
Abstract
Background and Purpose:
Lower extremity neuropathies from prolonged lithotomy positioning have been well documented. When we initiated our robot-assisted laparoscopic prostatectomy (RALP) program in December 2002, we chose to use the split-leg table that allows patient support in a more anatomic position, hypothesizing that this would reduce risk of neurologic compression injuries. We report our incidence of lower extremity neuropathies associated with RALP using split-leg positioning and review patient and surgical variables associated with this complication.
Patients and Methods:
We retrospectively reviewed records of 377 patients who underwent RALP using a split-leg table. Patient data including height, weight, body mass index, age, and smoking status; surgical variables such as surgeon operative experience and intraoperative times were also assessed. Intraoperative time was defined as anesthesia induction to anesthesia emergence to more accurately measure total time patients spent in the split-leg position.
Results:
Of 377 patients, lower extremity neuropathies developed in 5 (1.3%) in the immediate postoperative period. Of all variables examined, only increased intraoperative time was identified as a potential risk factor for the development of this complication (496.2±34.8 min vs 366.3±96.1 min, P<0.001). Overall mean operative time for all patients was 368.0±96.6 minutes. Three of the five patients had sympoms suggestive of a femoral mononeuropathy.
Conclusions:
Intraoperative time as defined in our study is a significant risk factor for development of postoperative neuropathy. We also found that split-leg positioning appears to put the femoral nerve at risk for injury, instead of the common peroneal nerve as has been previously reported from prolonged lithotomy positioning.
Introduction
Patients are commonly placed in the dorsal lithotomy position for this procedure. 3 Prolonged positioning in lithotomy has been associated with an increased risk for the development of lower extremity neuropathies in the postoperative period. 4,5 A relatively steep learning curve is another reported drawback to performing RALP, with varying reports of up to 250 cases needed before one is considered an “expert.” 6 –8
One assessment of national registries has raised the concern that RALP might offer inferior outcomes at lower volume and nonacademic medical centers. 9,10 Manny and associates 11 recently reviewed the lower extremity neuropathy rates of an experienced robotic surgeon performing RALP and robot-assisted radical cystectomy with the patient in the low lithotomy position and reported a complication rate of 1.7% in a series of 179 consecutive patients. Duration in the dorsal lithotomy position was discussed as a potential contributing factor to this complication. Presumably, at lower-volume centers, less experience with performing these procedures leads to longer durations of the patient in the dorsal lithotomy position—hence, a higher risk for postoperative lower extremity neuropathies.
When we initiated our RALP program in December 2002, we chose to use the split-leg table that allows patient support in a more anatomic position, with the hypothesis that this would reduce the risk of neurologic compression injuries seen with low lithotomy positioning. Early in our series, we noted that for most patients, the table's legs extended approximately an extra 8 cm beyond the patient's feet, necessitating that we hyperextend his hips 20 to 25 degrees to make extra room at the end of the leg support to allow docking of the robot. Since our program's initiation, four surgeons have used this positioning during their initial learning curve. In this study, we investigate the incidence of and the properties of postoperative lower extremity neuropathy after RALP at our institution as well as patient and surgical variables that are associated with an increased risk for this complication.
Patients and Methods
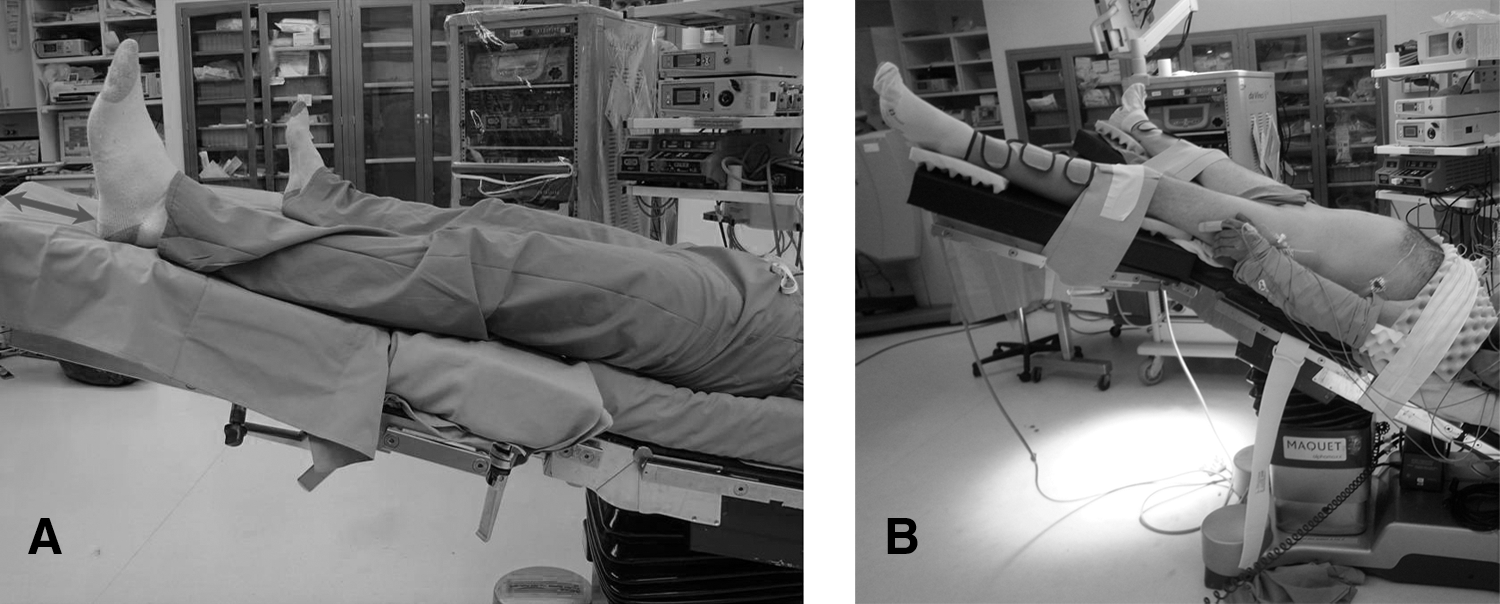
On Institutional Review Board approval, we performed a retrospective review of 377 consecutive RALP performed between December 2002 and March 2011 at the University of Iowa Hospitals and Clinics by one of four surgeons (JAB, CRT, FNJ, and HNW). These 377 patients represent our initial experience with RALP using a split leg table (Fig. 1A). Our method of positioning and contact point padding has been described previously. 12
