
Abstract
Optimal control of the dorsal venous complex (DVC) is a critical step in robot-assisted radical prostatectomy (RARP). If DVC is not controlled properly, bleeding may occur during the apical dissection. On the other hand, if it is controlled well, a bloodless field is attained and, thus, a precise apical dissection and urethral division is possible. Suture ligation is the most common technique used for dorsal vein control, while some authors recommend using an endovascular stapler. Recently, athermal division and selective suture ligation technique has been reported for DVC control. We describe a new technique: Use of a bulldog clamp to control the DVC during RARP. The control of the DVC with a bulldog clamp allows a bloodless field with precise apical dissection and provides preservation of maximum urethral length while avoiding sphincteral injury.
Introduction
Endovascular stapler ligation is another common technique used for dorsal vein control. 4,5 It has been underlined that firing of the large stapler device would not provide adequate visualization of the apex before division of the DVC. 7 Athermal division with selective suture ligation is another technique that has been reported for DVC control. 8,9
To the best of our knowledge, this is the first article that describes the use of a bulldog clamp to control the DVC during RARP. The control of the DVC with a laparoscopic bulldog clamp allows precise and bloodless apical dissection, maximum preservation of urethral length beyond the apex of the prostate, and avoids distal sphincter mechanism injury.
Technique
Patients
We started to use the laparoscopic bulldog clamp to control DVC before apical dissection and urethral transection in March 2011 after performing 450 RARP cases.
Until now, we applied this technique in 120 patients, and 50 of these patients have a minimum follow-up of 3 months. The technique is described and developed by the senior author (ARK).
Surgical technique
1. The patient is placed in a low lithotomy steep Trendelenburg position, and both arms are attached to the sides. Pneumoperitoneum is established by insertion of a Veress needle through the Palmer point. As described by Menon and associates, 2 a six port configuration with transperitoneal access is used.
