
Abstract
Background and Purpose:
Prolonged warm ischemia time (WIT) and operative time (OT) during robot-assisted partial nephrectomy (RAPN) can adversely affect renal function and clinical outcomes. Minimizing the duration of WIT and OT is critical to achieving good results postoperatively. Our standard technique for RAPN has evolved into an intracorporeal preparation (ICP) that minimizes the reliance on the first assistant. The goal of the current study was to analyze outcomes after ICP RAPN compared with those of the standard RAPN.
Patients and Methods:
A retrospective review of all patients who underwent RAPN was performed, comparing standard vs ICP technique. The ICP approach involves tacking of preprepared sutures along the abdominal sidewall adjacent to the kidney in preparation for hemostasis and renorrhaphy before arterial clamping, the use of robotic Scanlan® Reliance, bulldog clamps preplaced near the hilum of the kidney, and “sliding-clip” renorrhaphy. We compared intraoperative (OT, WIT, estimated blood loss [EBL]) and pre/postoperative outcomes (serum creatinine, glomerular filtration rate [GFR], length of stay [LOS]) of RAPN between the ICP and standard approach.
Results:
A total of 44 consecutive RAPNs (18 ICP, 26 standard) were performed. Median nephrometry score was 7a, and mean follow-up was 13 months. Mean tumor size was 2.4 cm, and most common stage was T1a. There was no significant difference between ICP and standard RAPN with regard to nephrometry score and stage. Mean WIT was significantly lower for the ICP vs standard RAPN (19 vs 23 min, P=0.049) as was mean OT (161 vs 204 min, P=0.027). On multivariate analysis, ICP RAPN was an independent predictor of WIT (P=0.02). There was no significant impact on preoperative and postoperative GFR for either approach. EBL and LOS were similar between the two groups.
Conclusions:
The ICP RAPN leads to a significant reduction in WIT and OT while maintaining similar perioperative outcomes compared with the standard approach.
Introduction
The da Vinci® robotic system (Intuitive surgical, Sunnyvale, CA) was introduced in 2000 and has been quickly adopted for many urologic procedures. Its ease of use compared with standard laparoscopic technique and wide range of instrument maneuverability have led to its increased use for robot-assisted partial nephrectomies (RAPN) and made it the fastest growing robotic procedure in 2008. 7 Recent studies have shown equivalency in cancer control along with shortened learning curves with RAPN compared with conventional laparoscopic approaches. 8 –12
Warm ischemia time (WIT) continues to be a limiting factor in laparoscopic approaches. A maximum acceptable WIT of 30 minutes has been described, 13 although many series suggest that every minute has an aggregate effect on the final outcome. 14 –17 In addition, with each 1-minute increase of ischemia time, acute renal failure is more likely to develop. 18 Technical advancements in the RAPN procedure—sliding clip renorrhaphy, zero-ischemia for hilar tumors, and early unclamping—have led to decreasing WIT and improved outcomes. 19 –21
RAPN continues to evolve and, through our experience, we have developed a novel RAPN approach—the First Assistant Sparing Technique (FAST) RAPN. This technique is aimed at further decreasing WIT and operative time by using a completely intracorporeal preparation (ICP). This technique involves strategic positioning of all sutures and robotic Scanlan® bulldog clamps intracorporeally before clamping, so as to minimize reliance on the first assistant during the resection and repair of the tumor and defect. These modifications allow the surgeon to further control WIT while minimizing the impact of the first assistant on this important metric.
We outline our FAST RAPN technique and report the resulting operative and clinical outcomes before and after its inception. We hypothesize that the ICP technique will lead to decreased WIT and OT compared with the standard, more first-assistant dependent, technique of RAPN.
