
Abstract
Background and Purpose:
Patients with localized prostate cancer (PCa) who are treated by radical prostatectomy (RP) have a good overall survival rate. Their quality of life, however, can deteriorate because of the incidence of bladder neck contracture (BNC). Our aim was to evaluate the incidence and the risk factors of BNC after minimally invasive radical prostatectomy (MIRP) with a single-knot running suture also known as the Van Velthoven technique (VVT).
Patients and Methods:
From 2003 to 2010, 2115 patients underwent extraperitoneal, transperitoneal, or robot-assisted RP for localized PCa. A single-knot running suture according to the VVT was performed for the vesicourethral anastomosis. Follow-up was scheduled and standardized for all patients and recorded into a prospective database. BNC was defined by a reduction of the lumen that does not allow the passage of an 18F fibroscope.
Results:
Mean follow-up of the patients was 43 (6–144) months. Of all
Conclusions:
BNC incidence after MIRP using the single-knot running suture for the vesicourethral anastomosis is low. Previous TURP and external beam radiotherapy are identified as risk factors. This technique showed satisfying results regardless of the classic laparoscopic or robot-assisted approach.
Introduction
A transurethral resection of the prostate (TURP) before the RP, 9 a vesicourethral anastomotic (VUA) fistula, the presence of cardiovascular risks factors, 10 a high body mass index (BMI), 11 a high volume perioperative blood loss, 12 and adjuvant radiotherapy 13 are among the recurrently reported risk factors. While some studies 10 have reported less BNC when a very experienced surgeon performs the RP, others did not show any correlation between the surgeon's experience and the incidence of the BNC. 14,15 Bladder neck preservation is not a factor that can protect a patient against BNC. 16,17
Data from the Cancer of the Prostate Strategic Urologic Research Endeavor cohort showed a higher incidence of BNC after retropubic RP (RRP) compared with other treatment for localized PCa (external beam radiotherapy [EBRT] and brachytherapy) with an incidence varying from 2.7% to 25.7%.
BNC after open RRP has been reported to occur in 6% to 15% of men, yet early reports of laparoscopic RP (LRP) are associated with a BNC rate of 0% to 3%. 18 In a large series of 650 consecutive robot-assisted LRP (RALP), 19 the BNC incidence was 1.1%. Garg and See 20 reported a low incidence of BNC (0.74%, follow-up 48 mos) in their retrospective series of 406 patients using an intussuscepted VUA in RRP. A recent systematic review and cumulative analysis of comparative studies on RRP, LRP, and RALP 21 concluded that most of the available studies showed similar rates of anastomotic strictures in RRP and LRP. The cumulative analysis of all of the available data suggests that strictures were significantly less common in LRP (relative risk [RR]: 2.92; 95% confidence interval [CI] of RR: 1.97–4.34; P<0.00001). Considering only the prospective studies, such differences lack statistical significance (RR: 2.23; 95% CI of RR: 0.93–5.32; P=0.07). Similarly, no statistically significant differences were found between LRP and RALP with regard to anastomotic stricture (RR: 1.42; 95% CI of RR: 0.40–5.06; P=0.59).
A single-knot running suture anastomosis also known as the Van Velthoven technique (VVT) has been reported as a technical modification in LRP to ensure a watertight closure of the VUA to lower BNC rates. 22
The objective of our study was to evaluate the incidence and the risk factors of the BNC after minimally invasive radical prostatectomy (MIRP) with the VVT for the VUA.
Patients and Methods
Patient selection
Between January 2003 and January 2010, 2115 men had a MIRP with the VVT for the VUA. All patients had been staged with digital rectal examination (DRE) and MRI. Bone scintigraphy and abdominal CT were performed when the prostate-specific antigen (PSA) level was >10 ng/mL. Only patients with localized PCa had been operated on. A MIRP includes transperitoneal LRP (TLRP), extraperitoneal LRP (ELRP), and RALP. At our institution, all procedures were performed by three surgeons (CCA, ADLT, LS). The hospital's ethics committee approved the study, and good clinical practice criteria were respected. The primary and the secondary end points were the incidence and the associated risk factors of the BNC using the VVT for the VUA. Treatment options are also reported.
Surgical technique
The different steps of the surgery have been described previously. 23,24 The single-knot running suture was performed as described by Van Velthoven and colleagues 22 regardless of the minimally invasive approach. The main steps of the VUA suture are shown in Figure 1. A synthetic monofilament absorbable suture 3.0 polyglytone (Caprosyn,™ Covidien, Mansfield, MA) was used. Anastomoses with the “Rocco” posterior reconstruction and the V-Loc™ (Covidien, Mansfield, MA) barbed sutures were excluded from this study.
