
Abstract

A 41-year-old woman underwent percutaneous nephrolithotomy (PCNL) at a local hospital because of a right renal calculus. The Double-J stent was placed in the right ureter during surgery. She was discharged uneventfully 7 days after that procedure. Six weeks later, as scheduled, the patient was in clinic to have the Double-J stent removed through cystoscopy. Unfortunately, the lower end of the ureteral stent could not be visualized during this cystoscopy.
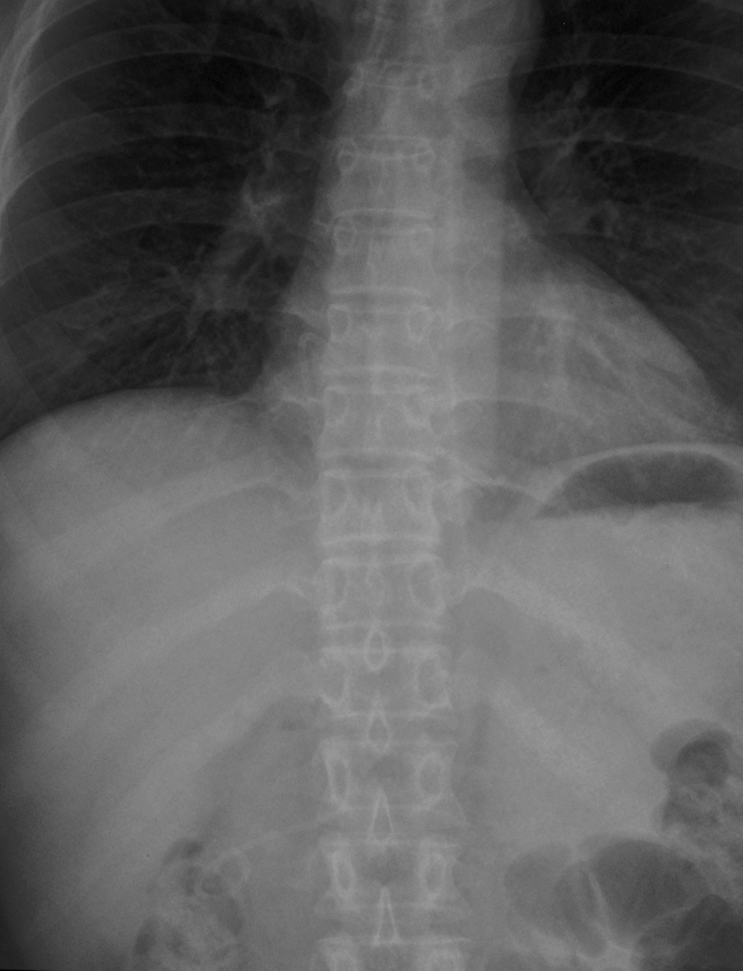
Radiography of the kidneys, ureters, and bladder showed that the Double-J stent was not within ureter, only with its distal portion in the right renal pelvis and the residual catheter along the course of the inferior vena cava (Fig. 1). Her laboratory examination was unremarkable except urinalysis (occult blood +++, white blood cell +++). Although the patient did not have any symptom or sign, she was transferred to our hospital 2 days later to prevent further serious complication.

Skiagram of the kidneys, ureters, and bladder at presentation.
At our hospital, radiography (Fig. 2) and CT (Fig. 3) confirmed this unusual migration of the Double-J stent. Different from the the authors' case, the stent was not entirely in the vessels, and its lower end was located in right renal pelvis. The patient presented with no hematuria or bleeding that might be attributable to intracatheter blood clotting. When the stent was removed, however, the importance of pressure gradient between the right renal pelvis and inferior vena cava should not be dismissed.
Radiography revealed the migration of the Double-J stent into the inferior vena cava.