Patients and Methods
A retrospective review of our Instituitional Review Board approved oncology database was performed for patients who underwent RAPN. The records of 44 consecutive patients who underwent RAPN from 2009 through 2011 by two separate surgeons (JL, KKB) were identified. Patient demographics and preoperative, intraoperative, and postoperative variables were collected. Preoperative variables included tumor size, stage, location, Fox Chase R.E.N.A.L (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score, serum creatinine (Cr), and glomerular filtration rate (GFR). Intraoperative and postoperative clinical variables included OT, WIT, estimated blood loss (EBL), length of stay (LOS), transfusion requirements, serum Cr, and GFR. Postoperative pathologic variables included tumor stage, size, margin status, and histology. Serum GFR was calculated using the Modification of Diet in Renal Disease equation. Recurrence and progression were also assessed based on postoperative CT or MRI performed based on annual surveillance for pT1 tumors. Recurrence was defined as a newly enhancing lesion in the region of the old resection site that was then pathologically confirmed to be of similar histology as the primary lesion. Progression was defined as distant metastases seen on CT or MRI.
FAST
RAPN at Columbia University Medical Center was performed with our standard approach until 2011. In this method, after dissection of the renal hilum, laparoscopic bulldog clamps were applied by the first assistant as typically performed during laparoscopic partial nephrectomy. Successful achievement of renal ischemia is confirmed with intracorporeal color-flow Doppler ultrasonography. After excision of the tumor with cold scissors, 2-0 monofilament absorbable suture was used to close any collecting system defects, followed by selective figure-of-eight suture ligation of visible arterioles or venules in the resection bed using 4-0 monofilament absorbable suture. Renorrhaphy is then performed using the sliding clip technique along with a hemostatic bolster made of cellulose polymer (Surgicel,® Ethicon, Somerville, NJ) and hemostatic matrix (Floseal, Baxter Biosurgery, Deerfield, IL). 19 Individual sutures are passed by the first assistant as needed during the repair of the defect. Once the repair is complete, the first assistant laparoscopically removes the bulldog clamps, and hemostasis is confirmed visually.