Data collected from patient charts included age, height, weight, body mass index (BMI), smoking status, surgeon, date of surgery, and intraoperative times. Intraoperative times were defined as time from anesthesia induction to anesthesia emergence to more accurately measure total time patients spent in the split-leg position. Variables in patients who reported postoperative lower extremity neuropathies were compared with those without such neuropathies using the Mann-Whitney U two-tailed t test. P values <0.05 were considered significant. Statistics are reported here as mean±standard deviation or as percentages where appropriate.
Results
Patient demographic data
Patient ages ranged from 38 to 78 years (mean 59.6 years), height from 160 to 195 cm (mean 177.5 cm), weight from 86.3 to 153.5 kg (mean 93.5 kg), BMI from 18.8 to 50.7 (mean 29.6). Opererative times ranged from 183 to 663 minutes (mean 368.0 min). Age, height, weight, and BMI were found not to be significant risk factors for the development of postoperative neuropathies (Table 1).
Mann-Whitney two-tailed test; statistical significance level set at P<0.05, two-tailed test.
BMI=body mass index; ND=not determined.
Postoperative neuropathies
Of the 377 patients included in this series, lower extremity neuropathy developed in 5 (1.3%) during the first 7 days after surgery (Table 2). All five patients were symptomatic within the first 24 hours after surgery, with symptoms including lower extremity weakness, numbness, and paresthesias. Of these five, three experienced weakness and paresthesias in the femoral nerve distribution, and one had symptoms suggestive of an obturator nerve mononeuropathy. The fifth patient complained of transient, cramping pain in his calves. A consultation with physical therapy and orthopedics specialists suggested gastrocnemius muscle tendon shortening and swelling. Symptoms persisted beyond 3 months in three of the five patients affected, with residual symptoms up to 1 year after surgery.
Additionally confirmed by spinal/orthopedic staff.
Additionally confirmed by a neurologist.
Additionally evaluated by orthopedic staff to rule out deep vein thrombosis and compartment syndrome; also evaluated by a physical therapist.
Mean duration in the split-leg position for these patients (496.2±34.8 min) was 34.8% longer than the overall mean for all patients in this series (368.0 min), reaching statistical significance (P<0.05. Durations in split-leg positioning ranged from 440 to 523 minutes for affected patients and 183 to 663 minutes for nonaffected patients. Importantly, three of the five patients with postoperative lower extremity neuropathy were operated on during the surgeon's first 35 RALPs (Table 2).
Discussion
The risk for lower extremity neuropathy during lithotomy positioning is well documented, and surgeons are increasingly aware of this risk. Dorsal lithotomy is the traditional position used for RALP. 3 Lower extremity neuropathies in the immediate postoperative period are a potential complication of this positioning method. Most of these neuropathies result from mild self-limited peripheral nerve injuries, with resolution usually within a few weeks. Prolonged hip flexion, abduction, and external rotation as well as pressure point injuries have been implicated as possible causes for neuropathies in the dorsal lithotomy position. Manny and colleagues 11 reported a 1.7% incidence of postoperative neuropathies in a series of 179 patients who underwent either RALP or robotic-assisted radical cystectomy in the lithotomy position by a single experienced surgeon.
We have used a split-leg table for patient positioning since we started our robotic prostatectomy program in 2002 to allow for more anatomic positioning of the patient intraoperatively, thereby potentially reducing the risk of compressive neuropathies. In our current series, only 5 of the 377 patients had clinically confirmed lower extremity neuropathy, representing approximately 1.3% of our case series. This incidence is similar to the 1.7% complication rate reported by Manny and coworkers. 11
Prolonged duration in the dorsal lithotomy position, especially operative times exceeding 4 hours, has been implicated as the most significant risk factor for the development of lower extremity neuropathies. 4,13 Warner and associates estimated that for each hour in the lithotomy position, the risk for motor neuropathy increases 100-fold. 4 In our series, intraoperative times for all five patients in whom lower extremity neuropathies developed were significantly higher than the overall average operative time for all patients in this study (496.2±31.1 min vs 377.9 min, respectively, P<0.001), implicating duration of split-leg positioning to be a significant risk factor for the development of this complication.