2. First the peritoneum is incised, and the Retzius space is entered by using a 0-degree scope. Then after opening the endopelvic fascia, the levator ani muscles are pushed away from the prostate. The lateral surface of the prostate is exposed, and both puboprostatic ligaments are divided.
3. The scope is changed to a 30-degree downward position, and bladder neck dissection is started. For a neurovascular bundle sparing technique, seminal vesicle isolation and control of the lateral pedicle are performed with athermal dissection. Neurovascular bundle dissection is completed.
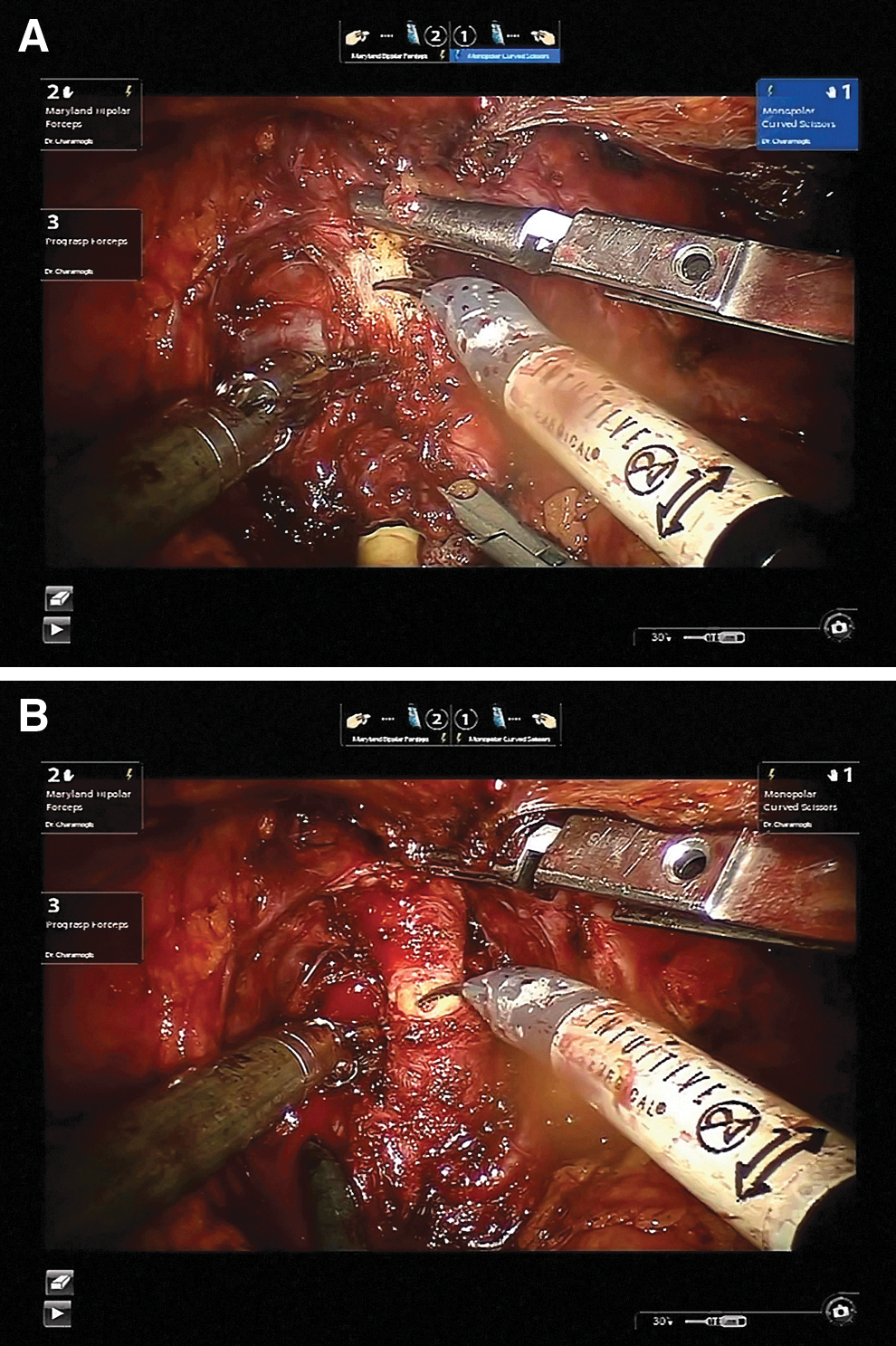
4. The DVC is controlled with a laparoscopic vascular bulldog clamp (Solos Endoscopy, Inc, Boston, MA). The bulldog clamp is inserted by the bedside surgeon (Figs. 1A-1B). The clamp has a freedom of motion within the applicator (Fig. 2). While the clamp is in place, the prostate is pulled cranially by the bedside surgeon. When the dorsal vein is too large to grab with the bulldog clamp, the prostate is grabbed with the Prograsp forceps attached to the fourth arm. This maneuver constricts the large dorsal vein and enables grabbing with the bulldog clamp. If there is a large bony outgrowth on the symphysis, the 30-degree scope is changed to an upward position, and the DVC is seen clearly. Although the placement of the bulldog clamp can be more difficult with the scope in an upward position, this can be accomplished without any further problem. These kinds of manipulations can be performed in different scenarios.
5. Apical dissection, division of the DVC and the urethra are performed under bloodless clear vision. Then Maryland bipolar forceps and monopolar scissors are switched to the needle drivers.
6. After removal of the bulldog clamp by the bedside surgeon, the DVC is selectively sutured with 2/0 polyglactin suture. The same suture is then passed through the periosteum of the symphysis pubis for periurethral suspension (anterior reconstruction).
7. A single simplified Rocco stitch is placed on the midline for posterior reconstruction. 10 Ultimately, urethrovesical anastomosis is performed by using two 18-cm 2/0 Biosyn™ sutures with the van Velthoven technique. 11

Free motion of the bulldog clamp within the applicator.
