
Abstract
Various improvements and modifications to the surgical treatment of benign prostatic hyperplasia have emerged over the last decade. Most techniques often initially claimed superiority only to turn out to be mediocre with time. Holmium laser enucleation of the prostate has been associated with superior outcomes compared with transurethral resection of the prostate and demonstrated improvement in long-term outcomes, while its clinical use has limitations. We describe the first use of plasma vaporization button electrode combined with loop electrode for transurethral vapor enucleation and resection of the prostate.
Introduction
During the past decade, a large number of new minimally invasive techniques, such as transurethral microwave thermotherapy, transurethral needle ablation, bipolar transurethral resection in saline (TURis), or laser procedures, have emerged. The most important recent innovation was the introduction of holmium laser enucleation of the prostate (HoLEP). Since its inception in 1996, HoLEP has been rigorously studied and has demonstrated long-term clinical improvement and a low rate of complications. 2,3 Despite proven efficacy, HoLEP has yet to become widely used because of the perceived steep learning curve and the costs associated with high power holmium laser systems. 4
Recently, a bipolar plasmakinetic vaporization system with a novel mushroom-like electrode was developed. As an alternative technique, the TURis plasma vaporization was described as a safe and effective treatment option for patients with LUTS from BOO. 5 In this study, we propose a “hybrid” technique that combines enucleation of the prostate gland with the plasma vaporization electrode and resection with a TURis cutting loop. We define this technique as transurethral vapor enucleation and resection of the prostate (TVERP).
Technique
The plasma vaporization electrode represents a new type of electrode with a special mushroom-like shape. It was initially performed for plasma vaporization of the prostate. We applied this electrode to enucleation of the prostate as well. The procedures were shown in Figure 1.
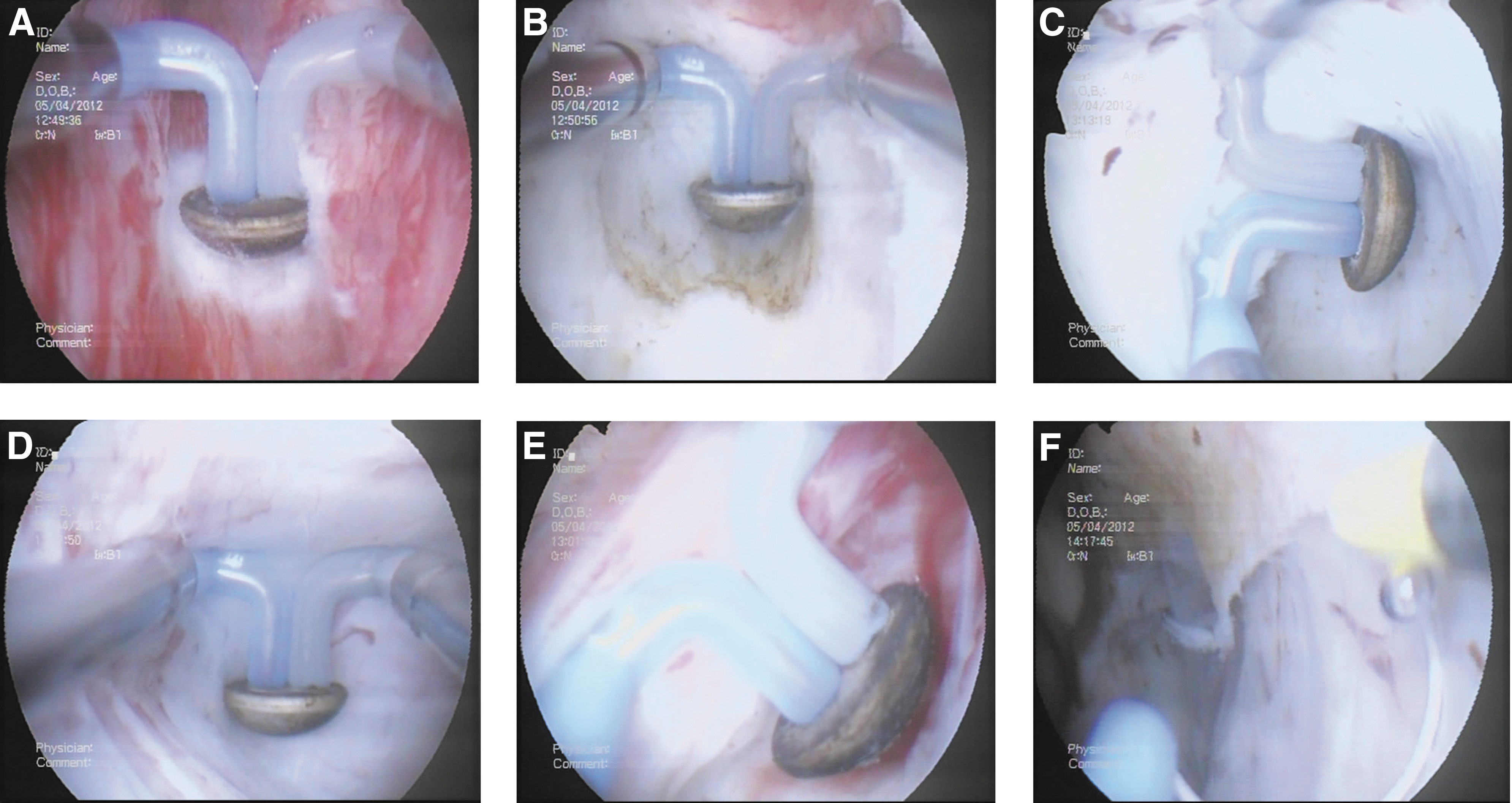
TVERP steps.