From July 2011, we have developed a fully ICP of RAPN in an effort to decrease OT and WIT. This approach to RAPN relies on prepositioning of all required sutures intracorporeally. After dissection of the renal hilum, a 3-0 monofilament barbed suture (V-Loc,™ Covidien, Mansfield, MA) followed by three to four size 0 polyglycolic acid sutures (Vicryl, Ethicon, Somerville, NJ) with Weck Hem-o-lok® ligation clips (Teleflex, Research Triangle Park, NC) and absorbable suture clips (Lapra-Ty, Ethicon-Endo, Cincinnati, OH) loaded approximately 1 cm from the tail of the sutures are tacked into the abdominal sidewall hanging above the kidney (Fig. 1). This allows for easy access to the suture once the renorrhaphy commences. The sutures are all placed near each other in line along the back wall, and all placed one by one during reconstruction. The needles are not cut until after all steps are completed and bulldog clamps are removed, and hemostasis achieved; only then are the needles cut and removed sequentially. In addition, all team members are aware of suture and bulldog counts.
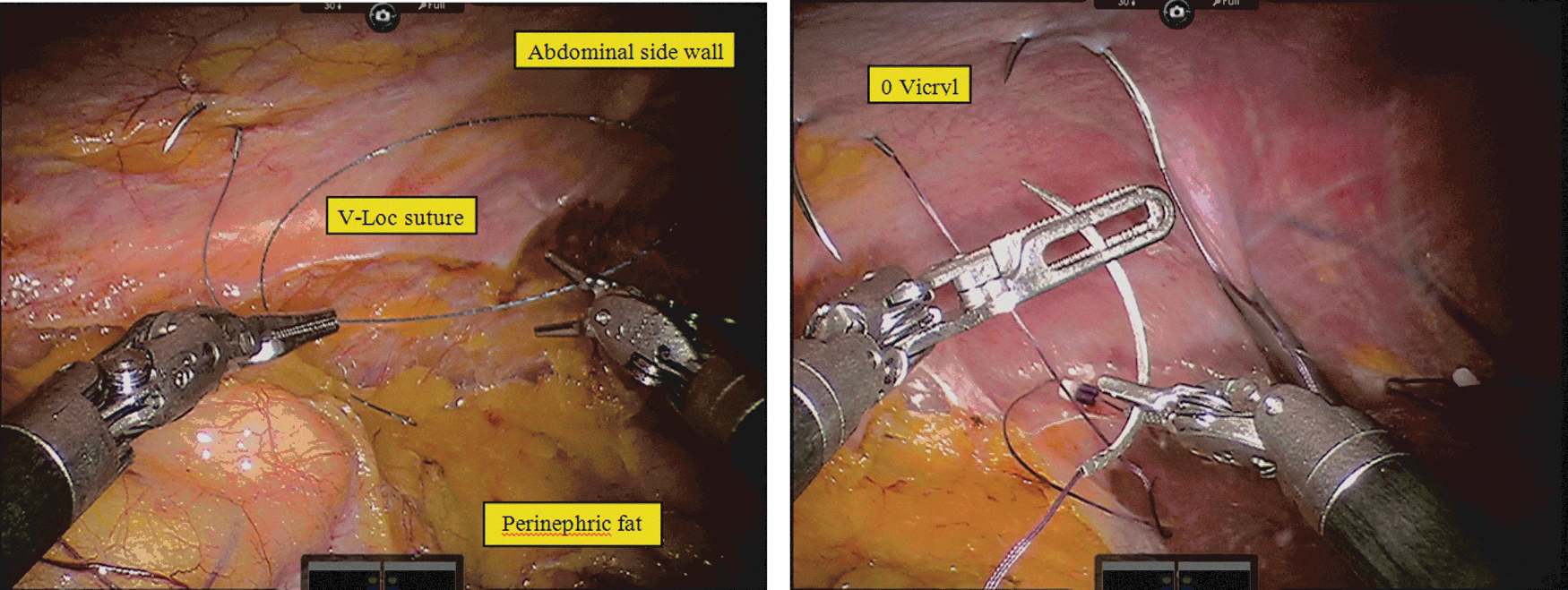
Intracorporeal preplacement of sutures in preparation for renorrhaphy before hilar clamping. All needles are tacked to the abdominal sidewall near the kidney and defect for easy access during repair.
Robotic Scanlan® Reliance bulldog clamps are then introduced intracorporeally by the first assistant and then positioned adjacent to the renal hilum in the perirenal fat (Fig. 2). Each bulldog has a 2-inch silk suture tail tied to the end so that in the event that it falls away, it can be grasped easily and removed from the body. All sutures and bulldog clamps are placed within a 30-degree range of motion of the camera arm so as to provide easy and quick access when performing renorrhaphy and to minimize misplacement of sutures and bulldog clamps. Clamping of the renal artery is then solely performed by the console surgeon using the da Vinci Prograsp™ forceps (Intuitive Surgical, Sunnyvale, CA). We perform clamping of the renal artery only (with selective clamping when feasible) using one or two bulldogs clamps as needed.
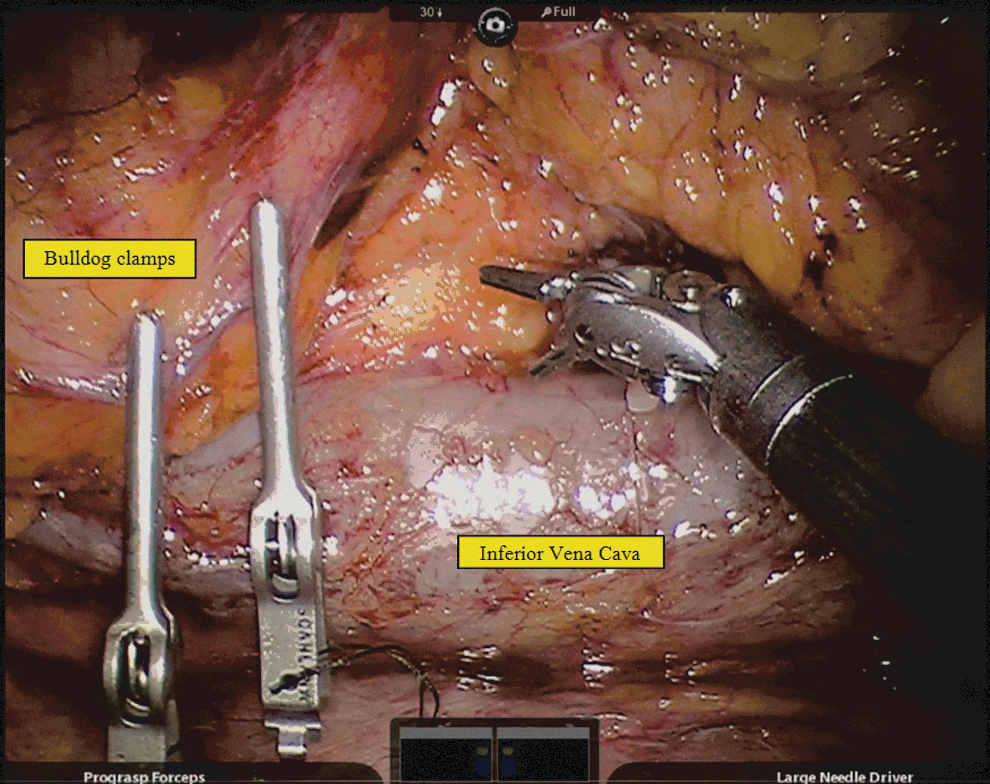
Robotic Scanlan® bulldog clamps positioned adjacent to the hilum in the perirenal fat in preparation for clamping.
