
Abstract
Purpose:
To examine the efficacy of an alpha-1 blocker and its correlation to structural alteration of the prostatic urethra and the loss of energy in the urine flow using a virtual urethra processed from an endoscopic video image.
Materials and Methods:
Video images of the prostatic urethra were recorded during cystourethroscopy in 11 patients with benign prostatic hyperplasia (BPH) before and after treatment with an alpha-1 blocker, naftopidil. The three-dimensional (3D) structure of the prostatic urethra was reproduced from video files. Fluid dynamic analysis and hydraulic energy calculations were performed using the “virtual” 3D urethral images.
Results:
In 9 of 11 patients studied, an 11% improvement in the loss of energy (range, 1%–82%) was seen. Alpha-1 blocker treatment mediated the disappearance or decrease of the bulky vortex formation in seven patients, which led to an improved urinary stream. A positive correlation was found between improved energy loss and residual urine volume (P=0.0312).
Conclusion:
Alpha-1 blocker therapy led to a decreased energy loss in the urine flow in the prostatic urethra in relation to the improvement of clinical symptoms. The cystourethroscopy could be a tool to assess the urethral resistance in patients with BPH using image processing methodology.
Introduction
Urodynamic studies assess lower urinary tract function by measuring intraluminal pressure, volume of irrigant or urine, and the duration of the urination. Recent research has shown that urine velocity in the urethra can be calculated by using Doppler ultrasonography combined with video images. 9 These examinations are able to collect data that can be used to analyze the hydraulic phenomenon occurring inside the lower urinary tract. Based on these results, direct calculations of the energy loss of the urine flow can also be performed, which offers another approach for estimating the voiding dysfunction.
We have previously developed a method for obtaining three-dimensional (3D) coordinates of the intraluminal cavity of urinary tracts based on endoscopic video images in relation to voiding dysfunction. 10,11 A further study has led to the development of a method that makes it possible to construct a virtual urethra using cystourethroscopic video images. 12 By using this virtual 3D urethra construct, it is possible to simulate urine flow and calculate the energy loss associated with urination. 13