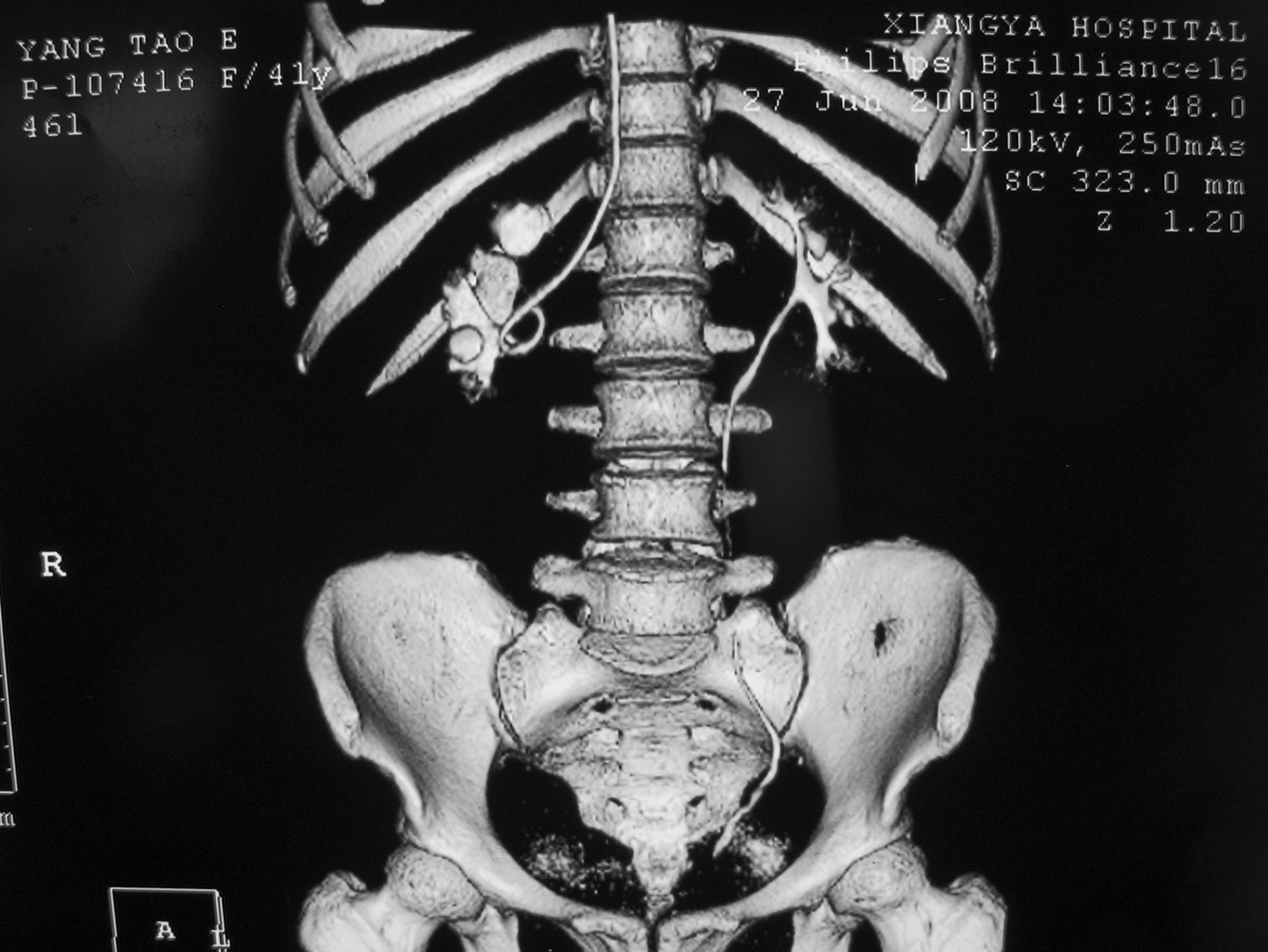
Three-dimensional reconstruction of computed tomography.
Normal intrapelvic pressure is less than 15 cm H2O, and it could be greater (even more than 22 cm H2O) when obstruction is present. 1 Generally, central venous pressure (CVP) was about 5 to 12 cm H2O. CT also showed that the patient had mild hydronephrosis, so her intrapelvic pressure should be greater than or nearly equal to CVP. That meant hematuria or hemorrhea was less likely to present, but the risk of infection was increased when the stent was removed. Hence, antibiotic prophylaxis should be essential during treatment.
To our knowledge, there are three ways to remove endovascular foreign bodies: Open surgery, transurethral, and intravascular retrieval. We agree with the authors that percutaneous intravascular extraction would be less invasive than the former ones. Finally, the stent was successfully retrieved under angiography, and the patient was discharged 3 days later. She had an uneventful 3-year follow-up visit recently.
Migration of a Double-J stent into the inferior vena cava is a rare and severe complication of PCNL even if the patient presented in a well condition. A long-indwelling stent may result in inflammation, hemorrhage, thrombopoiesis, and even fragmentation. 2 Intravascular extraction is an effective, feasible, and safe method to remove an endovascular Double-J stent.
Footnotes
Acknowledgment
We thank Jay Mei, M.D., Ph.D., for editorial assistance with our manuscript.