With the FAST technique, the first assistant is then only used for dynamic retraction and suction during WIT for tumor excision and placement of the Hem-o-lok clips when performing the sliding clip renorrhaphy. Cutting and removing sutures along with placement of Lapra-Ty clips is performed after bulldog clamps are removed. The remainder of the RAPN is performed in the standard fashion. Of note, excellent verbal communication during this portion of the operation is imperative between the console surgeon and the assistant and all operating room staff. A preclamping flight check of all the steps and necessary sutures and equipment is imperative.
Statistical analysis
Patient data were analyzed based on their respective RAPN technique—either the standard or FAST approach. Demographic variables were then compared using the chi-square test or Student t test where appropriate. Preoperative, intraoperative, and postoperative variables were also compared between the two approaches using the chi-square and Student t test. Univariate and multivariate linear regression models were used to determine significant predictors of OT, WIT, and GFR. A P value of < 0.05 was considered statistically significant for all analyses (STATA version 11.0, College Station, TX)
Results
A total of 44 consecutive patients were included in the study, 18 of whom underwent FAST RAPN. The mean age of the entire cohort was 56 years (standard deviation [SD] 12.8), mean body mass index (BMI) was 30 (SD 6.8), and 61% of the cohort was male (Table 1). The majority (77%) of patients had a Charlson Comorbidity Index (CCI) score ≤2 (Table 1). No differences were observed between the two groups for age, sex, race, BMI, or CCI (Table 1). Median follow-up time was significantly longer for the standard group compared with the FAST group (45 vs 2 mos, P<0.001) (Table 1). Overall mean preoperative tumor size was 2.6 cm (SD 0.96), median nephrometry score was 7a, mean GFR was 84 mL/min/1.73 m2, and the majority of patients were cT1a (93%) (Table 2). Tumors were evenly divided between right (48%) and left (52%) sides (Table 2). There were nonsignificant differences between FAST vs standard RAPN groups with regard to preoperative tumor size, side of tumor, nephrometry score, clinical stage, or preoperative GFR (Table 2).
FAST=first assistant sparing technique; BMI=body mass index; CCI=Charlson Comorbidity Index.
FAST=first assistant sparing technique; GFR=glomerular filtration rate; OT=operative time; WIT=warm ischemia time; EBL=estimated blood loss; LOS=length of stay.
Patients who underwent FAST RAPN had a significantly shorter mean OT (164 min, SD 42) compared with patients undergoing the standard technique (204 min, SD 54, P=0.01) (Table 2). Similarly, mean WIT was significantly shorter for the patients who underwent FAST vs standard RP (18 vs 23 min, P<0.01) (Table 2). There was no difference in EBL between the groups. One patient who underwent the standard technique experienced a urine leak. Average length of stay was 1.8 days (SD 0.99) (Table 2). There was no difference between the standard and FAST groups for pathologic tumor size, margin status, histology type, or recurrence rate (Table 3). Overall, mean pathologic tumor size was 2.5 cm (SD 1.3), the majority of patients were pT1a (59%), had negative margins (95%), and had clear-cell type renal carcinoma (57%) (Table 3). In addition, there was no difference found in postoperative GFR between standard vs FAST RAPN (79 vs 74 mL/min/1.73 m2) (Table 3).