In this study, we analyzed the correlation between the alteration of the 3D structure of the prostatic urethra, which was obtained from cystourethroscopic video images, and the improvement of LUTS before and at 4 weeks after administration of the alpha-1 blocker, naftopidil. Data were further analyzed to evaluate whether this method could be a novel tool for estimating voiding function.
Materials and Methods
Study design
Cystourethroscopic video images were recorded before and 4 weeks after daily oral administration of 75 mg of naftopidil. The inclusion criteria consisted of no history of BPH treatment, having an International Prostate Symptom Score (IPSS) more than 8, a quality of life (QoL) index more than 3, and a prostate volume more than 20 cc. The study was approved by the local ethics committee, with all patients providing signed informed consent.
Hydraulic analysis using the virtual urethra
Video images of the prostatic urethra were recorded using a 16F flexible fiberscope. Under a constant saline irrigation pressure, the fiberscope was slowly pulled back from the bladder neck to the urethral sphincter. A Windows™-based personal computer captured the video images via an analog-digital converter. The 3D structure of the prostatic urethra was reproduced from the video files using software (EndoFlatter, Chiba University) 11 that extracted the 3D information of the tubular organs based on the intensity of the pixels in each frame (Fig. 1A). The data were subsequently rearranged for color and the information coordinated to create the final virtual space image using software (OVE, Chiba University: Fig. 1B). 12
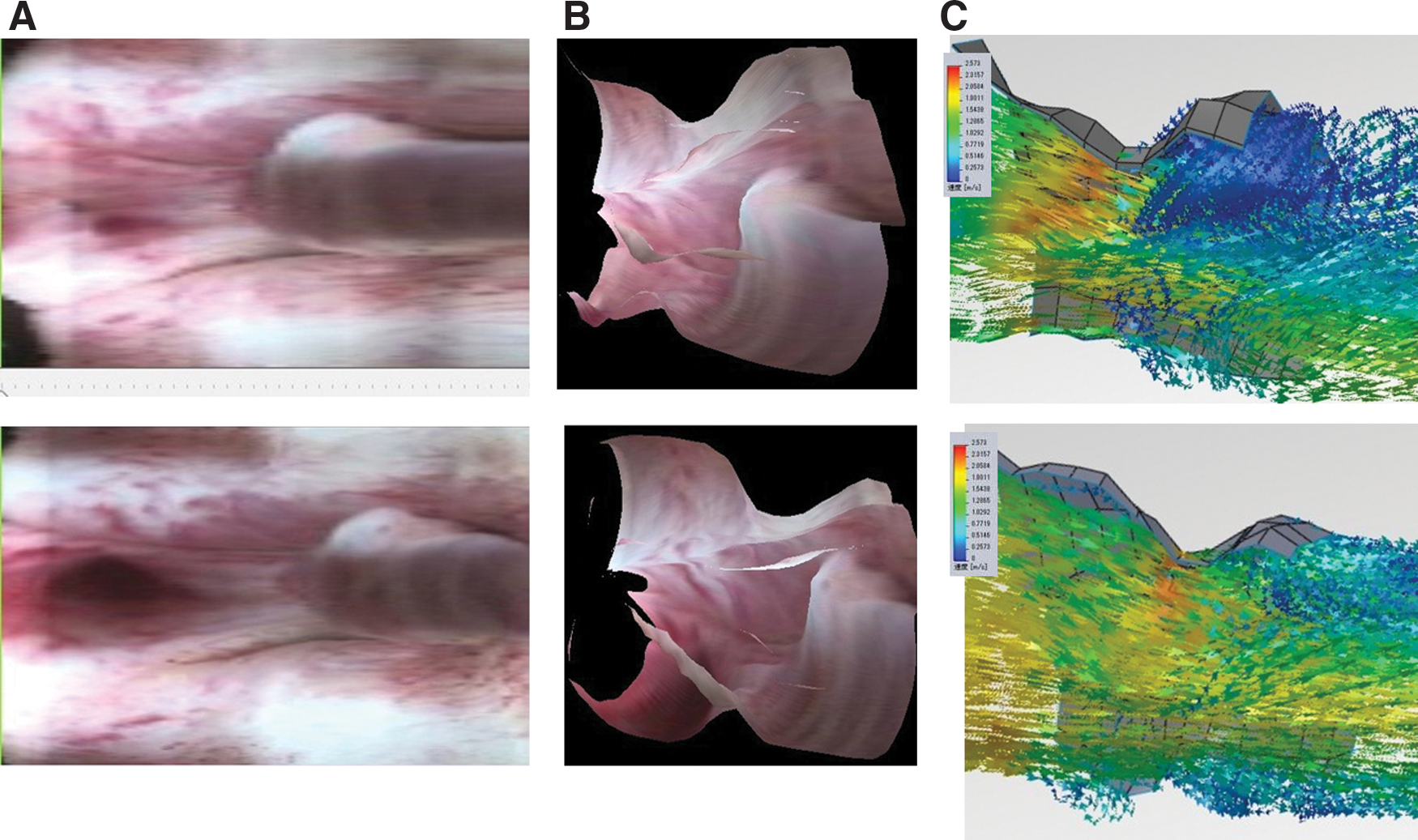
Top: Images before therapy. Bottom: Images after therapy.
As per a previously published method, 13 fluid dynamic analysis was then performed based on the reproduced 3D virtual urethral images. For this analysis, SolidWorks™ software (SolidWorks Japan, Tokyo, Japan) was used to create a prostatic urethra of the same length within the virtual space image. Hydraulic energy was calculated using the following formula: H=v2/2g+z+p/ρg, where H is hydraulic energy, v is velocity, g is gravity, z is height, p is pressure, and ρ is the density of water.
A constant bladder pressure was set in each patient. The relative level of energy was calculated at the bladder outlet and at the verumontanum. Correlations between the estimated losses of energy of the urine stream through the prostatic urethra and the clinical symptoms were then evaluated in the patients.
