
Abstract
Robot-assisted partial nephrectomy (RAPN) has been established as a viable alternative to open and laparoscopic partial nephrectomy for small renal tumors. Multiple variations in surgical technique have been described to reduce warm ischemia time (WIT). We present our off-clamp technique for RAPN. From August 2007 to January 2012, off-clamp RAPN was performed on 47 tumors in 39 patients. WIT was 0 minutes in all cases. The mean operative time was 147 minutes (SD=58); the mean and median estimated blood loss were 219 mL (SD=253) and 150 mL (range 50–1500), respectively; the mean length of stay was 1.9 days (SD=1.1). There were no intraoperative complications, and results for all surgical margins were negative. In experienced hands, our off-clamp technique for RAPN is a safe and feasible technique that eliminates WIT.
Introduction
Recognizing the potential renal parenchymal damage that can result from even limited ischemia, multiple variations in surgical technique aimed at reducing or eliminating warm ischemia time (WIT) have been described. 9,10 Such techniques can present technical challenges necessitating meticulous dissection of the renal vasculature. 11 More recently, techniques with no clamping of the renal hilum have been performed in a limited number of carefully selected patients. 12,13 In this article and supplementary video,* we demonstrate our off-clamp technique for RAPN, which has been performed in 39 patients from August 2007 to the present.
Technique
(1) Bowel preparation: Patients are placed on a clear fluid diet the day before surgery.
(2) Patient positioning: Patients are positioned in a flank position with pressure points padded with pillows and foam pads. The table is slightly flexed, and the patient is secured to the table with cloth tape.
(3) Trocar position: A Veress needle is placed in the lower quadrant and is used to establish pneumoperitoneum. Abdominal access is established by placing a 12-mm trocar at the umbilicus (camera port), and the abdomen is inspected. Two 8-mm robotic trocars are placed in the midclavicular line—one in the subcostal area and the other in the lower quadrant. If a four-arm approach is used, such as in taller patients or in cases of difficult dissection because of redundant perinephric fat, the third 8-mm robotic trocar is placed lateral to the midclavicular line between the umbilicus and the costal margin. A 12-mm trocar assistant port is placed in the midline above the umbilicus. In obese patients, trocar positions are shifted laterally. A 5-mm trocar for liver retraction in right-sided tumors is rarely necessary (Fig. 1).
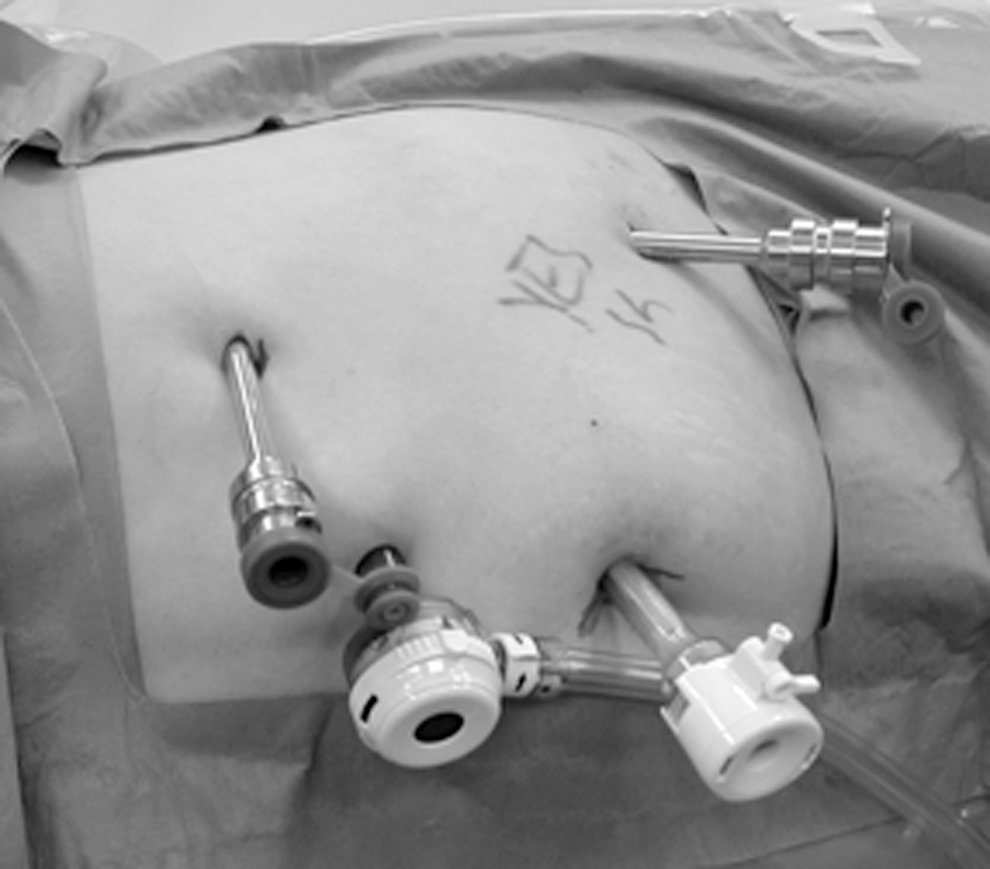
Trocar placement. A 12-mm trocar is placed above the umbilicus. Two 8-mm robotic working ports are placed—one medial to the anterior superior iliac spine and one below the costal margin in the midclavicular line. A 12-mm assistant port is placed in the upper abdomen at the midline. (For right-sided cases, an additional 5-mm trocar can be placed for liver retraction.)
