
Abstract
Background and Purpose:
Anatomic parameters determining renal mass complexity have been used in a number of proposed scoring systems despite lack of a critical analysis of their independent contributions. We sought to assess the independent contribution of anatomic parameters on perioperative outcomes of laparoscopic partial nephrectomy (LPN).
Patients and Methods:
Preoperative imaging studies were reviewed for 147 consecutive patients undergoing LPN for a single renal mass. Renal mass anatomy was recorded: Size, growth pattern (endo-/meso-/exophytic), centrality (central/hilar/peripheral), anterior/posterior, lateral/medial, polar location. Multivariable models were used to determine associations of anatomic parameters with warm ischemia time (WIT), operative time (OT), estimated blood loss (EBL), intra- and postoperative complications, as well as renal function. All models were adjusted for the learning curve and relevant confounders.
Results:
Median (range) tumor size was 3.3 cm (1.5–11 cm); 52% were central and 14% hilar. While 44% were exophytic, 23% and 33% were mesophytic and endophytic, respectively. Anatomic parameters did not uniformly predict perioperative outcomes. WIT was associated with tumor size (P=0.068), centrality (central, P=0.016; hilar, P=0.073), and endophytic growth pattern (P=0.017). OT was only associated with tumor size (P<0.001). No anatomic parameter predicted EBL. Tumor centrality increased the odds of overall and intraoperative complications, without reaching statistical significance. Postoperative renal function was not associated with any of the anatomic parameters considered after adjustment for baseline function and WIT. Learning curve, considered as a confounder, was independently associated with reduced WIT and OT as well as reduced odds of intraoperative complications.
Conclusion:
This study provides a detailed analysis of the independent impact of renal mass anatomic parameters on perioperative outcomes. Our findings suggest diverse independent contributions of the anatomic parameters to the different measures of outcomes (WIT, OT, EBL, complications, and renal function) emphasizing the importance of the learning curve.
Introduction
A number of systems have attempted to provide a quantifiable complexity measure for renal masses in consideration for NSS. 2 –4 These scores are composed of different anatomic parameters including tumor size, location, centrality, and growth pattern. Despite the interest in these systems, there has been no comprehensive and critical analysis of the individual score components and their independent contribution to renal mass complexity as determined by perioperative outcomes.
In this study, we sought to gain insight into the independent associations of renal mass anatomic parameters to perioperative outcomes in a cohort of consecutive patients undergoing laparoscopic partial nephrectomy (LPN).
Patients and Methods
After approval from the Institutional Ethics Committee, we retrieved records of consecutive patients undergoing transperitoneal LPN by a single surgeon (AT) between 2005 and 2011 from our prospectively collected database. Only patients with a single renal mass were included. Patients with aberrant kidney anatomy (ie, horse-shoe) were excluded. Preoperative contrast-enhanced CT were independently reviewed (SU, AW, AT) for anatomic parameters, including tumor size, side, growth pattern, location, and centrality. Disagreements were settled between the three reviewers.
Growth pattern was categorized in mostly exophytic, mesophytic, or endophytic based on the portion of renal mass located underneath the renal capsule surface (<50%, ∼50%, >50%). Location was classified on several planes: Anterior/posterior, medial/lateral, and polar (upper pole, lower pole, interpolar with demarcation lines being axial planes corresponding to the medial lips of the kidney contour). Tumor centrality was classified as hilar (direct contact with major renal vessels and/or renal pelvis), central (direct contact with collecting system and/or sinus), or peripheral. Spherical masses were defined as those with no single tumor dimension exceeding another by >20%.
The following perioperative variables were analyzed: Demographics, serum creatinine before surgery and at discharge, operative times (OT), warm ischemia times (WIT), estimated blood loss (EBL), intra- and postoperative complications. Estimated glomerular filtration rates (eGFR) were calculated using the modified Modification of Diet in Renal Disease formula. 5 Postoperative complications were classified according to the Clavien-Dindo system. 6 OTs were calculated “skin-to-skin.” Blood loss and OTs of any concomitant procedures performed were subtracted from the totals.
Statistical analyses
The following outcomes were considered for multivariable analyses: WIT, OT, EBL, total complications, intraoperative and postoperative complications, as well as eGFR at discharge. Multivariable linear (WIT, OT, EBL, eGFR) and logistic regressions (complications) were used to determine associations. All models were adjusted for sex, age, and year of surgery. For the WIT model, LPNs with no hilar clamping were excluded. Additional model-specific adjustments were made to isolate the impact of tumor anatomic aspects. The OT model was additionally adjusted for WIT, the eGFR model for preoperative eGFR and WIT, and the EBL model for OT. All complications models were adjusted for WIT and OT.