Statistical analysis
Statistical analysis was performed using analysis of variance. Values were considered significant at the level of P<0.05. JMP™ version 7.0.1 software (SAS Institute Inc., Cary, NC) was used for all calculations.
Results
A total of 11 patients with BPH were enrolled in the study. Patients' ages ranged from 58 to 86 years, with a median of 71 years. Ultrasonography-measured prostate volume ranged from 25 to 95 cc, with a median of 37 cc. Models for hydrodynamic simulation of the urine stream were successfully created based on the virtual endoscopy processing from the cystourethroscopic video images in all 11 patients. Using simulated velocity and pressure in the hydrodynamic models, we were able to calculate the relative energy loss during passage through the prostatic urethra.
In 9 of 11 patients studied, an 11% improvement in the loss of energy (range 1%–82%) was observed. After naftopidil treatment, a disappearance or decrease of the bulky vortex formation was seen in 7 of 11 patients (Fig. 1C), who exhibited an overall improvement of their symptoms, showing an improvement in the loss of energy in the intraluminal urine stream. When the energy level at the bladder outlet was set to 100%, the observed patient range was between 49.5% and 86.9%, with a median of 73.5% at the verumontanum level before naftopidil administration. After the therapy, the patient range was between 60.3% and 93.6%, with a median of 73.7%. Although naftopidil administration reduced the relative energy loss of the urine stream during passage through the prostatic urethra, this change was not significant.
Improvement of energy loss, however, was significantly correlated with improvements in the residual urine volume (P=0.0312, Fig. 2). Marginal significance was observed in the relationship between the improvement of energy loss and the improvement of the QoL index (P=0.0911). While a positive relationship existed between the improvement of the relative energy loss and the improvements of the IPSS or maximum flow rate (Qmax), significance could not be established because of the low patient sample number. No relationships were found between the age or prostate volume and the relative energy loss.
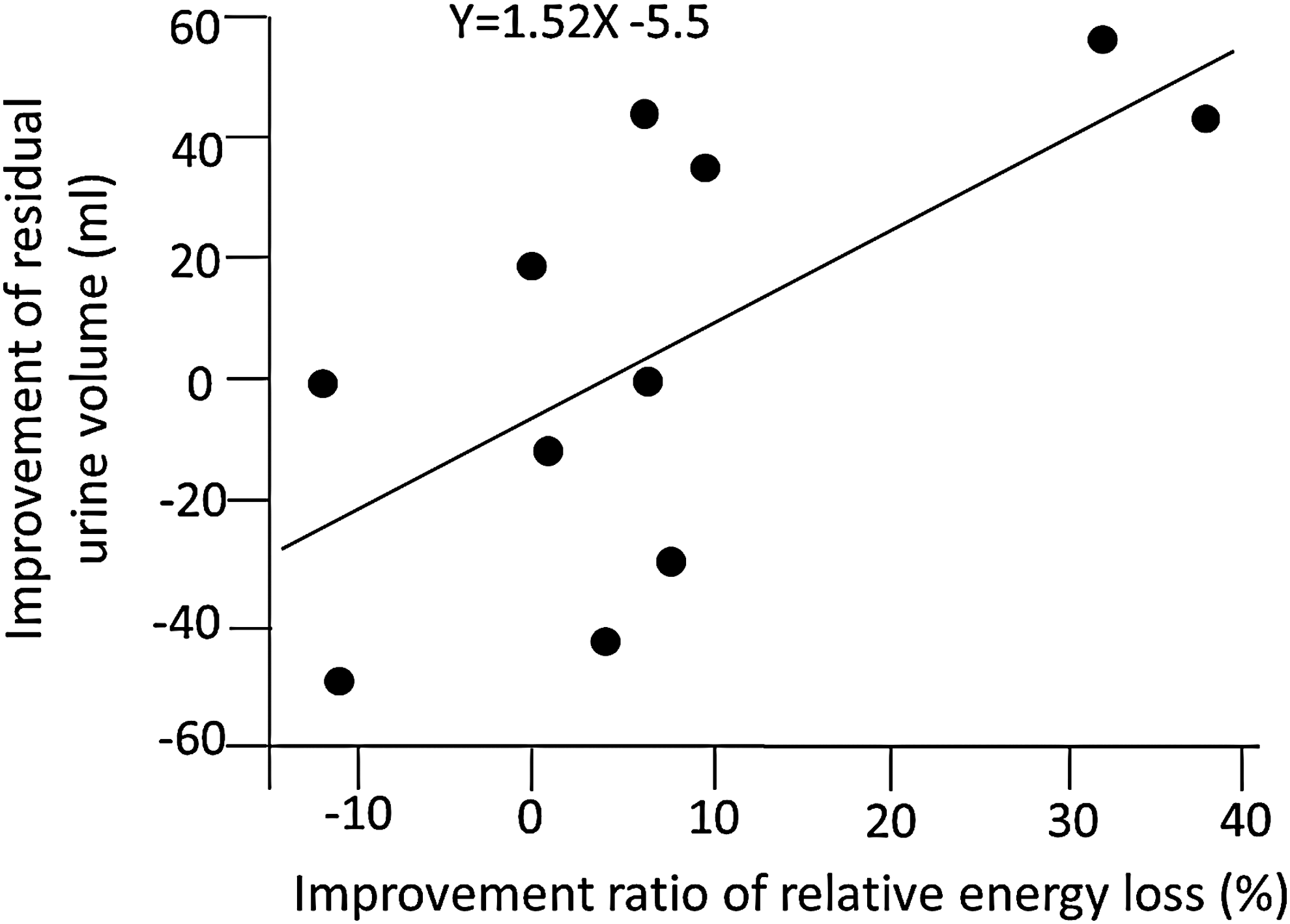
Relationship between the degree of improvement in the residual urine volume and the ratio of relative energy loss when compared before and after the therapy.
Discussion