FAST=first assistant sparing technique; GFR=glomerular filtration rate.
On multivariate analysis, preoperative GFR was the only significant predictor (P<0.001) of postoperative GFR when controlling for technique (FAST vs standard), preoperative tumor size, clinical stage, nephrometry score, CCI, BMI, and EBL (Table 4). With regard to OT and WIT, using the FAST approach to RAPN was a statistically significant independent predictor of both outcome measures when controlling for clinical stage, tumor size, BMI, and nephrometry score (P=0.03, P<0.001 respectively). BMI was also a significant determinant of both OT and WIT on multivariate analysis (P<0.01, P=0.03 respectively) while nephrometry score was also an independent predictor of WIT (P=0.001) but not OT (Table 4). Preoperative tumor size and clinical stage were not significantly associated with either OT or WIT (Table 4).
CI=confidence interval; FAST=first assistant sparing technique; BMI=body mass index; GFR=glomerular filtration rate; CCI=Charlson Comorbidity Index; EBL=estimated blood loss.
Discussion
This study establishes that the introduction of a new technique that minimizes the surgeon's reliance on the first assistant during the ischemic portion of RAPN has a significant impact on perioperative outcomes—namely, WIT and total OT. By performing an ICP RAPN, the surgeon may directly apply suture and bulldog to the renal hilum in a controlled fashion within a staged operative field, thereby maximizing efficiency and decreasing the number of surgical steps compared with the more first-assistant dependent technique. The current study supports the hypothesis that FAST RAPN decreases WIT and OT compared with traditional RAPN as demonstrated by the findings of several multivariate models. We show that the FAST technique is an independent predictor of WIT and OT when controlling for other important operative variables such as the nephrometry score, tumor size, and stage (Table 4).
WIT continues to be a major technical consideration and the main measurable parameter for the quality of PN. While the maximum acceptable time has been debated, it is generally considered that the lower the WIT, the less cellular damage to nephrons and in turn the better the functional outcome. In a recent international and multicenter retrospective analysis of 349 patients undergoing RAPN, Ficarra and associates 22 demonstrated that the level of surgeon experience was the most significant predictor of a WIT >20 minutes in both univariate and multivariate models. In addition, clinical tumor size and other anatomic characteristics were predictors of longer WIT. Furthermore, in a comprehensive review of the impact of WIT on kidney damage, Becker and colleagues 23 recommended a WIT of 20 minutes or less to avoid damage to the kidney. Thomson and coworkers 18 analyzed subjects with a solitary kidney to determine an acceptable cut-point for WIT. While they recommended a threshold of either 20 or 25 minutes, when WIT was analyzed as a continuous variable, it proved to be a significant predictor of adverse functional outcomes. This was compelling evidence for the authors to conclude that every minute of WIT counts. Although not ultimately significant, a study by Lane and colleagues 15 corroborated these findings, reporting that the length of ischemia time appears to be a risk factor for acute renal injury and thus that extended WIT will perpetuate adverse outcomes.
The cumulative experience with the robotic platform in recent years has shown decreased adverse events, improved outcomes, and decreased WIT. Minimizing renal exposure to ischemia remains a fundamental goal during PN, and research focusing on achieving this outcome is of critical importance. In a study of laparoscopic WIT vs cold ischemia, Foyil and associates 24 showed a direct correlation between WIT and a Cr clearance decrease. Further, in a porcine model with a solitary kidney, it was shown that a WIT of 30 and 60 minutes caused early renal dysfunction in 43% and 100% percent of pigs, respectively. 25 In another pig model, it was shown that even a WIT as short as 16 minutes induces a significant loss of nephrons. 26
In addition to the implications of a reduced WIT, the FAST technique also affords another important benefit in enabling the console surgeon to function and progress during a critical portion of the operation in a fashion that is relatively independent of the first assistant. Although it is often implicitly acknowledged as a significant factor, few studies have looked at the impact of the first assistant on surgical outcomes. In fact, in a review of RAPN, Reyes and coworkers 27 stated that an experienced bedside assistant is essential, and performs vital tasks including application of the vascular pedicle clamps, retraction and suction during tumor excision, and introduction of suture and bolster material.
