
Abstract
Background and Purpose:
The surgical approach and repair for urorectal fistula (URF) is a challenging task. A variety of techniques have been described to treat URFs, and the laparoscopic approach has been approved as an efficient tool for even some complex fistulas. We aimed to report our laparoscopic experience for complex URF repair with special emphasis on salvage prostatectomy.
Patients and Methods:
The study included four men (59–75 years), with laparoscopic repair for complex URFs. URF developed after transurethral resection of the prostate in patients 2 and 3 and after radical prostatectomy in patient 4. Patient 1 had received combined radiotherapy and chemotherapy for the rectal carcinoma; a prostatic abscess developed that resulted at the end in URF. Laparoscopic salvage prostatectomy was performed for patients 1 and 2. A transvesical laparoscopic approach was performed for patient 3, and a transperitoneal transvesical technique was performed for patient 4. A tunica vaginalis flap was used for patient 1, and peritoneal interposition flaps were developed in patients 2 and 4 mL, and no patients needed intraoperative blood transfusion. Postoperative hospital stay was 12 to 34 days. The urethral catheter was removed on postoperative day 11 to 32, and cystography showed no leakage of contrast except in patient 1.
Conclusions:
Laparoscopic URF repair is safe and efficacious in experienced hands even in complex cases, and salvage laparoscopic prostatectomy seems like a valuable operative option. The technique requires advanced experience, however, particularly with pelvic surgery and intracorporeal suturing.
Introduction
A patient with URF usually presents with urine leaking from the rectum. The first treatment option is conservative and includes urinary and/or fecal diversion. This approach is rarely successful, however. 6,7 A variety of techniques have been described to treat URFs, including transanal, transanorectal, transsphincteric, transabdominal, perineal, and combined approaches that are frequently used. 2,3,5,8 –10
The laparoscopic approach has been approved as an efficient tool for even some complex URF. 11 –14 Recently, the da-Vinci robot system has been applied successfully for the management of an URF as an alternative therapy option. 14
We aimed to describe different laparoscopic approaches including our salvage prostatectomy technique for URF repair on four patients and discuss the outcomes. A review of the literature with particular emphasis on the minimal invasive approaches is also included and discussed.
Patients and Methods
Patients
One year after radiotherapy, urinary leakage through the anus developed without abdominal pain. Cystourethrography (CUG) revealed a URF and a right vesicoureteral reflux grade II. Rectal examination showed normal findings. Urinary analysis showed increased white blood cells with nitrite positivity. Conservative treatment with a urethral catheter for 8 weeks was initiated and failed; a decision for surgical treatment was taken.
We performed retroperitoneal laparoscopic fistula repair for patient 1, transperitoneal laparoscopic repair for patients 2 and 4, and transvesical laparoscopic repair for patient 3.
Surgical technique
All operations were performed by the same surgeon (JR). Patient characteristics and surgical outcomes are summarized in Table 1. Under general anesthesia, patients were placed in a low lithotomy and Trendelenberg position head downward, with compression stockings applied to the legs. An 18F silicone urethral bladder catheter was placed.
BMI=body mass index; TURP=transurethral resection of the prostate.