Since the discovery that detrusor pressure exerted in the bladder is responsible for the hydraulic energy of the urine and that this pressure is reduced during passage through the urethra, many studies have tried to further analyze the hydraulic aspects of voiding dysfunction. Madersbacher and colleagues 14 used simple straight tube models to demonstrate that there is a loss of elasticity and a reduction of the hydraulic diameter of the bladder outlet and that this is important in voiding dysfunction. Glemain and coworkers 15 performed a pressure-flow study that investigated urethral resistance using elastic tubes as a model for BPH and documented the difficulty in calculating the exact hydraulic phenomenon in vivo. 15 Tojo and associates 16 calculated the urethral pressure at several points and showed that there was a hydraulic energy loss in patients with bladder outlet obstruction (BOO). 16 Using a virtual 3D model, we previously investigated the interference of the urine flow by a vortex in the urethra in patients with BOO and demonstrated the presence of a complex stream. 17 By being able to reconstruct a 3D structure of the urethra, this can potentially provide new methods for estimating the urethral resistance and a better understanding of the voiding function.
Although cadaver-based reconstruction of the urethra can provide spatial information on the urethra and adjacent organs, 18 it does not allow for reconstruction of an urethral cavity filled with urine. Contrast-enhanced MRI 19 or CT 20 technology may be able to potentially depict the physiologic status of the urethra during urination. While cystourethroscopy cannot document the physiologic status of urination, we were able to use a cystourethroscopic video image for reconstruction of a 3D structure of the prostatic urethra.
Our assumption in this study was that a retrograde irrigation would be able to reproduce the passive behavior of the urethra and would be similar to the actual conditions when exposed to the urinary stream during micturition. We tried to confirm our initial assumption by comparing the parameters of voiding dysfunction before and after administration of an alpha-1 blocker, which is known to dilate both the bladder outlet and the prostatic urethra. After administering this blocker, an enhanced dilation under pressure of the urine stream occurs. This dilation subsequently causes an improvement of the hydraulic energy loss during passage through the prostatic urethra.