San Francisco and colleagues 28 underscored these sentiments in a description of their early unclamping technique for RAPN; they wrote, “The role of the bedside assistant cannot be underestimated during both kidney mobilization and tumor resection.” Indeed, the steps the bedside assistant must perform in RAPN such as traction/counter-traction, placing and removing laparoscopic bulldog clamps, effectively clearing the operative field of blood, rapidly introducing and retrieving sutures, and placing laparoscopic clips during reconstruction are necessary and key to the outcome of the surgery. Our novel description of FAST removes the majority of these key steps from the hands of the first assistant, thereby minimizing the surgeon's reliance on the assistant's skill set, and in turn allowing modification and control of a previously intangible variable in the operation.
Moreover, while the literature underscores the role of the bedside assistant during RAPN, many articles have cast the reliance of the console surgeon on such an assistant as a per se limitation of the robotic technique. In the aforementioned article, San Francisco and associates 28 also stated that “major disadvantages of RAPN…include the lack of surgeon control of hilar clamping and unclamping, [and the] requirement for an experienced bedside assistant.” A review of current RAPN perspectives and future prospects by Gautam and coworkers 7 also concluded that the need for a skilled and experienced bedside assistant was a potential limitation of the robotic approach. Certainly, the impact of the first assistant during the course of robotic surgery transcends the field of urology alone, as Seamon and colleagues 29 clearly delineate delineate the necessity of a well-trained first assistant in their standardization of the hysterectomy for endometrial cancer. They comment that adequate exposure is the key to a successful procedure, and a skilled bedside assistant is essential in developing the dissection. Based on these prevailing opinions toward the first assistant in robotic surgery, as well as our unique experience, the current study suggests that the FAST approach to RAPN offers a benefit by allowing the surgeon to control the hilar clamping portion of the operation and thus minimize WIT.
Despite the important implications of this investigation, several inherent limitations warrant recognition. First, this study was conducted using a single surgeon's approach to FAST RAPN, and although the technique was introduced using several different first assistants, it has yet to be validated in a larger surgeon/first-assistant subset. Second, given the relatively short duration of follow-up, this study establishes the impact of FAST on perioperative but not long-term renal functional and oncologic outcomes. Third, a learning curve bias may confound our findings in that the OT and WIT decreases associated with FAST RAPN could in part be explained by improved surgical efficiency from experience alone regardless of technical modification.
While both WIT and OT are potentially reduced because of moving further along the learning curve, the surgeons who performed the standard technique had previously performed more than 500 PNs and both are minimally invasive fellowship trained surgeons with extensive experience. At the point that the patients were reviewed, presumably both surgeons were far along their learning curve and the impacts on WIT and OT are therefore from a change in technique. Consequently, our analysis should be beyond the learning curve of this procedure. Future directions in researching this technique could include a return to standard RAPN with a comparison of clinical outcomes to the FAST RAPN. We are confident, however, that this technique is an improvement and, therefore, unlikely to revert to the traditional technique in clinical practice at this time. A prospective randomized multisurgeon trial is warranted to substantiate our findings and add to the continued refinement of RAPN.
Conclusions
Our approach with a maximally intracorporeal preparation is a technical approach to RAPN that uses (1) a staged operative field, and (2) the application of sutures and bulldog clamps by the console surgeon. This model reduces the reliance of the surgeon on the first assistant's skill set during a critical portion of the operation, which affords a durable impact on important perioperative outcomes of WIT and total OT. Further studies are necessary to determine the impact of this technique of RAPN on renal functional and oncologic outcome.
Footnotes
Acknowledgments
William Berg is funded by a grant provided by the Doris Duke Charitable Foundation.
Disclosure Statement
No competing financial interests exist.