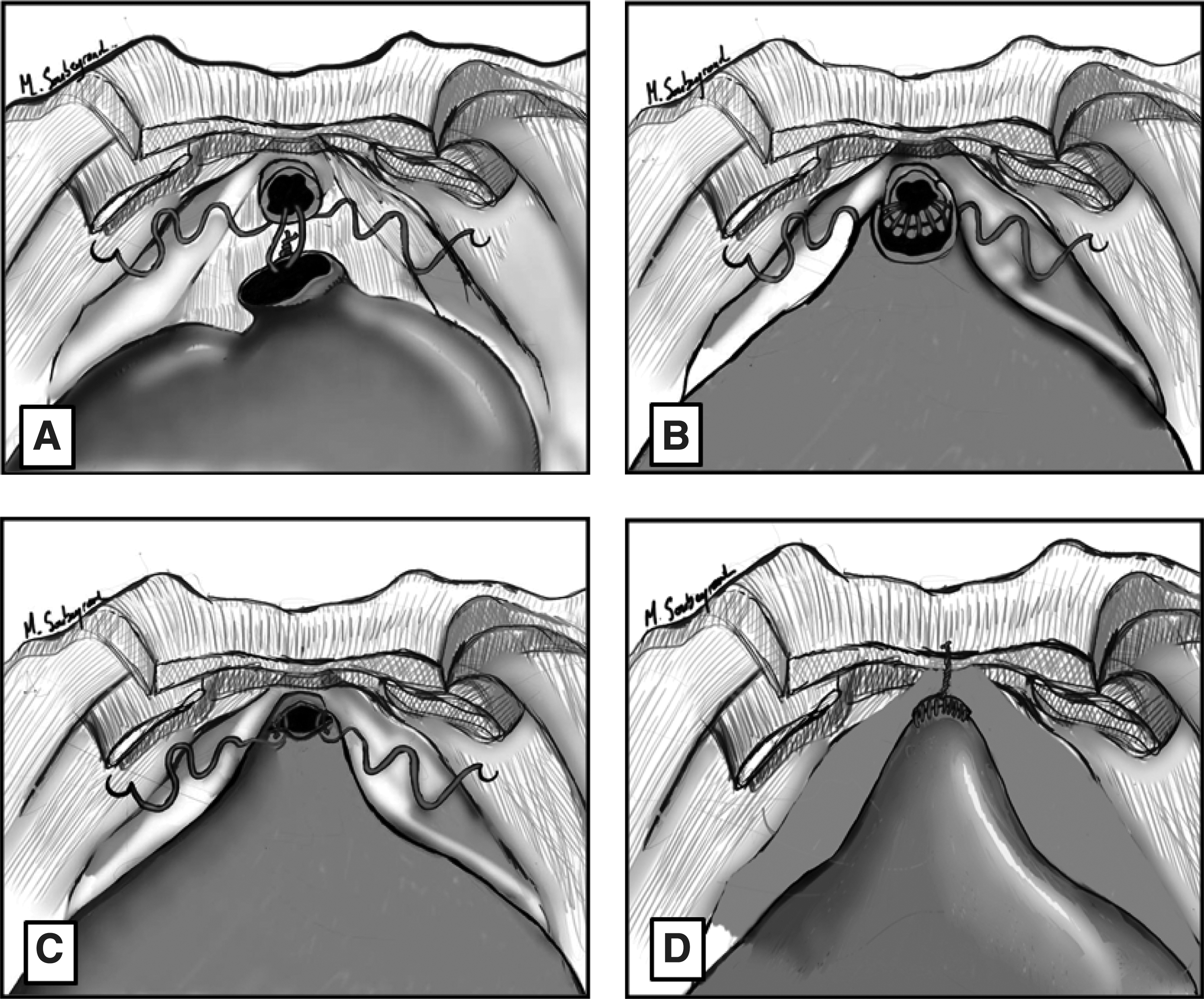
Technique for performing the running single knot anastomosis according to Van Velthoven and colleagues.
22
During the dissection, the bladder neck is divided with cold scissors. The mucosa is everted during the anastomosis. The bladder neck is not systematically reconstructed.