Multivariable analyses are presented with forest plots of the coefficients/odds ratio estimates and the corresponding 95% confidence intervals. Statistical analyses were performed with R v.2.13 (the R Foundation for Statistical Computing, Vienna Austria) using the Hmisc, Design, and metafor libraries. Data are presented as median (interquartile range) or number (percent) unless otherwise specified.
Results
A total of 147 patients undergoing LPN met the inclusion criteria. Patient and tumor characteristics are detailed in Table 1. Of note, tumor size ranged from 1.5 to 11 cm, most tumors were either mesophytic or endophytic, and central tumors accounted for more than one half of the cohort with hilar tumors representing 14% of the total. In nine (6%) cases, LPN was performed “off-clamp,” and these cases were excluded from WIT analyses.
Excluding laparoscopic partial nephrectomy off clamp.
eGFR=estimated glomerular filtration rate; WIT=warm ischemia time; PN=partial nephrectomy; EBL=estimated blood loss; RCC=renal-cell carcinoma.
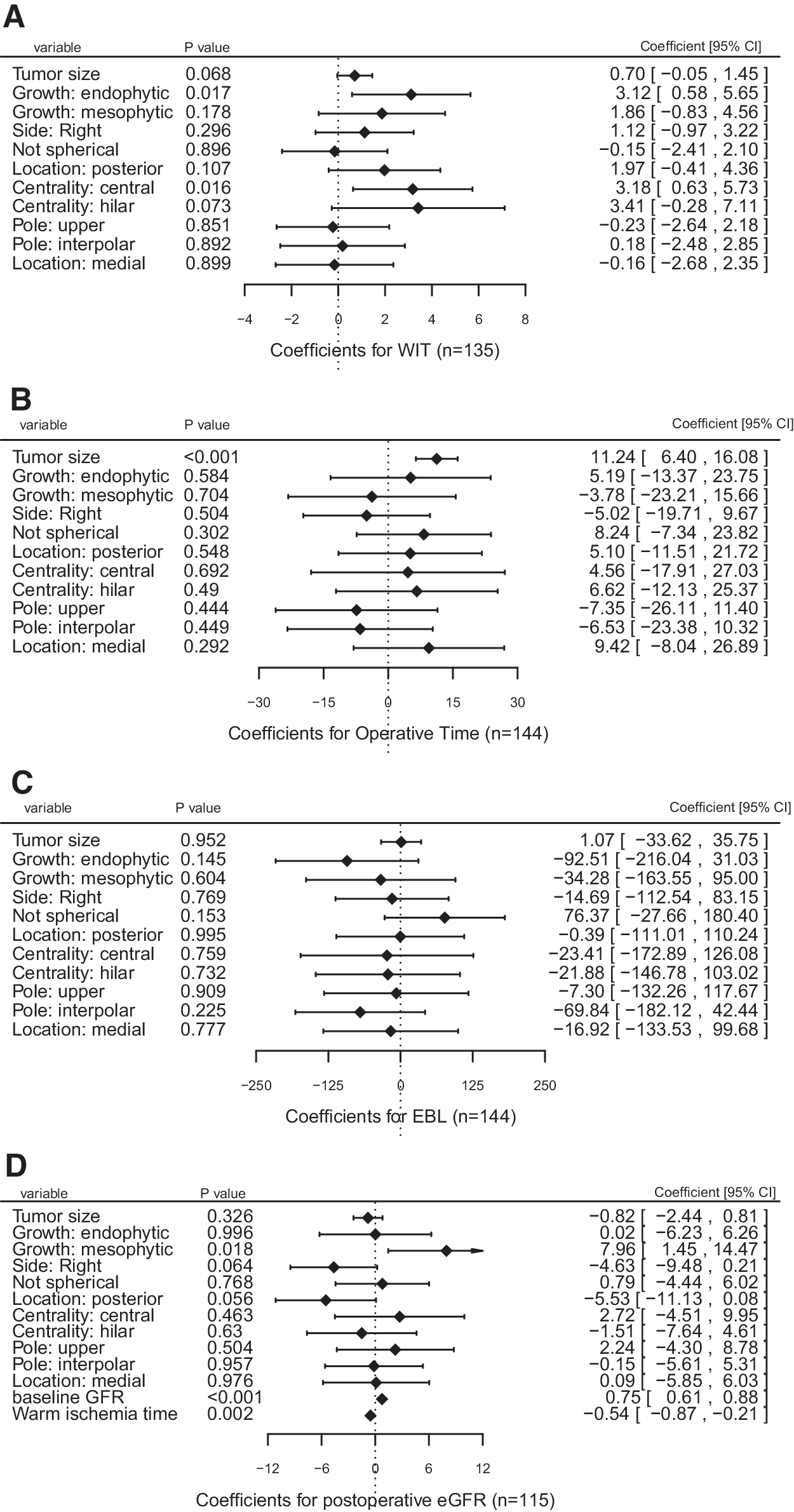
Results of the WIT analysis are detailed in Figure 1A. When adjusted for demographics and year of surgery, several anatomic parameters were associated with WIT: Namely, larger tumor size (P=0.068), endophytic growth pattern (P=0.017), and both central and hilar mass location increased WIT (P=0.016 and P=0.073, respectively). Polar location was not independently associated with WIT.
