
Abstract
Background and Purpose:
Investigators have reported that men undergoing radical retropubic prostatectomy (RRP) for prostate cancer (PCa) can experience significant changes in nocturia after surgery. We examined the effect of robot-assisted laparoscopic prostatectomy (RALP) on nocturia symptoms in men with PCa from baseline to 1-year follow-up.
Patients and Methods:
Between August 2006 and August 2010, 116 patients undergoing RALP for clinically localized PCa had baseline and 1-year Expanded Prostate Cancer Index Composite (EPIC) questionnaire data obtained. Patients were divided into three groups with respect to nocturia: N1 (0 or 1 episode per night), N2 (2 episodes per night), and N3 (3 or more episodes per night).
Results:
N1 (63 patients) had stable or worsened nocturia with 78% of patients retaining their N1 status, 21% progressed to N2 status, and 2% progressed to N3. N2 (29 patients) were 52% N1, 34% N2, and 14% N3 after surgery. The N3 (24 patients) had 29% improved to N1, 38% improved to N2, and 33% remained N3. EPIC urinary function and incontinence subscale scores were 92.3 and 91.3 preintervention and 85.2 and 76.6, (P=<0.001 for both), respectively, at follow-up. The combination of improved obstructive symptomatology and continence after RALP resulted in no net change in urinary bother.
Conclusions:
RALP is associated with improved symptomatology in patients with the greatest level of preinterventional nocturia. Patients with minimal preoperative nocturia may experience worsening of nocturia.
Introduction
Previously, Namiki and associates 11 evaluated symptoms of nocturia in 120 men after radical retropubic prostatectomy (RRP). Of particular interest, the authors noted that while overall voiding bother scores improved after RRP, there was evidence of a deleterious effect on nocturia and voiding frequency for men with mild preprocedure symptoms. This observation led the authors to hypothesize that the wide anatomic dissection around the prostate during RRP may disrupt the afferent and efferent innervation of the trigone and bladder neck causing partial denervation of the detrusor muscle, which could lead to increased nocturia. 11,12 Motivated by the observations of Namiki and colleagues, 11 we examined whether the bladder mobilization techniques, bladder neck dissection, and anastomotic principles used during robot-assisted laparoscopic prostatectomy (RALP) resulted in improved postoperative nocturia after surgery for PCa.
Patients and Methods
Institutional Review Board approval was obtained prior to the initiation of this study. We identified 116 patients who underwent RALP for clinically localized (TxN0M0) PCa and had both baseline and 1-year questionnaire data available for analysis. All patients were informed that their participation in this study was observational and would not dictate or affect standard pre, peri and postoperative care. We abstracted demographic and clinical information including age, body mass index (BMI), marital status, presence or absence of diabetes, presence or absence of erectile dysfunction, use of antihypertensive medications, and history of stroke or Parkinson disease from our registry database. In addition, we also abstracted baseline and 1 year postoperative scores for the Expanded Prostate Cancer Index Composite (EPIC) questionnaires and American Urologic Association (AUA) symptom questionnaire.
For our analysis, we first linearly transformed all scores on the EPIC questionnaire to a scale of 0 to 100, where higher scores indicate better quality of life. We then calculated the mean change from baseline to 1 year for total AUA score, total EPIC score, the score for each of the four EPIC subscales, and the scores for the individual questions 8 to 14 on the EPIC questionnaire. To evaluate the change from baseline to 1 year, we performed signed rank tests and examined the associated P values.
For our analysis focused specifically on nocturia, we classified the men into three groups based on their responses to question 14 of the EPIC questionnaire (How many times did you most typically get up to urinate from the time you went to bed at night until the time you got up in the morning?) at baseline and at 1 year. That is, for both the baseline and 1-year time point, we calculated the percentage of men who experienced 0 or one nocturia episode per night (N1), two episodes per night (N2), or three or more episodes (N3). To take advantage of our paired data (ie, two time points on each man), we calculated the percentage of men whose N category got worse, stayed the same, or improved from baseline to 1 year. Finally, for visual representation, we constructed bar graphs stratified by baseline N group showing the scores on question 14 before and after surgery.
All statistical tests were two-sided, and threshold of significance set at p=0.05. All statistical analyses were performed using SAS Version 9.2 (SAS Institute, Cary, NC).