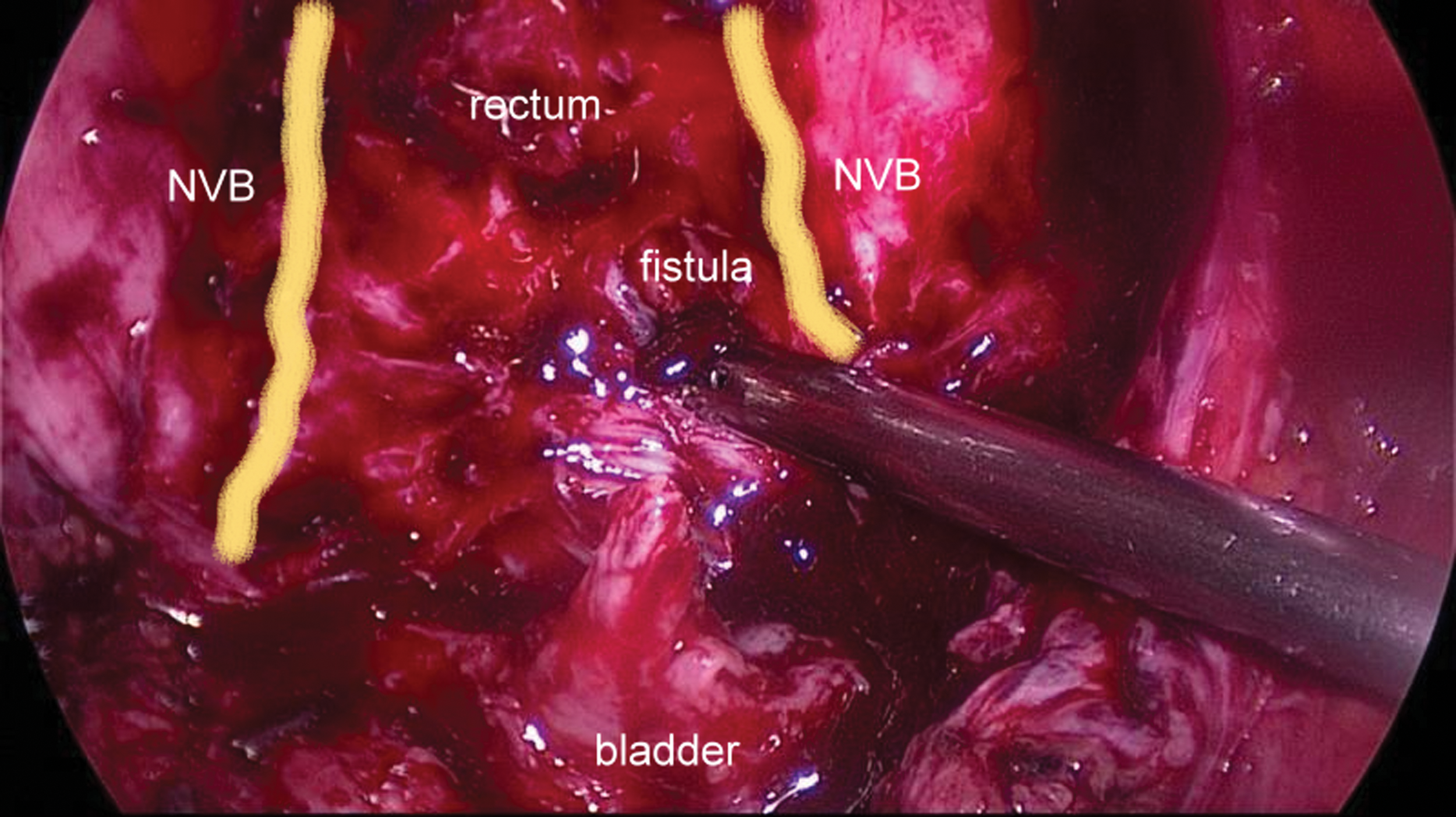
Demonstration of the fistula tract, rectum, neurovascular bundles (NVB), and urinary bladder.
