
Abstract
Background and Purpose:
CT has become a well-established modality in the evaluation of urinary calculi. The advent of multidetector CT (MDCT) scanners and submillimeter thick slice acquisitions has yielded CT images with even greater resolution. MDCT scanners allow for source data slice acquisition with submillimeter slice thickness. These source images can then be reconstructed to thicker slices for more convenient interpretation of the CT scan. Previous authors have looked at the effect of slice thickness on detection of urinary calculi. We investigated whether the thin slice source images yielded detection of additional stones and the potential significance of detecting these additional stones.
Patients and Methods:
Ninety-five consecutive patients who were referred to our outpatient imaging center for CT, with a clinical history placing them at risk for urinary calculi, were included in the study.
Results:
In 49 (52%) of the 95 patients, more calculi were visualized using the 0.625-mm thick images than with the 5-mm thick images. In 34 (69%) of these 49 patients, the additional findings were thought to be “clinically significant,” while in the remaining 15 (31%) patients, the additional findings were not thought to be clinically significant. In 46 (48%) of the 95 patients, there were no additional urinary calculi identified on the 0.625-mm thick images compared with that observed on 5-mm thick images.
Conclusion:
The results from this study encourage reviewing the thin slice source images of MDCTs in patients at risk for urinary calculi, because important clinical decisions may hinge on the additional findings made on these images.
Introduction
We investigate the value of reviewing the 0.625-mm thick source images obtained on a 64-slice MDCT compared with the 5-mm thick reconstructed images in patients at risk for urinary calculi and assess the potential significance of detecting these additional small calculi.
Patients and Methods
Ninety-five consecutive patients referred to our outpatient imaging center for CT, with a clinical history placing them at risk for urinary calculi, were included in the study (scans were obtained from January to June 2006) and evaluated in a prospective fashion. These patients presented with hematuria without history of urinary malignancy (39 cases), history of urinary calculi (34 cases), flank pain or colic (20 cases), or hyperparathyroidism (2 cases). This study was approved by our institution's Institutional Review Board. All CT scans interpreted in this project were performed for clinical indications, and there was no additional scanning performed on these patients because of this study.
Examinations were primarily read by one radiologist, and the results were confirmed by a second radiologist. All examinations were reviewed in the following manner: 5-mm thick images were first interpreted, and the presence of stones was noted. Then in the same review session, that same radiologist reviewed the 0.625-mm thick slices to assess for stones. Results were confirmed by a second radiologist. Discrepancies were settled by consensus. Soft tissue window settings were typically used.
All images interpreted for this study were obtained without intravenous contrast and reviewed in the axial plane. Depending on the clinical indication for the examination, patients may have had additional images obtained after administration of intravenous contrast as well. This study was compliant with the Health Insurance Portability and Accountability Act.
All images were reviewed on a Picture Archiving and Communication System workstation (Centricity, GE, Milwaukee, WI). All patients were scanned on a 64-slice MDCT (VCT, GE, Milwaukee, WI). Source images were obtained at 0.625 mm, automatic exposure control (variable mAs), and a kVp of 120 was used for all 95 patients.
All three radiologists are board certified in radiology. Two have completed abdominal imaging fellowships and all three interpret abdominal CTs on a regular basis. The term “clinically significant” was applied to calculi seen on the 0.625-mm thick CT slices but not on the 5-mm thick slices, whose identification thus potentially altered the diagnosis or treatment of the patient.
MDCT scanners obtain data by using multiple thin slices that then get reformatted to thicker slices. For instance, the 64-slice scanner used in this project obtains all images at 0.625-mm and then reconstructs these data into more “reader friendly” thicker slices if desired. If 5-mm thick images are desired, data are acquired at 0.625 mm and then eight of these thin slices are reconstructed into one 5-mm thick image. These 0.625-mm “source images” are readily available for review, however. If 2.5-mm thick reconstruction is desired, at a similar noise factor (image quality) as the 5-mm thick slice, the radiation dose for acquiring the data to make two 2.5-mm slices is actually greater than for one 5-mm thick slice. It must be emphasized, however, that all MDCT scanners acquire the data in thin slice fashion. These thin slices are then reconstructed to 2.5 mm, 5 mm, or whatever possible reconstruction is desired.
There is no real financial difference in obtaining the scans at 0.625 mm or reconstructed at 5 mm. The cost for such things as storage of the additional data, if desired, for the greater number of images being obtained (eight 0.625-mm thick slices are needed for one 5-mm thick slice) is negligible.
