
Abstract
The midurethral sling has emerged as an effective, minimally invasive treatment for patients with stress urinary incontinence. Bladder penetration is a known complication that, if unrecognized, may result in retained intravesical mesh. This rare complication can cause patient discomfort as well as become a nidus for infection and bladder calculi. Because of the technique of sling passage, the site of retained sling material is often along the anterior bladder wall, making evaluation and treatment via traditional retrograde cystoscopy prohibitively difficult. We describe a novel and minimally invasive method to remove the sling material using antegrade access into the bladder in conjunction with holmium laser vaporization. In our series of six patients in whom retrograde cystoscopic treatment had failed, all were successfully treated with antegrade cystoscopy and reported improved urinary symptoms. This new technique provides a simple, minimally invasive, and effective method for removal of exposed sling mesh.
Introduction
Removal of intravesical foreign bodies is typically performed with retrograde cystoscopy. Likely locations for bladder penetration during midurethral sling placement are the 11 and 1 o'clock positions along the anterior bladder wall. This location can make retrograde cystoscopic treatment prohibitively difficult. Often, a 70-degree lens is needed to visualize the injury, but a 0- or 30-degree lens is needed to use endoscopic instruments. To this end, we developed an antegrade approach to visualize and manage exposed sling mesh.
Technique
Adequate general sedation is administered. The patient is placed in the dorsal lithotomy position with a moderate Trendelenberg position. Retrograde cystoscopy using a 30 degree lens ensures proper cystostomy placement. An 18-gauge spinal needle is placed percutaneously 3 cm superior to the symphysis pubis. Placement should be in the midline near the dome of the bladder, being mindful that a vesicular puncture near the exposed mesh will result in difficulty accessing the desired site. Once placed, an Amplatz super stiff 0.035-inch guidewire is placed through the needle, while visualizing the wire cystoscopically. The abdominal fascia is incised in a cruciform pattern using a fascial incising needle (Cook Medical) over the guidewire. Amplatz renal dilators are used to dilate the tract to accommodate a 24F sheath.
Once the bladder is accessed, the cystoscope with a 30-degree lens is used to inspect the bladder, identifying both ureteral orifices and the site of eroded mesh (Fig. 1). Visualizing the anterior bladder wall involves rotating the cystoscope 180 degrees. A urethral catheter can be placed, depending on the need for continuous irrigation during the procedure. Encrustations on the mesh are removed using holmium:yttrium-aluminum-garnet (Ho:YAG) laser lithotripsy with a 1000 micron fiber, 0.6 to 0.8 joules of energy, and a pulse rate of 6 to 8 Hz. Once the mesh is exposed, endoscopic scissors are used to cut out the majority of visible mesh (Fig. 2). The Ho:YAG laser is again used to treat any remaining mesh using the aforementioned settings and ensuring good contact between laser fiber and mesh. Bugbee electrocautery at 60 W is used over the erosion site to allow for reepithelialization. The antegrade access sheath is then removed and the insertion site dressed. The urethral catheter is removed, if placed. The patient is then discharged home the same day, with oral antibiotics, anticholinergics, and analgesics.
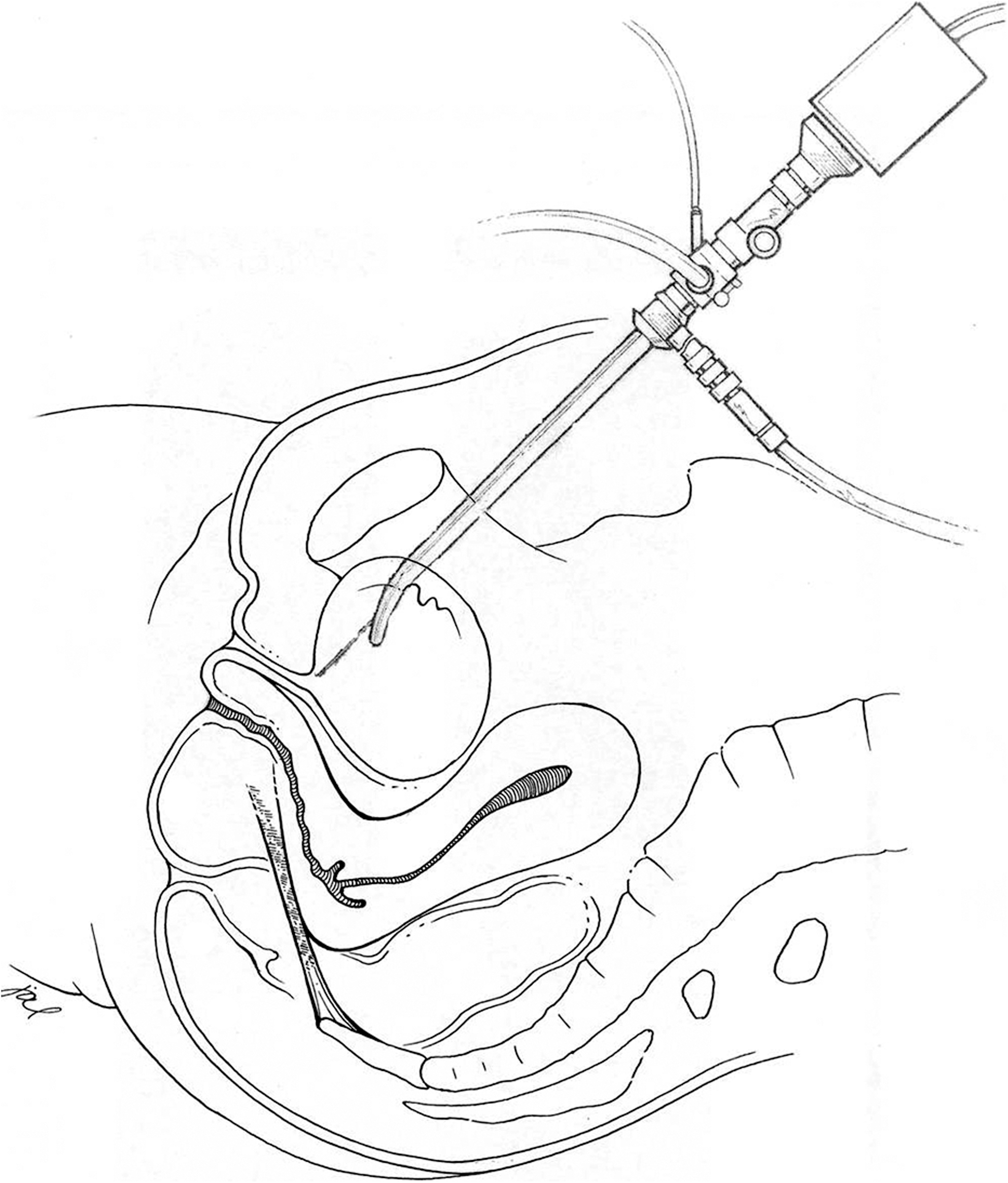
Schematic of antegrade cystoscopy.
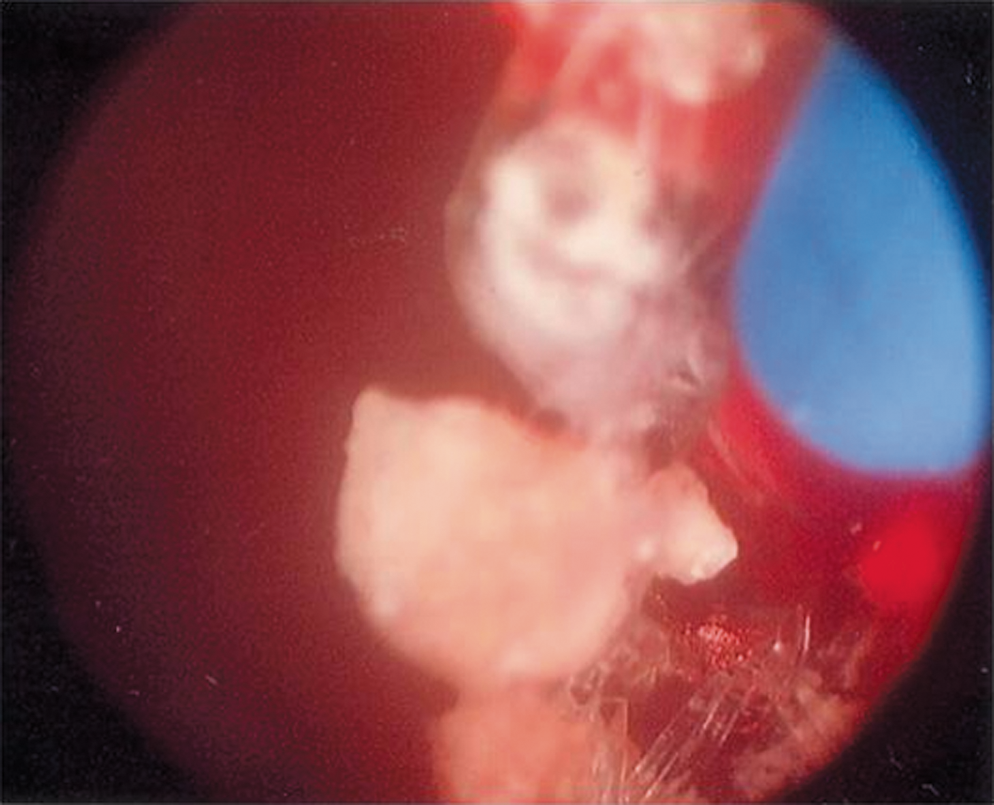
Intraoperative mesh removal.