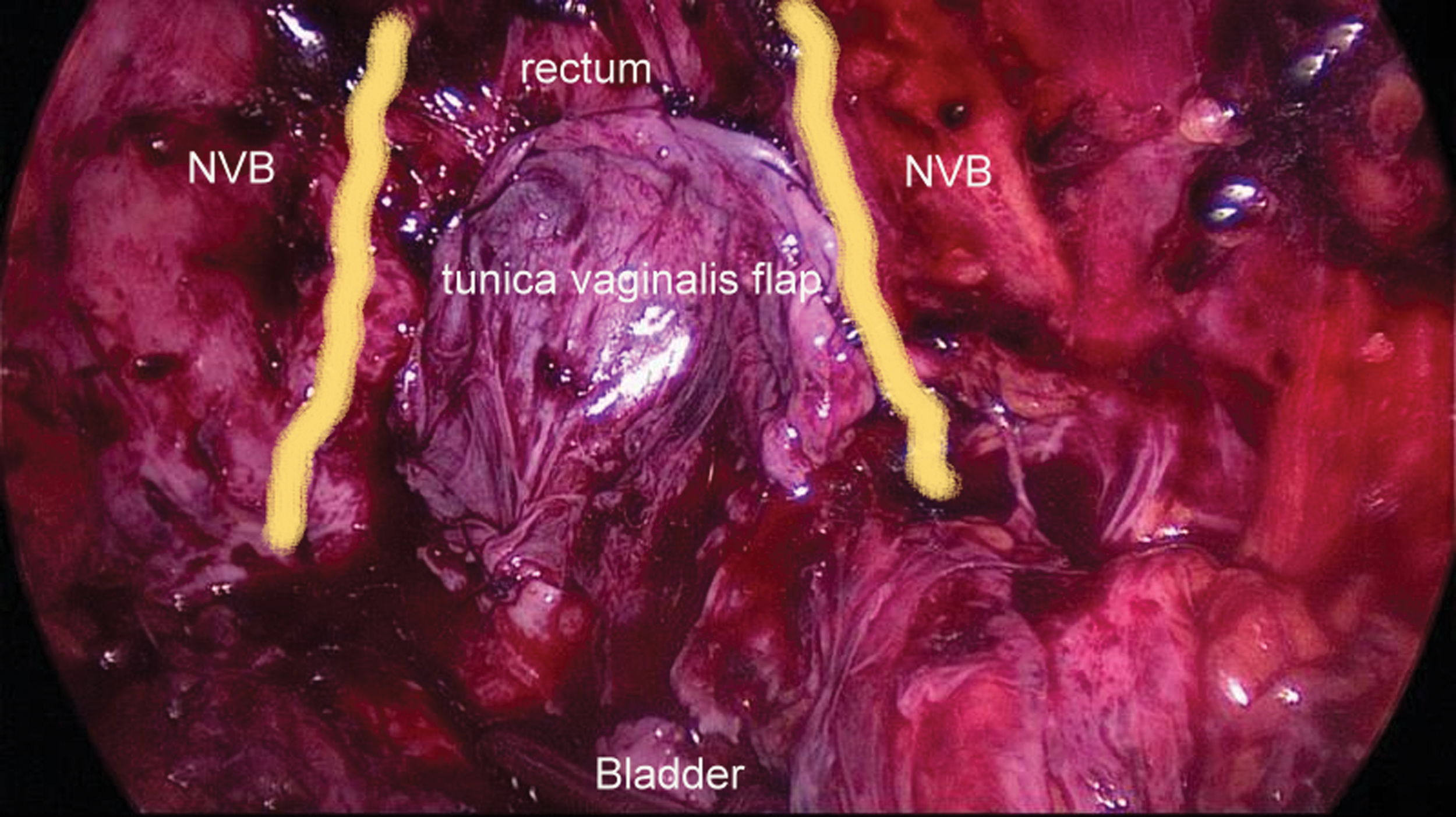
Interposing tunica vaginalis flap for the interposition is placed and fixed on the fistula suture line and sutured with 3/0 polyglactin stitches. NVB=neurovascular bundles.
Results
Patient characteristics, history, surgical and postoperative outcomes are summarized in Table 1. The range of operative time was 114 to 283 minutes. The range of intraoperative blood loss was 50 to 600 mL. No patients needed intraoperative blood transfusion. Postoperative hospital stay was 12 to 34 days. The urethral catheter was removed on postoperative day 11 to 32.
All patients were discharged from the hospital in good condition. Follow-up CUGs showed no leakage of contrast in all patients.