Follow-up
All patients were followed up at our institution, and medical visits were scheduled at 1, 3, and 6 months and then within a 6-month interval after RP. During each appointment, voiding symptoms, uroflowmetry, International Prostate Symptom Score (IPSS), incontinence status, erectile function, pain, PSA level, and DRE were evaluated.
BNC diagnosis
Patients with symptoms (dysuria, urgency) and scores of concern (IPSS and uroflowmetry) for obstruction were examined with urethrocystoscopy. All patients with urethral stenosis other than at the VUA site were excluded. The criteria for a BNC were structured so as to minimize the risk of under- or overdiagnosis.
Database and statistical analysis
Data were collected prospectively into a department database, including preoperative clinical and biologic characteristics and the following patient demographics: Age at diagnosis, preoperative PSA levels, and preoperative procedures (including TURP). Pathologic data were collected on biopsy cores (Gleason score) and on the pathologic prostate specimen (tumor-node-metastasis [TNM] stage, margin status, Gleason score). Perioperative and postoperative parameters including the perioperative blood loss volume, the duration of hospitalization, the BMI, the time of the indwelling catheter, the postoperative anastomotic urine leakage, and the use of adjuvant EBRT were observed and screened as risk factors for the incidence of BNC.
Significant risk factors according to univariate analysis were further analyzed through multivariate analysis using a logistic regression model. A double-sided P value<0.05 was considered as statistically significant. All data were analyzed using SPSS v.16.0 software (SPSS, Chicago, IL).
Results
Of the 2115 selected men, 1342, 241, and 532 patients had ELRP, TLRP, and RALP, respectively. BNC was diagnosed in 30 (1.4%) patients. The median follow-up after RP was 43 months (range: 6–114 mos). Overall, 1453 (69%) patients had more than 1 year follow-up. Patients' characteristics are summarized in Table 1. Among the BNC group, 50% and 78% of the patients received the diagnosis within 6 and 12 months after RP, respectively. The two groups were similar in terms of age at diagnosis, preoperative PSA levels, Gleason score on biopsies and pathology specimen, TNM stage, and margin status. BNC patients, however, had a worse IPSS and a lower uroflowmetry result at the time of the BNC diagnosis.
SD=standard deviation; PSA=prostate-specific antigen; IPSS=International Prostate Symptom Score; Qmax=maximum flow rate; TURP=transurethral resection of the prostate; ELRP=extraperitoneal laparoscopic radical prostatectomy; TLRP=transperitoneal laparoscopic radical prostatectomy; RALP=robotic assisted laparoscopic radical prostatectomy; EBRT=external beam radiotherapy.
The univariate analysis revealed that a hospitalization of more than 8 days (P=0.02), postoperative anastomotic urine leakage (P=0.01), a previous TURP before RP (P=0.04), and EBRT after surgery (P=0.001) were significant risk factors for BNC. Furthermore, patients operated on with a classic laparoscopic approach tended to have BNC develop more than patients operated on with the robot. This finding, however, was not statistically significant. Neither the BMI nor the blood loss during surgery showed any differences between the two groups. Conversely, under multivariate analysis, only a previous TURP to RP (P=0.04) and EBRT after the RP (P=0.007) were still considered as significant risk factors (Table 2).
TURP=transurethral resection of the prostate; EBRT=external beam radiotherapy.
During the follow-up period, the number of surgical procedures per patient was 2.4. The cumulative success rate was 90%. The success rate after one procedure was 47% and rose up to 64% after a second procedure. Eight patients needed more than two procedures to be cured. In three (10 %) patients, the treatment failed. The different treatment options and their respective success rates are shown (Fig. 2). Incontinence status was not impacted by the BNC treatment procedures. In fact, of all patients diagnosed with BNC, 4 (13.3%) and 1(3.3%) reported to wear one or more pads per day before and after the treatment, respectively (P=0.35).