The patients were placed in a lithotomy position. The TVERP procedure was performed using the bipolar high-frequency generator with power output set at 300 W for vaporization and 150 W for coagulation, respectively. We used a technique similar to HoLEP. Initially, the ureteral orifices, bladder neck, and verumontanum were identified.
The enucleation was started with the button electrode by vaporization at the distal edge of the middle lobe close to the verumontanum. A circular vaporization was made from the 5 to 7 o'clock position deep into the surgical capsule, which was defined by its characteristic white circular fibers. The button electrode was then inserted into the groove and moved in retrograde fashion toward the bladder to make a plane between the adenoma and the surgical capsule. During the dissection, the button electrode was used to coagulate the vessels and vaporize the adhesive fibers.
As the detachment progressed close to the bladder neck, the bilateral lobes were then dissected with the electrode along the plane in a retrograde and transverse fashion in the same way. Thus, the prostate was subtotally enucleated except for the connection to the bladder neck. Then we changed the button electrode with a cutting loop, which shared the same resectoscope, high-frequency generator, and irrigation solution system. The nearly devascularized lobes were resected rapidly without serious hemorrhage.
Finally, the button electrode was used to coagulate tissue and create a smooth surface of the cavity. All the adenoma fragments were evacuated by Ellik. A 22F, three-way Foley catheter was inserted, and continuous irrigation was applied as necessary until hematuria resolved sufficiently.
Equipment
Olympus SurgMaster UES-40 bipolar generator (Olympus)
26Fr continuous flow resectoscope (Olympus)
Continuous saline flow irrigation system
Bipolar resection loop (Olympus)
Plasma vaporization electrode (Olympus)
Role in Urologic Practice
Between January 2011 and November 2011, we performed TVERP using the Olympus TURis button plasma vaporization electrode in 17 consecutive patients at our institution. All procedures were performed by a single surgeon. The patients were evaluated preoperatively by digital rectal examination, prostate-specific antigen measurement, International Prostate Symptom Score (IPSS), quality of life (QoL), and prostate weight calculated by transabdominal ultrasound. Patient characteristics, indications, operative time, the duration of catheterization and hospitalization, and complications were recorded. We determined postoperative IPSS, QOL score at 3 months. None of the patients needed blood transfusions. In all cases, no major complications occurred. Table 1 summarizes the perioperative results of our patients undergoing TVERP. A statistically significant and pronounced decrease in IPSS and QOL scores was observed after the operation.
P<0.05 compared with preoperative data.
SD=standard deviation; IPSS=International Prostate Symptom Score; QoL=quality of life.
Over the past decades, various alternative procedures have been challenging the role of traditional TURP for BPH surgical treatment. Among these minimally invasive techniques, HoLEP has been more thoroughly investigated and proposed as a size-independent new gold standard for treatment of BPH. 6,7 A steeper learning curve, a higher initial purchase cost, and difficulty in tissue removal have limited its popularity to some degree, however.
Initially, monopolar electrovaporization was introduced to vaporize the prostate with a specially designed roller electrode. 8 This procedure was gradually abandoned because of significant postoperative side effects, such as LUTS and incontinence, which were associated with a high amount of remaining tissue coagulation. 9 Recently, bipolar vaporization of the prostate was introduced, which have shown much smaller zones of tissue coagulation than the conventional monopolar vaporization. The bipolar vaporization system in this study, called TURis plasma vaporization electrode, was the most widely used one, which was launched in 2008 by Olympus. It has also been performed for the treatment of nonmuscle invasive bladder cancer. 10
By combining bipolar vaporization, enucleation, and bipolar resection, we named this technique TVERP. Although definitive conclusions cannot be drawn from these data because of the small number of patients and incomplete learning curve, we were able to provide immediate excellent outcomes following the TVERP technique as measured by improvement in IPSS and QoL; no complication occurred, indicating that the new technique was safe and effective for BPH in the short term.
Compared with HoLEP, TVERP has several strengths. First, because of the excellent hemostatic characteristics of bipolar vaporization, the new technique can be performed with improved intraoperative vision. Second, the morcellator is not needed during the surgical procedure; thus, the risk of bladder mucosal injury will be avoided. Third, the costs associated with upgrading preexisting bipolar systems and the single-use electrode are much lower than HoLEP.
Conclusion
TVERP seems to represent a promising endoscopic treatment alternative for BPH. Because of the superior hemostasis characteristic, this procedure could be specially applied to high-risk patients with large prostates. Further prospective trials with large sample size and long-term follow-up are needed to affirm the value of this technique and its place in the current armamentarium of BPH therapy.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.