Coefficents for
Only larger tumor size was independently associated with OT (P<0.001) when adjusted for demographics, WIT, and year of surgery (Fig. 1B). None of the remaining anatomic parameters appeared to correlate with OT. As shown in Figure 1C, none of the considered anatomic variables significantly affected EBL, although nonspherical morphology appeared to be associated with increased EBL (P=0.153) without reaching statistical significance.
The analysis for postoperative eGFR is reported in Figure 1D. Baseline eGFR and WIT demonstrated the strongest associations with postoperative eGFR. Interestingly, when adjusted for baseline eGFR and WIT, mesophytic growth pattern appeared to be protective from eGFR decline (P=0.018).
A total of 15 (10.1%) intraoperative complications occurred, including bleeding (n=7) and conversions to radical nephrectomy (n=3). Postoperative complications occurred in 18 (12%) of patients with major complications (Clavien≥III), accounting for the majority of events (Table 2).
POVH=postoperative ventral hernia; p.o.=postoperatively.
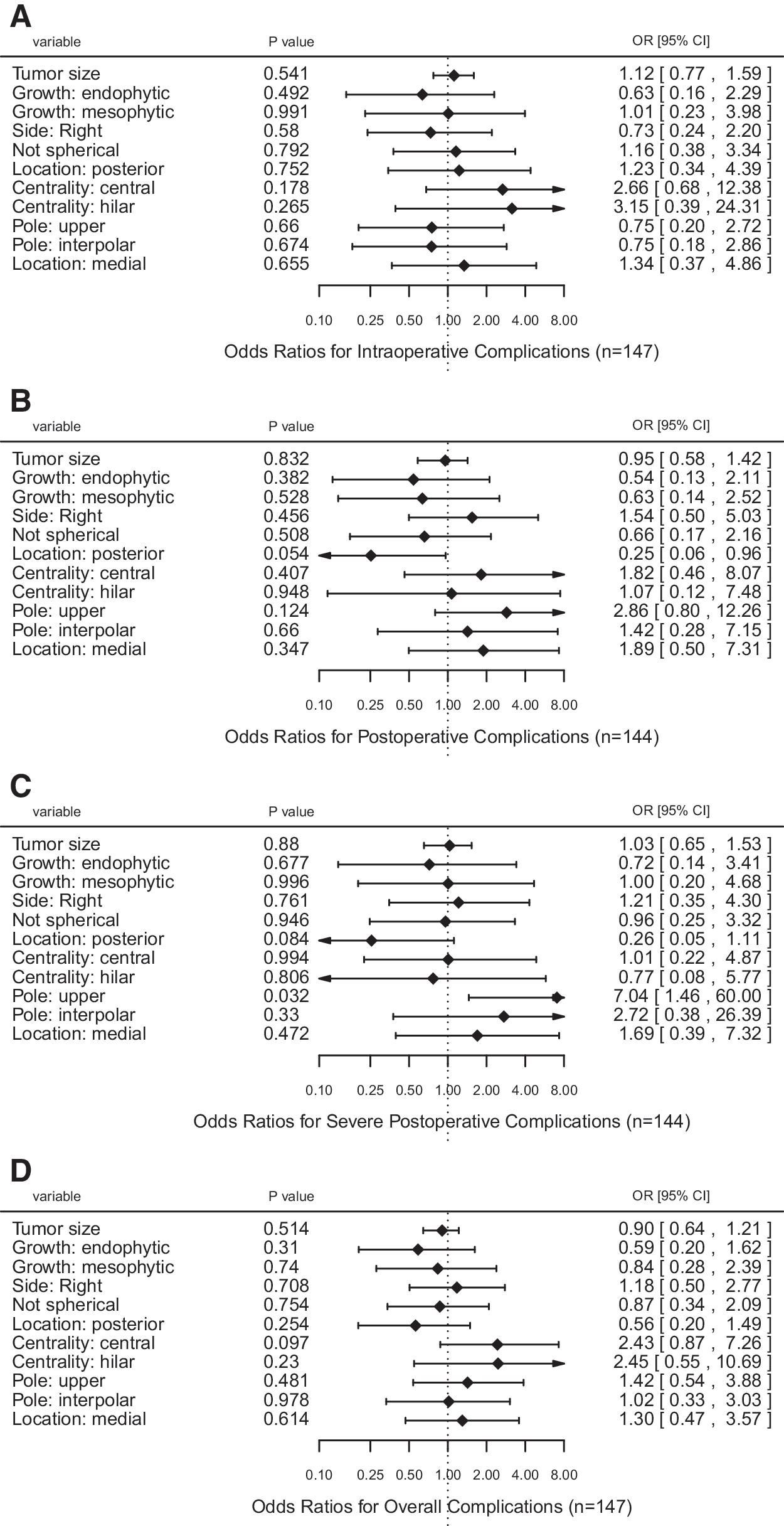
Tumor centrality demonstrated the strongest association with overall complications, as shown in Figure 2D. Central and hilar location increased the odds of complications 2.4-fold and 2.5-fold, respectively (P=0.097 and P=0.230). Analysis of intraoperative complications (Fig. 2A) did not reveal any statistically significant associations with anatomic parameters of the tumor, although central and hilar location increased the odds of intraoperative events 2.7-fold and 3.2-fold, respectively (P=0.178 and P=0.265). With regard to postoperative complications (Fig. 2B), posterior tumor location appeared to be protective (odds ratio [OR]=0.25, P=0.054), and central location increased the odds (OR1.8, P=0.407). For major complications (Fig. 2C), we noted an inverse association with posterior tumor location (P=0.084) and a direct association with upper pole location (P=0.032). The estimates confidence ranges remained wide for all anatomic parameters except tumor size, however.
Odds ratios for
Interestingly, a later year of surgery was significantly associated with reduced WIT and OT (P<0.001 for both) and reduced odds of intraoperative complications (P=0.023), suggesting a strong influence of the learning curve on these perioperative outcomes.
Discussion