Postoperative interventions and follow-up
The urethral catheter were removed on postoperative day 12 for patient 1 and day 16 for patient 2 because of his postoperative sepsis and the CUG performed that showed no leakage of contrast. Nonetheless, a recurrent fistula developed in patient 1 at 9 months after the surgery, and he still has a urethral catheter.
Discussion
URFs are a rare but devastating complication that can usually develop after TURP or radical prostatectomy. 1 –3 The URFs were differentiated to two groups by Munoz and associates. 17 One is benign and it is infectious and traumatic; the other is a malignancy-related complex fistula, such as neoplastic, surgical, and radiogenic. For these kinds of fistulas, the situation is even more complicated and accordingly the success rate is low. All of the cases in our series were complicated fistulas, occurring after chemotherapy or radiotherapy or combination therapy for different malignancies.
Conservative approaches, consisting of urinary diversion, wide spectrum antibiotics, and parenteral hyperalimentation, may allow cure in certain iatrogenic fistulas. Success rates as high as 25% to 53% have been reported in the literature. 8,18 Most of them (ie, complex fistulas), however, necessitated surgical interventions, especially if the fistula remained in for 3 to 6 months. 19,20 Another conservative approach option is bowel rest via fecal diversion and described by some authors as mandatory. Others, however, advocated that it is necessary only when there are previous failed repairs, complex fistulae, and a history of radiotherapy or pelvic sepsis or in the absence of bowel preparation. 21 All of our patients had urinary diversion. In addition, our two complex cases (patients 1 and 4) had fecal diversion (colostomies) (Table 1). Conservative therapy failed in all our cases, however, and we decided on minimally invasive surgical therapy.
Successful treatment of an URF is often challenging. Several procedures have been described, which include different approaches and different flap types and techniques. 9,10,19,22,23 There has been no consensus, however, on the best method of repair. 19
Basic surgical principles include excision and debridement of the fistula tract to healthy vascular tissue, and separation of the rectal and bladder suture lines with tissue interposition. 24 Especially for fistulas in irradiated fields with ischemic fibrosis and radiation changes around the fistula, the procedure is technically difficult and the probability of successful closure is low. 13 Munoz and colleagues 17 reported on 23 patients with complex fistulas using different surgical approaches, and their success rate was only 25% (6 patients) at the first operation.
Laparoscopy in urology has become popular in recent years. It is increasingly performed in many institutions worldwide, and the number of experienced surgeons with improved laparoscopic skills particularly dealing with complex urologic procedures has increased (Table 2). Laparoscopy provides the opportunity of magnification, thus better exposure, of the tissue layers, where many anatomic structures are located close to each other in a limited pelvic space, as in pelvic surgeries. This facilitates better exposure of the rectum and better preparation of the anterior rectal wall and more delicate dissection and removal of the fistula tract.
Two months postoperatively, the suprapubic tube was removed.
Robotic repair.
The range of the value.
Fistula recurrence in patient 1 detected on follow-up.
Pt=patent; Preop=preoperative; cons=conservative; Tx=treatment; op: operative; FU=follow up; recur=recurrence; RP=radical prostatectomy; NR=not reported; TURP=transurethral resection of the prostate; KP=chronic prostatitis; PA=prostatic abscess; AR=apical resection; RT=radiation therapy.
Currently, the published literature regarding laparoscopic URF repair is still rare and consists mostly of case reports. 11 –14 Our results in terms of mean operative time, blood loss, hospital stay, and catheter removal time were similar when compared with other cases (Table 2). In our opinion, the complexity of the fistula plays an important role in the success of the procedure as much as the preferred operative technique. We reached a success rate of 75% (three of four cases), which may be considered successful in our complex fistula group with additional comorbidities.