Results
All RALPs were performed by one of three surgeons at our institution. Each procedure was performed via a standard robotic transperitoneal approach with nerve sparing when clinically appropriate. A majority of the patients underwent unilateral or bilateral nerve-sparing operations. The operation was performed without anterior or posterior pelvic reconstruction (Rocco stitch). Anastomosis were completed in a running Van Velthoven fashion with double-armed 3-0 monofilament suture. 13 All patients were placed on the same postoperative pathway with the target discharge to home being postoperative day number 1 with catheter removal on postoperative day number 7 to 10. Cystography was not completed before catheter removal.
Table 1 provides an overview of demographic and clinical characteristics for our study population. The mean age of the men in our study was 63.3 years (min 46, max 77); 64% (74/116) were >65 and 36% (42/116) were ≤65. The mean BMI was 27.5 kg/m2 (min 19.9, max 37.6). Documented medical comorbidities included diabetes in 8% of men (9/116). Ninety-one percent (106/116) of patients had T2 disease, 9% (10/116) had T3 disease.
The sample median (mininum, maximum) is given for continuous variables; N (%) for categorical variables.
BMI=body mass index; ED=erectile dysfunction; AUA=American Urological Association; PSA=prostate-specific antigen.
Table 2 provides our comparison of mean AUA symptom score, urinary function scores, and urinary symptoms at baseline and 12 months postsurgery. The mean AUA symptom score for the overall group improved from baseline to 1 year (6.7 vs 5.0; P=0.002). Of note, 66 (55%) patients reported improved AUA score, 9 (8%) reported no change, and 44 (37%) reported a worse AUA score (data not shown). EPIC urinary function and incontinence subscale scores were 92.3 and 91.3 preintervention and 85.2 and 76.6, (P=<0.001 for both), respectively, at 1-year follow-up. Interestingly, these two changes did not result in an overall change in mean EPIC total urinary function scores (86.9 to 85, P=0.16) or EPIC urinary bother scores (82.7 to 84.1, P=0.30). For the individual questions 8 to 14 on the EPIC questionnaire, we observed improvements in the mean score for the questions related to emptying, voiding frequency, intermittency, weak stream, and hesitancy (all P values <0.05). Conversely, there was no evidence of changes in mean score for the question related to nocturia (P=0.23) and urinary urgency (P=0.84).
N=116.
N=106.
N=104.
P values based on the signed rank test.
SD=standard deviation; F/U=follow-up; AUA=American Urological Association; EPIC=expanded prostate cancer index composite.
For all patients undergoing RALP, the percentage of men classified as N1 (none to 1 episode at night) increased from 56% to 61% while the percentage classified as N3 (3 or more episodes at night) dropped from 20% to 13%. More importantly, based on the paired scores for each man, 59% of patients had no change in N category from baseline to 1 year, whereas 17% reported a worse N category and 24% reported an improvement in N category. Figure 1 represents a distribution of nocturia symptom scores before and after RALP stratified by baseline N group. The N1 group (63 patients) had 78% of patients retain N1 status, 21% progress to N2, and 2% progress to N3. The N2 group (29 patients) had 52% improve to N1, 34% remain at N2, and 14% worsen to N3. The N3 group had 29% improve to N1, 38% improve to N2, and 33% remain at N3.