NSS has become the standard of care for most renal masses whenever technically feasible. The measure of tumor complexity is subjective, however. Recently, a number of quantification systems were proposed to better describe renal mass anatomic features to enable comparability of the published literature. 2 –4 Despite the evident interest in these scoring systems and suggestions that the nephrometric scores may be associated with surgical outcomes, 7 –12 critical appraisal of the role of component renal mass anatomic parameters in perioperative outcomes of NSS is lacking. In this study, we used refined statistical methods to evaluate the influence of renal mass anatomy and found that the associations are complex, have different magnitudes, confer diverse clinical significance, and may be associated with some but not other outcomes that can be used to define complexity.
The nephrometric systems proposed consider the following anatomic parameters: Tumor size, growth pattern, nearness to or involvement of the collecting system, anterior/posterior as well as medial/lateral location, albeit using different definition criteria. We chose to use the same anatomic criteria, with some modifications. Polar location was evaluated using the limits proposed by one system (R.E.N.A.L. [radius; exophytic/endophytic; nearness; anterior/posterior; location]) whereas medial/lateral location was borrowed from another (P.A.D.U.A. [preoperative aspects and dimensions used for anatomic]).
We chose to assess centrality by classifying tumors as hilar, central, or peripheral. This decision was based on the objective difficulty to accurately estimate the nearness to the collecting system as proposed by Kutikov and colleagues 2 on 5-mm tomographic cuts. On the other hand, dichotomizing centrality based on involvement of the collecting system appeared to us as oversimplification. In addition, we introduced a novel parameter—renal mass shape—hypothesizing that nonspherical lesions may add to the complexity.
Perioperative outcomes are generally considered as a proxy for a higher degree of surgical challenge. Because the learning curve for minimally invasive NSS is important in defining these outcomes, 13,14 all analyses were adjusted for year of surgery, a surrogate for learning curve, which indeed demonstrated strong associations with WIT and OT, as well as intraoperative complications. This suggests that progressing with the learning curve in this series, we were able to reduce WIT, OT, and rates of intraoperative complications. Furthermore, this finding is of importance, indicating that analyses of outcomes of NSS (particularly those dealing with anatomic variables) should be adjusted for the learning curve to adequately assess independent associations. Of note, we could not find a published report on the aforementioned nephrometric scores that had considered learning curve in their statistical analyses.