Equipment
• 0 degree scope
• Maryland bipolar forceps
• Monopolar scissors
• 30 degree scope
• Laparoscopic vascular bulldog clamp with a freedom of motion within the applicator (Solos Endoscopy, Inc, Boston, MA).
• 2 needle drivers
• 2/0 polyglactin suture with UR-6 needle for selective DVC ligation and anterior reconstruction
• 2/0 polyglactin suture with UR-6 needle for posterior reconstruction
• 1 dyed and 1 undyed 2/0 Biosyn suture with UR-6 needle for urethrovesical anastomosis
Role in Urology Practice
The control of the DVC, apical dissection, and urethral transection are the crucial steps of RARP. Radical prostatectomy-related urinary incontinence can be reduced by preservation of urethral length beyond the apex and avoiding damage to the distal sphincter mechanism. 1 Because the depth of the suture cannot be seen clearly, it may injure the urethra and distal sphincteral mechanism and decrease the functional urethral length by compacting the urethra. 5,6 An optimum length of membranous urethra has been reported to be related with early continence recovery. 12 Sometimes the DVC stitch may loosen and be dislocated during apical dissection. This may cause bleeding and make apical dissection complicated. Resuturation of the DVC may be needed (Fig. 3).

Loosening of the dorsal vein suture and bleeding from the dorsal venous complex.
Endovascular stapler control of the DVC is somewhat blind and may cause urethral and external sphincteral injury. In addition, there would be an extra cost for each stapler use. Tewari and Tan 7 stressed that firing of the large stapler device would not provide adequate visualization of the apex before division of the DVC and reported a retroapical approach for apical dissection. In their technique, they used a 30-degree upward lens to facilitate retroapical and lateral dissection of the apex and membranous urethra. They performed suture ligation of the DVC and apical transection after precise dissection of membranous urethra and prostatic apex. They reported the preservation of the external sphincter and urethral stump to be better with this technique. They also had significantly lower positive apical surgical margin rates. 7
In our series, none of the patients had apical surgical margin positivity. Because the number of patients is small, it is not possible to make any comment that this technique improves the surgical margin positivity rate at the apex.
In our technique, using the bulldog clamp to control the DVC enabled a bloodless and clear vision of the apex allowing fine apical dissection without interfering with the anatomy. The length of the urethral stump is found to be adequate, and external sphincteral trauma is minimized.
Accessory pudendal arteries (APAs) have been supposed to have an important role to maintain erectile function and continence after radical prostatectomy. Approximately 25% of patients undergoing laparoscopic radical prostatectomy have APAs identified during the operation. 13,14 Because APAs are in close proximity with the DVC, if there is any APA, it can be identified and preserved well with the bulldog technique compared with other techniques.
Lei and colleagues 8 and Guru and coworkers 9 reported an athermal division and selective suture ligation technique for DVC control. In this technique, increasing pneumoperitoneum may be necessary to control arterial bleeding. Although rare, transfusion may also be needed. In our technique, because control of the DVC is optimal with the bulldog clamp and there is no bleeding, no additional intervention such as increasing pneumoperitoneum is necessary.
Because control of the DVC with the bulldog clamp allows a bloodless and precise vision of the urethra and apical anatomy, apical dissection is supposed to be faster, resulting in shorter total operative time. Beside this, as reported by Lei and associates, 8 omitting the instrument change for suture ligation of the DVC may contribute to shorter operative time. Also, optimal membranous urethral length may permit faster and easier urethrovesical anastomosis.
Using a laparoscopic bulldog clamp with a freedom of motion within the applicator allowing for angulations according to each patient's prostate apical anatomy is essential. This maneuver allows optimal positioning to obtain effective control of the DVC. This technique enables better control of the DVC and view of apical anatomy during RARP. This may lead to less trauma of the external sphincter and establishes a longer urethral stump.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.