Results
In 49 (52%) of the 95 patients, more calculi were visualized using the 0.625-mm thick images than with the 5-mm thick images. In 34 (69%) of these 49 patients, the additional findings were felt to be potentially clinically significant, while in the remaining 15 (31%) patients, the additional findings were not felt to be clinically significant. In 46 (48%) of the 95 patients, there were no additional urinary calculi identified on the 0.625-mm thick images compared with that observed on - mm thick images.
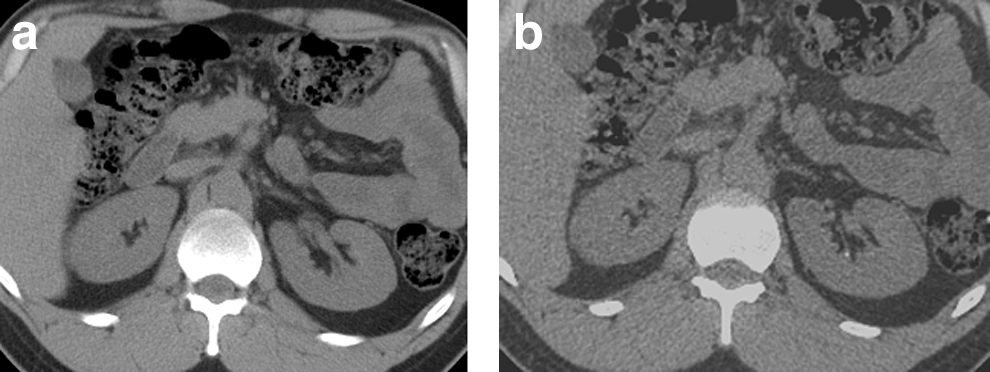
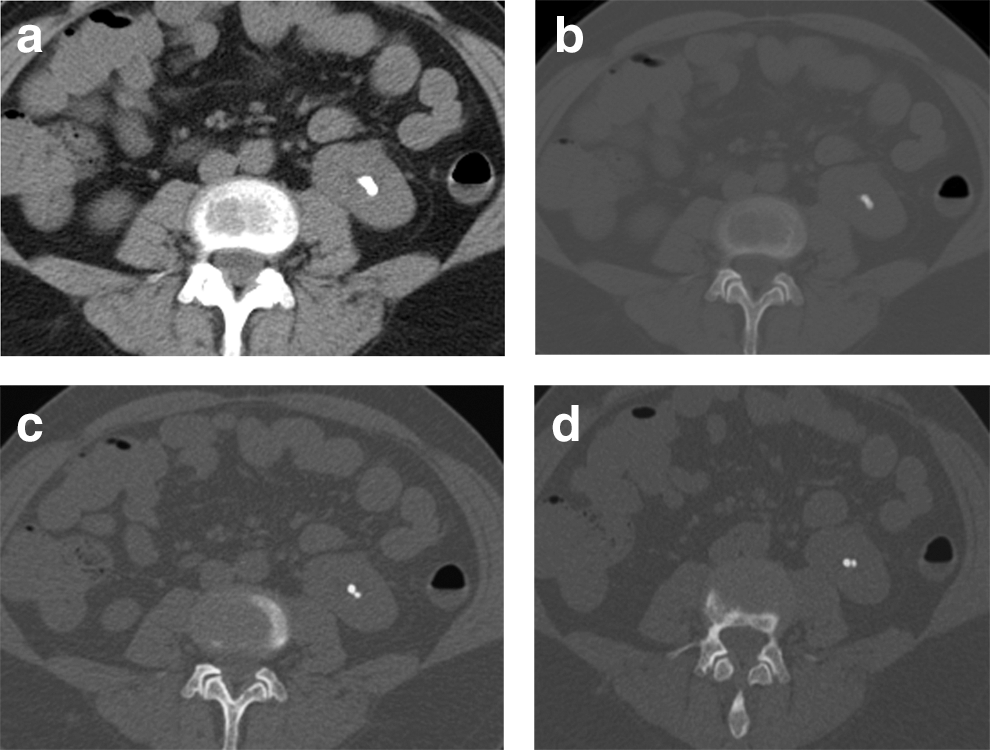
In the 34 patients in whom additional urinary calculi were seen on 0.625-mm thick images and thought to be potentially clinically significant, two of these patients had a history of hyperparathyroidism and were being evaluated for the presence of renal calculi. No calculi were seen on the 5-mm thick images; however, in both cases, 1- to 2-mm calculi were identified on the 0.625-mm images. Seventeen of these 34 patients had no calculi seen on 5-mm thick images, but at least one calculus was seen on the 0.625-mm images (Fig. 1). One additional case had two calculi seen on the 5-mm thick images. These calculi, however, were seen to actually represent a cluster of four smaller calculi on the 0.625-mm thick images (Fig. 2). In the 14 remaining patients in this group, 7 had unilateral renal calculi seen on 5-mm thick images, but bilateral renal calculi were identified on the 0.625-mm thick images, and 7 had only one calculus identified on 5-mm thick images but two or three calculi identified on the 0.625-mm images.