Our findings indicate that tumor size, growth pattern, and tumor centrality are associated with increased WIT after adjustment for potential confounders, similar to other reports. 15 –18 Of note, none of the above studies performed multivariable analyses adjusting for the learning curve, whereas our data show this to be an important confounding variable.
Our analysis suggests that only tumor size was strongly and independently associated with OT. Notably, among the included confounding variables, both WIT and year of surgery were associated with OT. In concert with our findings, Eng and coworkers 16 found tumor size to be associated with OT in their series of 153 LPN. Interestingly, in the study by Venkatesh and associates 18 that focused on tumor growth pattern, they found endophytic tumors had increased OT on univariable analysis; however, our model shows no association when adjusted for confounders.
While EBL is commonly considered an important perioperative outcome that may reflect the actual difficulty of the surgery, our analyses did not show any statistically significant independent associations between anatomic characteristics of the mass and EBL. Interestingly, endophytic growth pattern appeared to be associated with decreased EBL. This likely reflects an effect of the learning curve not completely mitigated by adjustments of the analysis. In fact, endophytic tumors are generally considered technically challenging and are less likely to be challenged early in the learning curve. A second finding of interest is that nonspherical tumors appeared to increase EBL; albeit, it did not reach statistical significance.
Our analysis confirms the current body of literature indicating that anatomic features of renal masses do not independently predict postoperative renal function. 19 –21 Our results show preoperative eGFR and WIT as the strongest predictors of postoperative eGFR with the narrowest confidence intervals (Fig. 1D). This finding is similar to that reported by Lane and colleagues 21 in their analyses of a large series of solitary kidney partial nephrectomies whereby postoperative renal function was independently associated with baseline GFR and percent parenchyma spared, while tumor characteristics lost statistical significance on multivariable analysis. Interestingly, Lane and coworkers 21 found that adjusting for nonmodifiable factors reduces the statistical impact of ischemia times on postoperative renal function (P=0.08).
In our analysis, mesophytic growth pattern, right-sided, and posterior location appeared to near statistical significance. We observed, however, higher baseline eGFR values for mesophytic and posterior tumors (P<0.001 for both) that may have driven these results.
Our findings suggest that among anatomic characteristics of the renal mass, only tumor centrality is potentially associated with intraoperative and overall complications (Figs. 2A–D), although the statistical power is limited for these analyses. This contrasts with other reports using nephrometric scores whereby higher tumor complexity assessed based on a sum of anatomic characteristics has been reported to correlate with individual complications, such as urine leak, 8 and overall perioperative 9 and postoperative 10 complications. Other series have failed to demonstrate this association. 11,12
On the other hand, several reports have associated tumor centrality alone with NSS complications. Venkatesh and associates 18 have found hilar tumors more prone to complications, and another study 22 suggested corticomeduallary tumor location to increase the risk of complications. Our data corroborate these findings with the additional refinement of controlling for year of surgery, an important confounder.
In this study, we provide a comprehensive analysis of the impact of renal mass anatomic parameters on perioperative outcomes of LPN. We submit that several anatomic parameters are independently associated with perioperative outcomes. The individual anatomic features used by the currently available nephrometric scores, however, are not uniformly predictive of outcomes in this series, suggesting that caution should be exercised in using these validated tools. Tumor size and centrality may have the strongest associations with outcomes that define renal mass complexity. Most importantly, we emphasize the importance of the learning curve in defining perioperative outcomes.
Our study is limited by its retrospective nature, despite the prospective collection of data. Moreover, selection of less complex renal masses in the early experience may have introduced selection bias that we attempted to mitigate by adjusting for the year of surgery, whereas currently, almost the totality of renal masses presenting at our institution are treated with minimally invasive partial nephrectomy. Further, we did not adhere to the exact classification of anatomic parameters as used in the available proposed scores because the intention of this study was not to validate the existing system but rather to critically analyze the factors (ie, centrality, growth pattern, and so on) in relation to outcomes. In addition, we excluded patients with multiple tumors and aberrant anatomy and our findings may not apply to these specific populations. Finally, this is a single center report that requires validation in other cohorts.
Conclusions
This study represents the first comprehensive analysis of the impact of anatomic parameters on perioperative outcomes of LPN while adjusting for the learning curve. In this series, the anatomic parameters used by the current nephrometric scoring systems did not uniformly predict perioperative outcomes. Our findings suggest diverse independent contributions of the anatomic parameters to the different measures of outcomes (WIT, OT, EBL, complications, and renal function) emphasizing the importance of the learning curve. These data provide a critical appraisal and constructive criticism on the proposed nephrometry systems in an effort to refine the objective measurement of renal mass complexity.
Footnotes
Disclosure Statement
No competing financial interests exist.