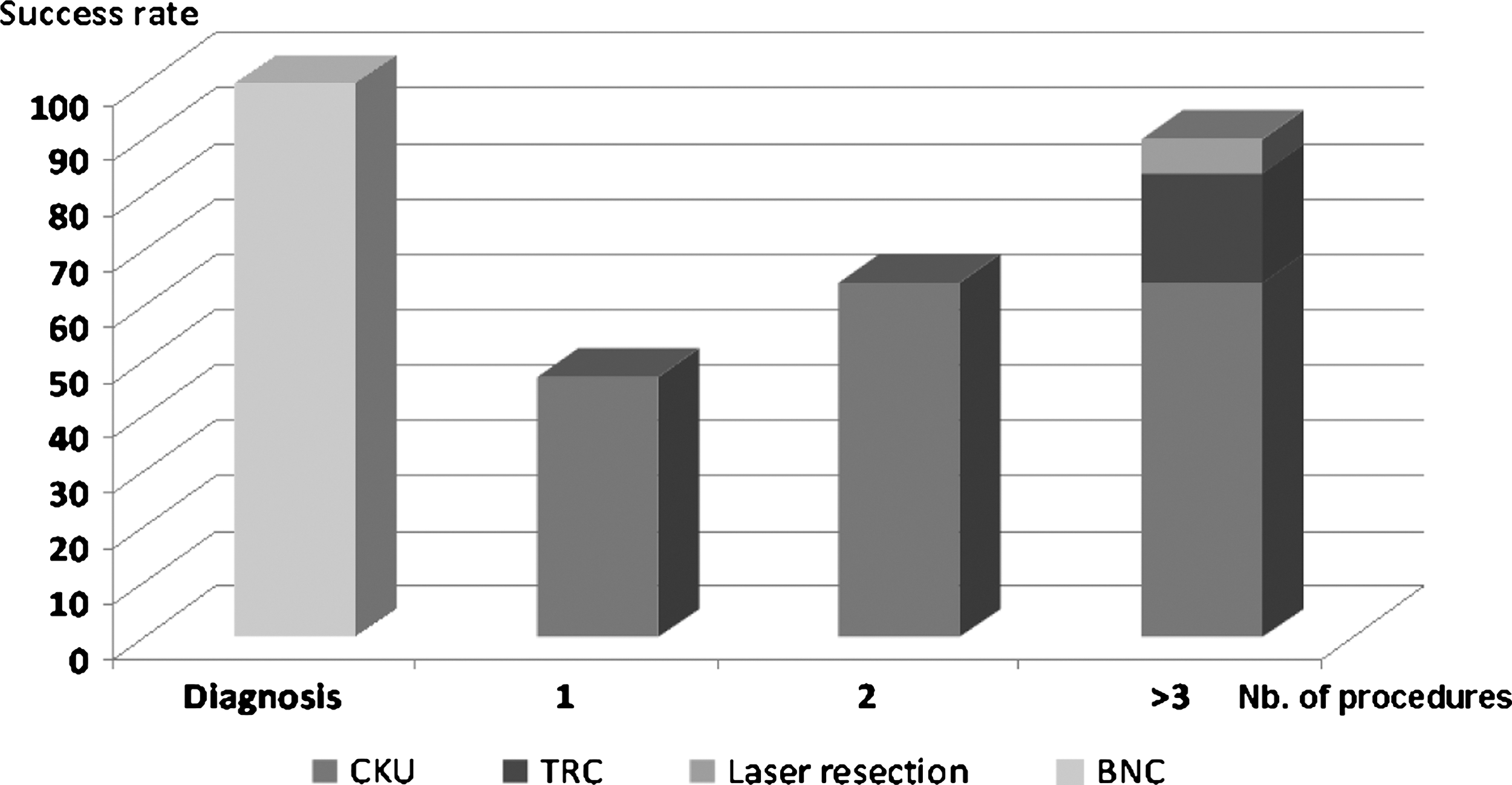
Success rate and treatment options. CKU=cold-knife urethrotomy; TRC=transurethral resection of the contracture; BNC=bladder neck contracture.
Discussion
The VUA is an integral part of the reconstructive portion of RP. 25 BNC is a complication of this reconstruction and is considered a significant reason for morbidity. Apart from the additional operations necessary to correct the condition, BNC puts patients at an increased risk of incontinence. 26 Cited risk factors for BNC after RRP include surgical/anastomotic technique, “excessive” blood loss, urinary extravasations, and history of previous TURP, pelvic EBRT, smoking, and cardiovascular disease. These factors lead to an excessive hypertrophic healing response and scar formation. 12 Another aspect of the surgical technique that plays a role in leakage and BNC is the concept of posterior reconstruction. In the randomized paper by Menon and associates, 27 while no impact on continence was observed with reconstruction, the authors did observe that “a secondary benefit with reconstruction of the periprostatic tissues”. The incidence of cystographic leaks was lower with double layer anastomosis. We consistently had an anastomotic leak rate of 10% to 11% with single layer anastomosis and 3% with double layer anastomosis.