Equipment
Obtaining antegrade access
• 23F rigid cystoscope
• 0.035″ Amplatz super stiff guidewire
• Amplatz renal dilators
• Fascial incising needle
• 16F Foley urethral catheter
Excising exposed mesh
• Holmium:YAG laser with 1000 micron fiber
• Endoscopic scissors
• Endoscopic graspers
• Bugbee electrocautery
Role in Endourology
We identified six women from 2009 to 2011 with exposed intravesical midurethral sling mesh. The mean age of the patients was 53.7 years (range 38.0–66.7 y). All presented with pelvic pain and had been treated unsuccessfully using retrograde cystoscopy. Office cystoscopy verified the presence of mesh, which was located in the 11 and 1 o'clock positions along the anterior bladder wall. Using the antegrade approach, four of six (67%) patients were able to have complete removal of all mesh in one procedure, confirmed by flexible cystoscopy on postoperative visit. Two (33%) patients needed a second antegrade procedure. No patients needed more than two procedures. There were no intraoperative or postoperative complications.
Mean follow-up was 8.0 months (range 1.3–22.9 mos). Three of six (50%) patients stated that their urination was “better” compared with before surgery, while the other three of six (50%) patients stated they were “much better” after the procedure. Five of six (83%) paients reported that pain and lower urinary tract symptoms (LUTS) resolved. One of six (17%) patients reported that pain resolved but LUTS were unchanged.
Discussion
Synthetic mesh slings are widely used for stress urinary incontinence. Rates of exposed mesh range from 0% to 2% using these techniques and can be attributed to surgical approach and surgeon experience. 7 –9 Unfortunately, when unrecognized injury occurs, exposed intravesical sling mesh can cause bladder calculi and significant urinary symptoms.
Multiple endoscopic approaches have been reported. Compared with open intra-abdominal or transvaginal techniques, endoscopic approaches offer decreased blood loss, infection risk, and postoperative pain. Endoscopic approaches commonly use retrograde cystoscopic removal of the intravesical mesh and adherent calculi. 10,11 Because of the mesh location, however, the affected area is often poorly visualized and subsequently inadequately treated. Alternate methods have been described using suprapubically placed laparoscopic instruments. 12 –15 Pure laparoscopic techniques necessitate multiple trocars penetrating the bladder. Combined laparoscopic/cystoscopic approaches use retrograde cystoscopy, which still provides suboptimal visualization. Both of these approaches do not take advantage of the full armamentarium of cystoscopic tools.
The antegrade cystoscopic approach we describe has advantages over the classic retrograde and laparoscopy-assisted approaches. The technique has been described and successfully applied to procedures at the bladder neck. 16 The instrumentation is well known and does not necessitate familiarity with laparoscopic techniques. The angle of the cystoscope allows for direct and straightforward visualization of the eroded mesh along the anterior bladder wall. Accidental ureteral orifice injury is minimized, because these can be seen easily through a suprapubic approach. Finally, continuous bladder irrigation through a urethral catheter maintains visualization that is unimpaired by intraoperative bleeding.
Despite its advantages, the antegrade approach has theoretical drawbacks. Placement of a suprapubic access tract carries risk for bowel injury. This is minimized by cystoscopic visualization during placement, but this approach should be cautioned in patients with previous abdominal surgeries or small capacity bladders. In this situation, suprapubic cystostomy via ultrasonographic guidance or Lowsley retractor should be considered. 17 Patients with bleeding disorders or who need therapeutic anticoagulation are likewise suboptimal candidates for suprapubic cystostomy.
Conclusion
Patients with exposed intravesical mesh at or near the bladder neck should be strongly considered for antegrade cystoscopic removal. The procedure is well tolerated and safe. Further studies with larger patient populations and longer follow-up are needed to further investigate and develop this novel and effective procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.