(4) The robot is brought in and docked at a 30- to 45-degree angle toward the patient's head.
(5) Renal hilar exposure: Using a 30-degree downward lens, the colon is reflected medially away from the anterior aspect of the Gerota fascia. The gonadal vein and ureter are identified, and the gonadal vein is followed up to the renal hilum. The renal vessels are exposed and dissected free, which allows rapid application of robotic bulldog clamps if bleeding should preclude safe off-clamp tumor excision.
(6) The kidney is mobilized and the Gerota fascia is incised. The perinephric fat is dissected away from the renal capsule to expose the tumor. Peritumoral fat is preserved for pathologic examination. Intraoperative ultrasonography is used to demarcate tumor margins. It is crucial for the surgeon to have a clear notion of tumor dimensions to avoid a positive surgical margin.
(7) Intravenous mannitol (12.5 g,) is administered by the anesthesiologist. Two robotic bulldog clamps are introduced to allow for expeditious clamping of the hilum, if necessary. This allows the surgeon to respond quickly to bleeding that cannot be controlled with an off-clamp approach and is especially important early in the experience with this approach.
The margins of the mass are outlined circumferentially with monopolar electrocautery on the robotic scissors. This cautery is continued until an appropriate plane of dissection is found. The ProGrasp forceps (in the second robotic arm) are used to bluntly separate the tumor from the residual renal parenchyma with intervening tissue cauterized meticulously with the monopolar scissors. If a large vessel from the renal parenchyma is noted to be bleeding during tumor excision, the robotic bulldogs can be applied to the vessel in the resection bed. This controls the bleeding vessel(s) until suture ligation or clip application of the vessel(s) can be performed. In addition, larger vessels that are directly supplying the tumor can be controlled with Hem-o-lok clips (Teleflex Medical, Research Triangle Park, NC) if hemostasis with cautery is not adequate.
Mobilization of the tumor is continued circumferentially until complete excision of the tumor is achieved (supplementary video*). The bedside assistant uses suction and applies countertraction as necessary during tumor excision. The specimen is then placed above the liver or spleen for later retrieval.
(8) The base of the resection bed is cauterized. The insufflation pressure of the pneumoperitoneum is decreased to 5 mm Hg, and the resection bed is examined for any ongoing bleeding.
(9) A running 2-0 Vicryl on an SH needle (Ethicon Inc, Johnson & Johnson, Somerville, NJ) is used to oversew any patent venous sinuses or arteries at the base of the resection. If the collecting system has been entered, it is similarly closed. The defect in the renal parenchyma is closed using a sliding clip renorrhaphy technique 14 with interrupted 0 Vicryl sutures, Hem-o-lok clips, and Lapry-Ty suture clips (Ethicon Endosurgery, Cincinnati, OH). Gerota; fascia is then similarly reapproximated.
(10) The specimen is entrapped in a 10-mm specimen bag and then the robot is undocked. The specimen is removed through the 12-mm umbilical port with extension of the incision as necessary.
(11) The fascia for the 12-mm ports is closed with one Vicryl suture. The skin is reapproximated with a subcuticular absorbable 4-0 monofilament suture.