In spite of the small number of subjects examined in the current study, our results demonstrated an improvement of the hydraulic energy loss in the virtual urethra that was calculated from the patients' cystourethroscopic videos. In addition, these data showed that this improvement was associated with a reduction of the residual urine volume and an improvement of the QoL index and the Qmax after therapy. Although this was not significant, it did show there was a positive relationship with the improvement of the IPSS. The present study, however, was unable to document any relationship between the improvement of the hydraulic energy loss and the changes in the flow rates.
Estimations of flow rate can be difficult to measure precisely, because they depend on the total urinary volume. 21 In some patients who have difficulty in voiding urine in an unfamiliar environment, this can lead to incorrect volume measurements. 22 Therefore, to ensure that correct flow rates can be calculated, the voided urinary volume needs to be collected under similar conditions and after a patient has become adjusted to the environment.
Residual urine volume measurements are a reliable way to determine volumes in patients with BOO, and these data can be used to detect the patient's potential risk in addition to being used to monitor the progression of disease. 23 Although the exact mechanism of residual urine in the bladder after ceasing urination has yet to be elucidated, a steeper reduction in the hydraulic energy of the prostatic urethra might have some effect on the early termination of the voiding reflex via an unknown pathway. Because voiding dysfunction is identical to an enhanced loss of the hydraulic energy of urine during passage through the urethra, subjective estimation may correspond to the hydraulic condition. Thus, the results of the present study could be indicative of the hydraulic phenomenon that occurs in the prostatic urethra.
The drawback of the present method is that it uses cystourethroscopy, which is considered to be an invasive examination. Use of flexible scopes under local anesthesia, however, makes this examination much more acceptable compared with examinations that use conventional rigid scopes. Our present results demonstrated the feasibility of using a flexible cystourethroscope to precisely process 3D images of the prostatic urethra, which made it possible to easily perform hydraulic simulation tests and calculate the energy loss. Conventional urodynamic studies are performed normally by measuring the intraluminal pressures of the lower urinary tract during the storage and voiding phase. The caliber of the flexible scope used to measure pressures is similar to catheters used during urodynamic examinations. As they become smaller, use of small cystourethroscopes instead of catheters may very well promote performing novel examinations that can be used to reconstruct the 3D structure of the urethra during micturition, thereby enabling a more accurate calculation of the hydraulic energy.
Endoscopic examination methods that allow simulation of urine flow inside the prostatic urethra and calculations that correspond to the parameters of voiding function may help in the future to detect critical lesions responsible for urethral resistance. Previous therapeutic modalities for LUTS have included transurethral resection of the prostate, holmium laser resection of the prostate, and transurethral incision of the prostate. 24 Other therapies that have been used include transurethral microwave thermotherapy, transurethral needle ablation, and high intensity focused ultrasound. 25 In addition, a recent report has also documented the efficacy of injecting botulinum toxin A into the prostate. 26
While development of these modalities has led to less invasiveness and a higher efficacy, the present study documents a potential alternative method that can be used for simulating urine flow before and after managing a critical lesion. This new method is less invasive and makes it possible to design a management plan based on virtual endoscopic images.
Conclusion
Using cystourethroscopic video image processing and hydraulic model reconstruction, we were able to successfully estimate the hydraulic energy loss in patients with BPH before and after administration of an alpha-1 blocker. This promising new methodology makes it possible to assess the urethral resistance in patients with BPH or BOO.
Footnotes
Acknowledgments
We thank Drs. K. Kawamura and T. Imamoto from the Department of Urology, Chiba University, and Dr. K. Mikami from the Department of Urology, Saiseikai Narashino Hospital, for their efforts in collecting the patients' data, and Mr. G. Sakuyama, Graduate School of Engineering, Chiba University, for support with our hydraulic calculation analysis.
Disclosure Statement
This research was sponsored by a National Grant of the Ministry of Education, Culture, Sports, Science and Technology in Japan (No.23659753), and a donation from Asahi Kasei Inc. to Dr. Igarashi. For the remaining authors, no competing financial interests exist.