The reported incidence of this complication decreases with surgeons' experience and over time with the improvement of the surgical techniques of RP. 20
Among the published studies concerning the surgical techniques, our study is the first to evaluate specifically the incidence, risk factors, and treatment outcomes after MIRP with a running knot suture of the VUA in a high-volume laparoscopic center. This rate is one of the lowest reported in the literature. Garg and See, 20 using a definition of BNC similar to ours, reported an incidence rate of 0.74% in their retrospective series of 406 patients using the same technique in RRP. This low incidence can be explained by a good urethral realignment, with a watertight closure in a tension-free fashion in this suture. Moreover, all patients have been operated only by experienced surgeons (LS, ADLT, and CCA). Accordingly, Hu and coworkers 14 reported a shorter hospital stay and a lower incidence of BNC after RP in experienced surgeons (>40 RP procedures per year).
Most BNC were diagnosed during the first year after RP. Giannarini and colleagues 28 reported 95% of their BNC 12 months from RRP (median: 3.8 mos) with a follow-up of 69 months (40.5–99 mos). Because most BNCs occur within 2 years of the follow-up, 11 we believe that the incidence values reported here offer an accurate representation of the risk of the BNC being associated with this reconstructive technique.
As reported, previous TURP to RP 3,6,7,29 and EBRT 11 are found to be risk factors for BNC incidence. This incidence may rise up to 33% in the case of patients who are undergoing RP and who have had a TURP. 6 A thin and poorly vascularized bladder neck may result from a TURP procedure that leads to a bad scar forming after the RP procedure. Furthermore, radiotherapy may play a role in scar forming and leads to the same result.
In our study, robot-assisted surgery tended to have less BNC without reaching a significant difference. Data on the current literature did not report a significant difference between the LRP and RALP with respect to the incidence of BNC. In a recent comparative review of RRP, LRP, and RALP), Ficarra and associates 30 reported similar rates of BNC in RRP and LRP in most reviewed studies. Only a single retrospective study reported a lower rate of BNC in LRP compared with RRP. 31
Two issues should be considered when explaining the benefits of the robotic approach. At first, the high resolution and the three-dimensional vision of the robot may offer a more precise anastomotic suture. Second, the robot-assisted procedures have been performed after a long experience of laparoscopic procedures. Thus, these procedures have benefited from our previous experience acquired laparoscopically. In fact, we do not perform LRP anymore, and all RP procedures are now performed using the robotic approach.
A high blood loss volume and a late removal of the catheter were reported to be risk factors for BNC. 12,32 Taken separately, these factors did not reach a statistical significance in our study. A duration of hospitalization after RP of more than 8 days and urine leakage were predictive factors under univariate analysis, however. A longer hospitalization was usually related to postoperative complications: Leakage of the VUA and late removal of the catheter and blood transfusion. When they both occur, these complications may affect the incidence of BNC.
The appropriate management of BNC has been a source of heated debate for years. Even though this was not the objective of our study, examining the results can lead to some key conclusions regarding treatment options. The treatment of BNC is rarely achieved after one procedure. Patients should be informed that BNC treatment may necessitate more than one procedure to achieve a lasting result.
Our study is subject to some limitations. Clinicians pay more attention to symptomatic patients and, thus, these patients are more likely to be examined. In fact, patients are not screened systematically. Urethrocystoscopy was performed only if the patient had voiding dysfunction such as dysuria, a high IPSS, a reduced uroflowmetry. As a result, this may lead to an underestimation of the BNC incidence rate. As long as these patients have a low or no symptomatic BNC, however, this is not an important issue because their quality of life is not affected. Second, treatment options were surgeon-dependent.
We believe this suturing technique is easy and fast with a low incidence of BNC. Therefore, we perform it in all RP procedures. Besides, the use of this technique is becoming more common since the introduction of the barbed sutures without the need to tie knots. 33 Recently, two randomized trials (monofilament vs barbed suture) have been published. 34,35 They both concluded the superiority of the barbed suture with regard to time reduction and cost benefit. The complication rate was similar, however. Both studies did not comment specifically on BNC.
Conclusion
This study showed a low incidence of BNC after MIRP using a VVT for the VUA. A TURP before RP and adjuvant radiotherapy are risks factors. During follow-up, the surgeon must pay attention to any voiding dysfunction that may reveal a BNC. Patients should be informed that the treatment of BNC is time consuming and that multiple procedures are usually necessary to reach a satisfying result.
Footnotes
Disclosure Statement
No competing financial interests exist.