Equipment
• da Vinci® Surgical System Si HD (Intuitive Surgical Inc, Sunnyvale, CA)
• ProGrasp™ forceps, curved scissors, and large needle drivers (Intuitive Surgical Inc, Sunnyvale, CA)
• Laparoscopic 0- and 30-degree lens and da Vinci 0-degree lens (Intuitive Surgical Inc, Sunnyvale, CA)
• Two 12-mm trocars
• Two or three 8-mm robotic trocars and one 5-mm trocar (right side) for liver retraction (rarely used)
• Laparoscopic suction-irrigator
• Laparoscopic scissors for assistant
• Flexible laparoscopic ultrasound transducer or robotically-controlled ultrasound transducer (Hitachi Aloka Medical Ltd., Wallingford, CT)
• Two long, straight (25 mm) robotic bulldog clamps (Scanlan International Inc, St. Paul, MN)
• Sutures: 2-0 Vicryl™ suture (SH needle) for deep repair of renal defect, 0 Vicryl (CT-1 needle) for renorrhaphy and reapproximation of Gerota fascia (Ethicon Inc, Johnson & Johnson, Somerville, NJ)
• Hem-o-lok® Clips (Teleflex Medical, Research Triangle Park, NC), Lapry-Ty suture clips (Ethicon Endosurgery, Cincinnati, OH) and clip appliers
• Endoscopic specimen bag, 10 mm
Role in Urologic Practice
Our off-clamp technique has been used successfully for 47 tumors in 39 patients. Mean age in our series was 59.4 years. The mean tumor size was 2.8 cm, and mean nephrometry score was 6.2. No patients in this series had any WIT or intraoperative complications. Importantly, there were no conversions to an open approach or radical nephrectomy (Table 1). Pathology results in our series revealed malignancy in 79% of the patients and no positive surgical margins, demonstrating good oncologic control. This technique was safe and feasible in this group of patients. Notably, we started using our off-clamp technique for RAPN after previous experience with other robotic and laparoscopic procedures (including >100 conventional RAPN and >100 robot-assisted laparoscopic prostatectomies).
SD=standard deviation; ASA=American Society of Anesthesiologists; CCI=Charlson Comorbidity Index; eGFR=estimated glomerular filtration rate; EBL=estimated blood loss; RCC=renal-cell carcinoma.
The negative impact of prolonged WIT has been well established. The upper limit for a safe duration of WIT that allows for renal recovery postoperatively was previously held to be 30 minutes. 7 More recently, this upper cutoff for a safe duration of WIT has been defined as 20 minutes. 8,15 Other authors have found that every additional minute of WIT is associated with increased odds of acute renal failure and chronic kidney disease postoperatively. 16
As such, we sought to develop a technique with an aim to safely eliminate WIT in patients undergoing nephron-sparing surgery. This technique allows hemostasis to be achieved in “real time,” because any bleeding vessels can be fulgurated with monopolar cautery or be clipped during tumor excision, thus avoiding problems with significant bleeding on unclamping of hilar vessels, as can be seen with conventional RAPN. Our technique also precludes a potentially challenging dissection of renal microvaculature, 11 as may be necessary with other approaches for minimizing WIT. In addition, because our off-clamp technique does not necessitate controlled hypotension during tumor excision, as has been previously described, we feel that our technique minimizes risk to patients with cardiac comorbidities. 17 Lastly, our technique also can be applied in cases of challenging hilar or multifocal tumors (supplementary video*).
There are current limitations to our off-clamp technique. As with conventional RAPN, an experienced bedside assistant is necessary for successful completion of this surgery. The assistant allows adequate visualization of the surgical site and assists with traction/countertraction. In addition, in the case of hemorrhage during tumor excision, the assistant is needed to expeditiously apply laparoscopic bulldog clamps, although the recent introduction of robotic bulldog clamps may decrease reliance on the bedside assistant in this regard.
Lastly, our off-clamp technique requires surgeons to have previous experience with robot-assisted surgery in order to be performed safely. Implicit in this concern is the concept of appropriate tumor selection, which is especially relevant early in the experience with off-clamp RAPN. Our series included 39 patients who underwent off-clamp RAPN over 5 years. During this time frame, the surgeons involved in this series have performed approximately 500 RAPNs. With increased experience, however, our off-clamp technique is applied much more liberally to even complex renal masses, including those that are endophytic, hilar, and in close proximity to the collecting system. Our increasing experience with off-clamp RAPN has resulted in us initiating a prospective, randomized study comparing off-clamp with conventional RAPN at our institution.
Conclusion
Our off-clamp technique is safe and reproducible in the hands of experienced surgeons. We think that this technique can be quickly learned and implemented by surgeons with previous robotic experience. This technique allows for tumor excision with good oncologic control and no WIT.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.