bloc with minimal bleeding and minor trauma to the bladder wall. Tumors ranged in size: Two small (<2 cm), six medium (2–5 cm), and three large (>5 cm). Tumor location included six lateral wall, two dome, two trigone (adjacent to ureteral orifice), and one posterior wall. All UC tumors were nonmuscle-invasive, including five high-grade, two low-grade, and one nondiagnostic. Of these, detrusor muscle was present in 50% of the initial ESRBT specimens and 100% of tumor base biopsies analyzed. Tumor architecture preservation was generally excellent (Fig. 2).
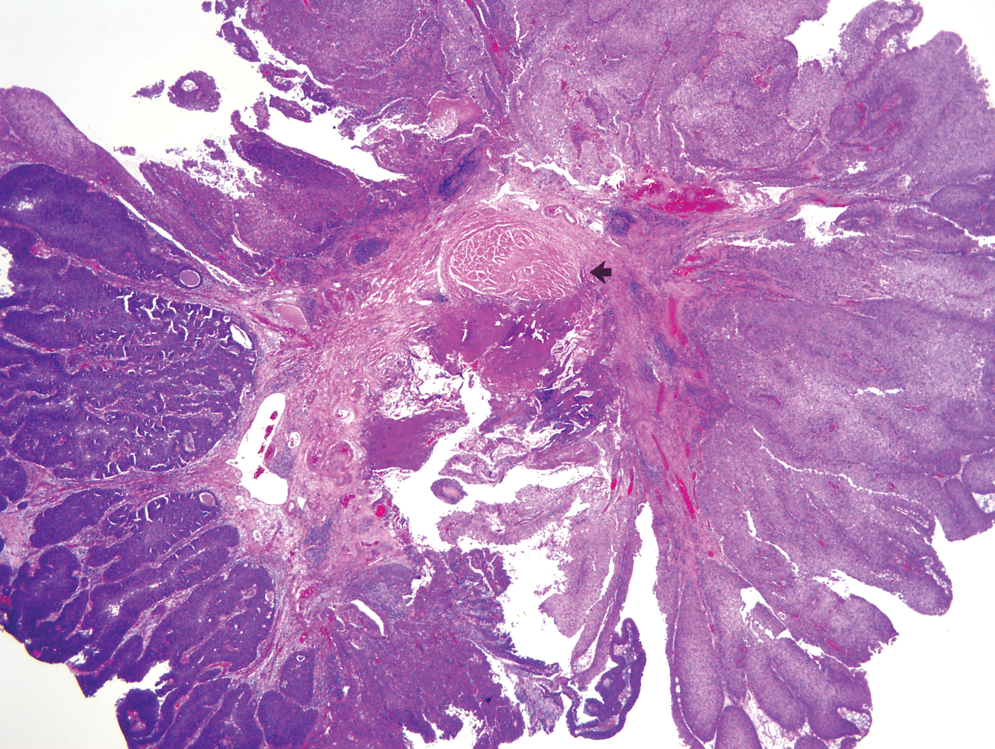
Histologic findings in bladder tumor resected by ESRBT. A large papillary urothelial neoplasm surrounds a central area of lamina propria and a small portion of detrusor muscle (arrow). Examination of an intact specimen, as illustrated, facilitates orientation of the tumor with the underlying structures and in difficult cases may help to determine the stage of the tumor more accurately.
Pathologic interpretation of tumor grade was limited in one specimen because of crush injury (very small tumor). Pathologic interpretation of muscle invasion was limited in two specimens from the same patient because of electrocautery injury (very small tumor) and from the use of electrocautery during bisection (large tumor). No intraoperative or postoperative (on 2-week follow-up) complications were identified, including significant bleeding, bladder perforation, obturator reflex, or ureteral injury. On long-term surveillance of UC patients (N=7), no long-term complications were identified, while tumor recurrence ultimately developed in 57% of patients (mean follow-up: 17 mos; range 10–25 mos) with a mean time to first recurrence of 12 mos (range 3–25 mos).
Discussion
Traditional TURBT is associated with high rates of incomplete resection, understaging, and tumor recurrence. Furthermore, it violates the oncologic principle of en bloc resection. To the best of our knowledge, no other tumor is resected in a top-down piecemeal fashion—that is, by cutting into the tumor and dispersing the tumor cells throughout the organ or body. This approach may contribute to the high recurrence rate seen after TURBT. Piecemeal resection also promotes bleeding and impairs visualization, possibly leading to prolonged procedure times because of frequent clot evacuation, incomplete resection of the base, or imprecise resection of the base with perforation. Given its shortcomings, we contend that TURBT, our current standard of care, deserves reevaluation.
ESRBT is easy to perform and can be applied throughout the bladder. It greatly simplifies resection of medium, large, and especially vascular tumors. ESRBT avoids bleeding, improves visualization, and minimizes the surgical footprint left on the bladder wall. By amputating the bulky papillary distal tumor portion first, ESRBT allows for a more accurate biopsy of the tumor base, which ensures inclusion of detrusor in the pathologic specimen. Besides these concrete benefits, ESRBT offers the theoretical advantages of en bloc resection—namely, preserving tumor architecture and limiting tumor dispersal. We suspect that, by limiting tumor seeding, ESRBT may lower recurrence rates; however, the present study was not designed to address the efficacy of ESRBT and therefore does not support this claim.
It is important to note that ESRBT is only effective on pedunculated tumors. Smaller and sessile tumors are less amenable to this technique because it is technically difficult to amputate these tumors, and as we learned in two cases, pathologic assessment is compromised. In our experience, sessile tumors necessitate the use of a resectoscope, and small tumors are best resected with a rigid biopsy forceps.
We were able to obtain muscle in half of our UC specimens by ESRBT alone; however, theoretically, the tumor stalk should not contain detrusor muscle. We postulate that two factors may have permitted inclusion of detrusor muscle within the snare: (1) The application of direct pressure to the bladder wall with the thin wire snare may allow deeper tissue to protrude distal to the level of the snare like a cookie cutter imprinting dough, and (2) for those tumors arising from the anterior half of the bladder, the tumor's own weight may assist in tenting the deeper tissue into the lumen of the bladder distal to the level of the snare like a water balloon being filled from a faucet. Nevertheless, to ensure correct staging, the base of the tumor should undergo biopsy for complete resection and detrusor muscle sampling after initial amputation with the snare. We strongly believe that directed biopsy of the tumor base should be considered an advantage of ESRBT.
For larger tumors, we demonstrated the ability to capture the tumor with a retrieval net. Before discovering this tool, we divided larger specimens with the snare to facilitate removal, a technique that we no longer use because of its violation of the tumor integrity and its detrimental effects on pathologic assessment. While the tumor must temporarily sit on the bladder floor before it can be retrieved with the net, we feel that this aspect of ESRBT is not incompatible with the notion of en bloc resection, because it differs very little from the natural state of the tumor in the decompressed bladder before resection. The management of large tumors resected by ESRBT, however, still needs refinement, especially for tumors that may be too large to remove intact via the urethra.
This study demonstrates that ESRBT is a feasible approach for resecting pedunculated bladder tumors. It is intended to supplement rather than replace current bladder tumor management. Further investigation is warranted.
Footnotes
Disclosure Statement
Dr. Ponsky is a member of the safety monitoring boards of Accuray Inc. and Tengion Inc., and is a consultant for US Endoscopy and Varian Medical Systems. For all other authors, no competing financial interests exist.