Of significance, our overall mean operative time for RALP (368.0 min) was longer than has been typically reported in the literature (141–540 min), 14 because we recorded the time from general anesthesia induction to anesthesia emergence. The more commonly used definition of operative time is from skin incision to skin closure; however, we believe our measurement better reflects the actual time the patient was positioned on the operating table.
BMI ≤20, recent tobacco use, and a history of neuropathy have been implicated as further risk factors for development of lower extremity neuropathy. 4,5,15 We did not note significant correlation between BMI and the risk for development of postoperative neuropathies. Low-BMI patients, however, were underrepresented in our study, as reflected by the average BMI of 29.6. An intriguing hypothesis that comes out of this observation and consistent with Warner and colleagues 4 is that the extra subcutaneous fat padding in higher-BMI patients is somewhat protective against pressure-related nerve injuries. Because the observed neuropathies in this series were likely not from direct pressure, this may be less germane.
We also analyzed tobacco use as a potential risk factor for postoperative neuropathies. Our case series of 377 patients included 103 (27.3%) current or former tobacco users. Of these, postoperative neuropathies developed in only two (1.9%), significantly lower than the 71% seen by Warner and coworkers. 4
Our study also reveals that the split-leg table potentially puts different nerves at risk for injury compared with those reported for lithotomy positioning (Table 2). Warner and colleagues 4 retrospective review of 198,461 consecutive patients who underwent various surgeries in the lithotomy position showed that motor neuropathies commonly involved the common peroneal (78%), sciatic (15%), and femoral (7.3%) nerves. We found that the split-leg approach appears to place the femoral nerve at risk for intraoperative injury. The characteristics and distribution of the neuropathies seen in three of our five patients are consistent with femoral mononeuropathy.
Evaluation of the respective patient complaints was not standardized, a caveat that was a consequence of the retrospective nature of this study. Subsequent prospective studies will standardize this evaluation. We postulate that the hip hyperextension that was necessary to allow effective docking of the robot can lead to femoral nerve compression as it courses beneath the inguinal ligament, 16 thus affecting the motor and sensory branches downstream of the ligament. The paradigm for most femoral neuropathies is that they tend to resolve spontaneously, although permanent damage remains in a small number of patients, leading to significant disability. 17 In our study, most of the patients (three of five) had residual neuropathies beyond 3 months from surgery. Obturator mononeuropathy is also a possible complication of pelvic lympadenectomy. One hundred five (27%) of the patients in this series underwent concomitant pelvic lymph node dissection. Of note, only one of these patients experienced postoperative neuropathy, but in the femoral nerve and not the obturator nerve distribution.
The leg supports on the split-leg table used in this study extended about 8 cm beyond the patients' feet. With this extra length, we often encountered difficulties docking the robot without hyperextending the hips, because the robotic arms would bump into these extensions, making docking impossible. As a result and as stated previously, we had to extend the patients' hips 20 to 25 degrees to create more room for the robot to be docked. We routinely attempted to raise the legs back up after docking the robot to minimize hip hyperextension, but we frequently were not able to raise them all the way back up to neutral position. This hip extension potentially increases the risk for nerve compression at the hip. Lastly and importantly, we recently switched to a shorter version of leg supports (Fig. 1B) that allows effective docking of the robot between the patient's abducted legs without the need for hip extension as needed for the leg supports used in this study. We are currently evaluating this new method.
Most of the complications (three of five) occurred during the first 35 cases performed by these surgeons, and none occured during the last 35 cases. The number of cases beyond which a surgeon is considered to have passed his/her initial learning curve for RALP has varied widely in the literature, from 20 to 250 cases. 6 –8 Undoubtedly, the existence of a learning curve is likely to compromise the outcomes of the initial cases performed by the surgeon, and this may include position-related complications. As surgeons gain more experience and move further along their respective learning curves, they should be able to perform these surgeries more quickly, potentially reducing the risk of such complications.
Conclusions
Complication rates with split-leg positioning are comparable to those previously reported for lithotomy positioning when performing RALP. The duration of time in the split-leg position was the only factor we identified as a potential risk for development of lower extremity neuropathy. Split-leg positioning also seems to put the femoral nerve at most risk, likely from hip hyperextension, compared with common peroneal neuropathies associated with extended lithotomy positioning. Use of shorter leg supports may facilitate da Vinci robot docking in the split-leg position, eliminate or reduce the need for hip hyperextension, and prevent or reduce these complications. Also noteworthy is that most of these complications occurred during the earlier portions of the surgeon's learning curve, suggesting that with experience, the incidence of these complications might be lower.
Footnotes
Disclosure Statement
No competing financial interests exist.