The open salvage prostatectomy was reported before in the literature, especially for postirradiation URFs. Mundy, Andrich and coworkers 25 have advocated that good exposure of the rectal defect after a salvage radical prostatectomy for closure and interposition of an omental flap before the vesicourethral anastomosis was advantageous. They found, however, that the salvage radical prostatectomy was not easy to perform in this group of patients with complex fistulas.
We have performed a salvage laparoscopic prostatectomy for URF in patients 1 and 2. Laparoscopic radical prostatectomy has become an accepted alternative to open surgery worldwide with distinct advantages such as the reduction of postoperative pain, complication rate, hospital stay, and convalescence related to the less invasive approach. 26,27 The laparoscopic approach to URF requires advanced laparoscopic experience, particularly with pelvic surgery and intracorporeal suturing. The type of surgery that will be performed depends mostly on the training and experience of the surgeon. For these reasons, this operation is not proposed for surgeons in the early learning curve. To date, we have treated more than 2500 patients successfully using the Heilbronn techniqu 28 with both laparoscopic and robot-assisted approaches in our institution.
The role and value of salvage prostatectomy in these complex and difficult cases is still to be determined. It seems beneficial, however, if an established laparoscopic technique is combined with experience. Another important point to underline is the advantage of the Heilbronn technique, because the posterior dissection is performed on the rectum at an early step of the operation; this allows good exposure of the rectum and better dissection of the anterior rectal wall and the fistula tract. Furthermore, we think that the robotic approach would also facilitate the salvage prostatectomy procedure with the well-known advantages—especially the high quality, three-dimensional vision and six degrees of freedom in the deep pelvis might increase the surgical outcomes. Therefore, we intend to perform the next URF procedures in our institution with robot assistance.
Nonetheless, a recurrent fisula developed in one of the patients (patient 1) at 9 months after the surgery. He had received combined radiotherapy and chemotherapy for the rectal carcinoma; thereafter, a prostatic abscess developed that resulted in URF. An interposition flap is obligatory in similar complex cases. We have preferred a large tunica vaginalis flap in this case (Fig. 2) because of the low tissue quality of omentum and peritoneum. Jordan and colleaues 29 have reported better results using muscular flaps, such as gracilis or rectus abdominis, in similar complex cases. Besides all the advantages of the minimally invasive technique, developing these bulky flaps seems still technically challenging for minimally invasive approaches.
As observed in previous studies, laparoscopic radical prostatectomy is technically more challenging in obese patients and may contribute to increased operative times, blood loss, and positive surgical margins. 30 –32 This might be another negative factor in our patient 1 with a high body mass index (36.8 kg/m2).
The transvesical approach and intravesical laparoscopic suturing have already been described by Gill and associates. 33 Recently, many investigators have presented their experience with laparoscopic transvesical operations for fistulas using the intracorporeal suturing technique. 34 –36 We have reported our experience and technique for transvesical laparoscopic urethrorectal fistula repair 11 The laparoscopic extraperitoneal and/or transvesical approach offers several advantages, including excellent exposure; avoidance of bowel manipulation, such as occurs in the transabdominal approach, or cutting through the muscles, such as in the perineal approach; decreased operative time and postoperative morbidity, and, finally, earlier convalescence. This approach, however, is suited only for the fistulas close to the bladder neck. We preferred in our patient 4 a similar transperitoneal approach that has allowed us additionally to develop a peritoneal interposition flap.
Conclusions
Laparoscopic URF repair seems to be a safe, feasible, efficacious alternative to the open abdominal approach, and salvage laparoscopic prostatectomy seems like a valuable operative option with the well-known advantages of laparoscopy. Although it is not possible to draw a strict conclusion with the limited number of patients in our series, we recommend this minimally invasive surgery in the management of URF, particularly by experienced laparoscopic surgeons in high volume centers. We think that the robotic approach would facilitate the salvage prostatectomy procedure with the well-known advantages. Further randomized studies are warranted to compare the outcomes of laparoscopy vs open URF repair.
Footnotes
Disclosure Statement
No competing financial interests exist.