In the 15 patients in whom additional calculi were identified on the 0.625-mm thick images vs the 5-mm thick images but were not thought to be clinically significant, 14 had multiple calculi identified on the 5-mm thick images, and one or two additional calculi identified on the 0.625-mm thick images. One patient in this category had a number of calculi identified on the 5-mm thick images and an additional 2-mm calculus in the urinary bladder identified on the 0.625-mm thick images.
Discussion
As previously reported by Memarsadeghi and associates, 3 small stones (<3 mm) may be missed at a CT slice thickness of 5 mm but detected at smaller section widths. With the advent of MDCT, the ability to generate thinner slices such as 2.5 mm is very convenient. The use of 5-mm thick images, however, is still fairly common practice in evaluating the abdomen. In this article, we confirm the findings by Memarsadeghi and associates 3 and also look at the potential significance of detecting these additional small stones. In this study, all additional calculi that were identified on the 0.625-mm thick images were on the order of 1 to 2 mm. In many of the cases in this study where additional calculi were detected, these additional small calculi may not have been responsible for the presenting symptoms, such as hematuria or colic. The potential significance of detecting these additional small calculi, however, comes from the effect these additional calculi have on the workup, subsequent treatment, and follow-up in these patients. In this study, potentially clinically significant stones were identified in a number of particular situations:
(1) Patients with hyperparathyroidism are evaluated for end-organ effects of hypercalcemia. Hyperparathyroid patients who are otherwise asymptomatic but do have renal calculi will typically have neck dissections to explore for parathyroid adenomas. The two patients in this study with hyperparathyroidism had renal calculi detected on the 0.625-mm thick images. These same patients would have been falsely classified as being free of renal calculi if the 5-mm thick images alone were reviewed. 6,7
(2) Identifying the presence of calculi in a patient with hematuria may be of critical importance, because the index of suspicion regarding etiology of the hematuria may be altered with the discovery of additional small stones. 8 The greater sensitivity of the 0.625-mm thick images, with respect to finding these small calculi, may thus provide a more definitive diagnosis in the radiologic evaluation of patients with hematuria. 8
(3) In another example of clinically significant additional stones, current urologic practice recommends metabolic evaluation in several different clinical scenarios. One indication for performing such a workup is the presence of multiple, or bilateral, stones, because this finding suggests a higher risk for metabolic abnormality. 8 –13 In addition, it is important to delineate these small calculi so that in the case of follow-up scans, they are not misinterpreted as newly developed stones. Patients classified as recurrent stone formers may need more aggressive workup and treatment. 10 –13
(4) Finally, the better resolution of 0.625-mm thick slices can more accurately define stone burden, as seen in one patient in this study. The four tiny calculi on the thin-slice CT may present a treating urologist with different indications to observe and follow these stones because of the high probability of spontaneous passage, while the thicker (5-mm) CT slices suggested stones in a size range where treatment may be recommended because of a lower chance of spontaneous passage. 14 –17
There are limitations to this study. Because of the nature of the study, there is no gold standard. In theory, some of these additional tiny calculi identified may have been false positives representing artifact or vascular calcifications. The assumption is made that finding additional 1- to 2-mm calculi in some clinical scenarios, such as otherwise asymptomatic hyperparathyroidism, will imply the same clinical consideration that larger stones (that would be seen on 5-mm thick slices) would have in patient treatment. This article presents theoretical advantages for detecting these additional tiny stones. The actual significance of detecting these tiny calculi remains unknown but is an area for further research.
Conclusions
The results from this study encourage reviewing the thin slice source images of MDCTs in patients at risk for urinary calculi, as important clinical decisions may hinge on knowing that stones are present in a patient with hematuria, or that a metabolic evaluation is needed to reduce the risks of progression and recurrence. In reality, we do not know the actual significance of detecting these additional tiny stones. This is a topic for further research. In addition, the optimal slice thickness for evaluating patients at risk for urinary calculi is still to be determined.
Footnotes
Disclosure Statement
Dr. Berkenblit is a lecturer for Novartis. For the remaining authors, no competing financial interests exist.