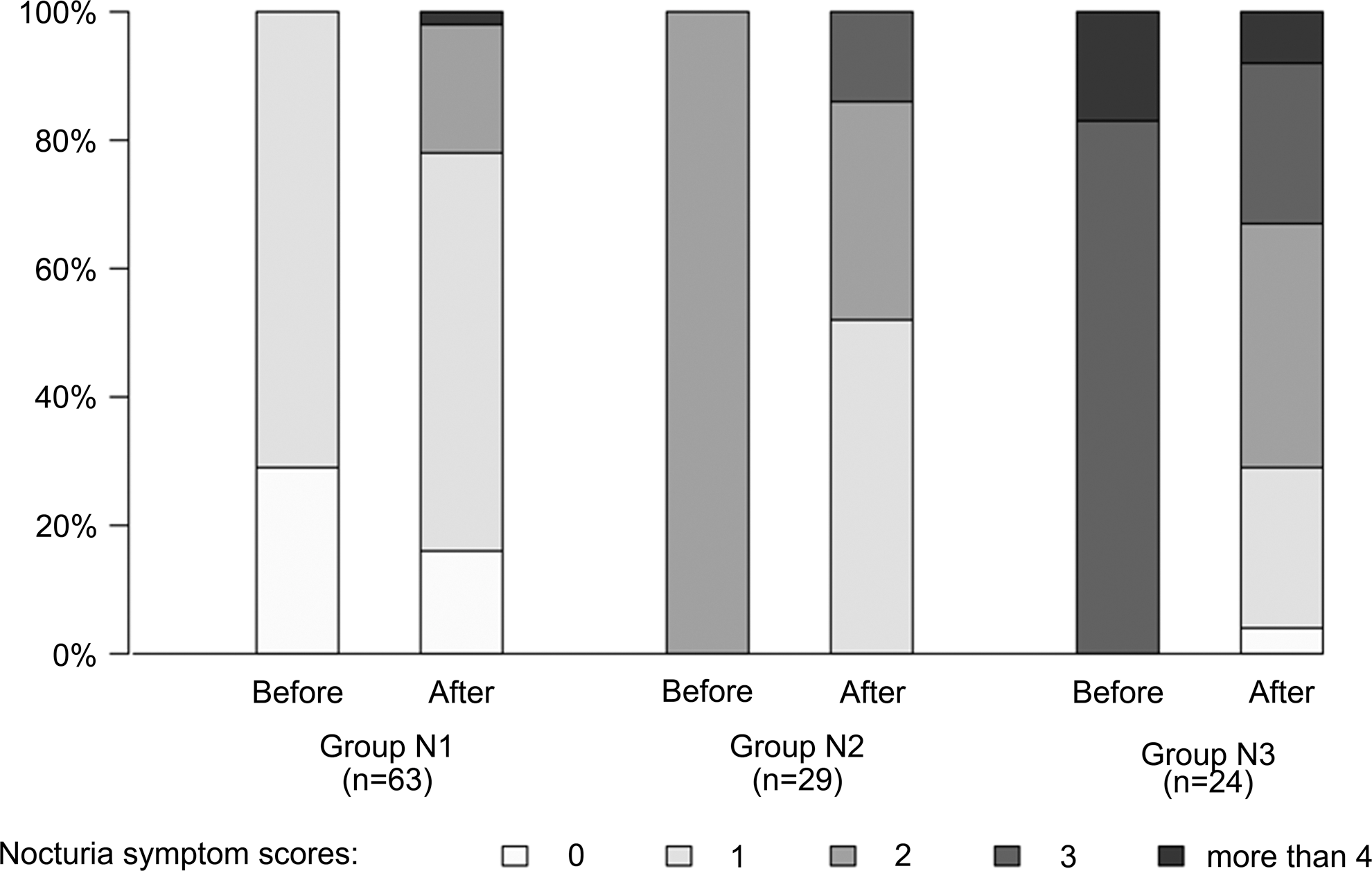
Distribution of nocturia symptom scores before and after robot-assisted laparoscopic prostatectomy, stratified by baseline scores: N1 with scores of 0 or one time, N2 with a score of two times, N3 with scores of three or more.
Discussion
Previous investigators have noted that PCa patients with significant preoperative nocturia are likely to improve after RRP 11 ; however, patients without significant urinary bother or preoperative nocturia can worsen after RRP. Namiki and coworkers 11 used data on 120 patients after RRP to report improved overall voiding bother scores but a deleterious effect on nocturia and voiding frequency in a subset of men with mild preprocedure symptoms. Based on this observation, the authors hypothesized that the wide anatomic dissection around the prostate during RRP may disrupt the afferent and efferent innervation of the trigone and bladder neck to cause partial denervation of the detrusor muscle. This denervation may be the reason for the sphincter weakness, impaired detrusor contractility, and decreased compliance seen in patients after RRP. 14 That being said, what remains unclear is whether the bladder mobilization techniques, bladder neck dissection, and anastomotic principles used during RALP translate to similar urinary results postsurgery.
We report for the first time that RALP leads to similar effects on urinary symptoms and nocturia as those noted by Nakami and associates 11 for open RRP. Indeed, in our hands, it appears that the surgical approach of RALP and specifically the method of intraperitoneal bladder mobilization and bladder neck transection do not offer an advantage over RRP with respect to postoperative nocturia for patients with PCa who are treated surgically. That is, 23% of the patients we classified as N1 (0–1 nocturia episodes per night) at baseline worsened to a N2 or N3 classification 1 year after surgery. This is in contrast to 67% of patients in the N3 group who improved to N1 or N2 1 year after surgery.
Nocturia is not generally cured by removing even highly obstructive prostates. This underscores the notion that local bladder dysfunction represents an important, and perhaps underappreciated, aspect of nocturia in men. As with operative procedures for benign prostatic hyperplasia (BPH), this dysfunction is somewhat recovered after removing the obstruction of the prostate gland, although patients generally do not return to the nighttime voiding habits of their youth. 15,16
Other factors not related to the lower urinary tract (ie, nocturnal polyuria and decreased prevalence of stage 3 and 4 sleep) do not appear to be readily reversible or easily treatable in patients with nocturia as well. That being said, even modest improvements in nocturia can have significant positive impact on the quality of life of patients. 17 This is potentially due in part to the decreased frequency of time these patients generally spend in the restorative stages of sleep. In meta-analysis of urodynamic parameters after various modalities of transurethral resection of the prostate (eg, monopolar and laser), bladder denervation was noted as a possible therapeutic benefit of mechanical resection with respect to relieving irritative symptoms. 16 More recently, investigators focusing on evaluating nocturia-related quality of life after operative treatment of BPH reported that decreased total episodes of nocturia and hours of uninterrupted sleep were associated with improved nocturia-related quality of life. 17
Similar to the overall etiology of nocturia,, the ideal treatment regimen is most likely multifaceted. Multiple agents including the alpha blockers, anticholinergics, and desmopressin agonists have been used in the medical management of nocturia. 5 –8 As of this date, we are unaware of studies examining the use of these agents in patients who have had prostatectomy for PCa and subsequently have either de-novo or ongoing nocturia and urinary bother. Whether the effect of these medications is similar to or entirely different from the effect seen in patients with a native urinary tract would be informative both from a clinical and pathophysiologic perspective.
Worsening nocturia after RALP or prostate removal may be indicactive of overactive bladder (OAB). The International Continence Society defines OAB as urgency, with or without urge incontinence, usually with increased daytime frequency and nocturia and the absence of infection or obvious pathology. 18 The prevalence of OAB in men in the United States is about 16% and markedly increases after the age of 64. 19 OAB-V8 and OAB-9 short forms have been validated linguistically to facilitate data collection crossculturally and the international comparison of symptom bother and health-related quality of life in patients with OAB. 20 One could make the argument that screening for OAB in the prostate cancer population may benefit patients with regard to counseling about the possibility of voiding dysfunction after RALP and its subsequent effect on quality of life.
Weaknesses of our investigation include relatively small sample size, measurements at only two time points, and the limited generalizability of data from tertiary referral centers. Indeed, we are mindful that this report represents the findings from one surgical practice and therefore our observations must be independently confirmed. In addition, we did not have access to functional data from urodynamic studies on these men and therefore report only subjective measures of our outcomes of interest. Similarly, our lack of objective analysis regarding prostate volume, voiding volume, and postvoid residuals with respect to preoperative and postoperative nocturia is a limitation of this study.
With these limitations in mind, our patients demonstrated no overall change in urinary bother through a combined increase in incontinence-type symptoms and decrease in obstructive type symptoms. This is a conclusion that is intuitive and may help inform decision making for patients with PCa in their later years who experience moderate or severe lower urinary tract symptoms including nocturia. Those patients who have excellent urinary function, including a lack of nocturia, should be informed of the possibility of increased urinary bother after surgery; conversely, if patients have significant nocturia related to lower tract obstruction, they have a good chance of seeing their bother improve.
Conclusion
Our data suggest that patients with PCa who have greater frequency of nocturia before RALP are more likely to improve with respect to both nocturia episodes and overall urinary bother. Those with little or no nocturia should be counseled that they may have worsened symptomatology after RALP.
Footnotes
Disclosure Statement
No competing financial interests exist.