
Abstract
Purpose:
This study evaluates the safety and efficacy of intravesical ropivacaine as part of a mulitimodal approach to the provision of analgesia after robot-assisted radical prostatectomy (RARP).
Patients and Methods:
In this double-blind, placebo-controlled trial, 40 patients who were scheduled to undergo RARP for treatment of localized prostate cancer by a single surgeon (SP) were randomized 1:1 to receive either alkalinized intravesical ropivacaine or placebo (0.9% sodium chloride) at the completion of the vesicourethral anastomosis. A standardized general anesthetic was administered in each case. The primary outcome was a reduction in postoperative pain as assessed by a visual analogue scale (VAS). The need for alternate analgesic agents was recorded. Adverse events related to the administration of intravesical ropivacaine were documented prospectively.
Results:
No serious adverse events related to the administration of intravesical ropivacaine were identified. In the ropivacaine group, there was a significant reduction in the cumulative needed dose of ketoralac relative to placebo at 6 hours postoperatively. There was no statistically significant difference between the groups with regard to pain scores or narcotic use at any time point.
Conclusions:
Intravesical administration of ropivacaine may be used safely in the context of RARP and is associated with a significant, albeit modest reduction in the need for supplementary analgesic agents, but did not result in a decrease in postoperative pain scores.
Introduction
The safety and efficacy of intravesical local anesthetic agents has been described in a urologic context in the treatment of patients with interstitial cystitis, bladder spasms, and symptoms related to ureteral stents. 6 –9 In light of these findings, we designed this study to evaluate the role for intravesical local anesthetic agents after RARP. To our knowledge, intravesical local anesthetic use as a means of analgesia postradical prostatectomy has not previously been described.
Patients and Methods
Study design
Eligible men who were scheduled for RARP at our center were offered the opportunity to participate in this randomized, double-blind, placebo-controlled study. The study protocol was approved by The University of Western Ontario Health Sciences Research Ethics Board (Review #17444). A no objection letter was issued by Health Canada given the off-label use of ropivacaine in this study.
Eligibility criteria are outlined in Table 1. All eligible patients were randomized by a computer generated schedule (Research Randomizer,
RARP=robot-assisted radical prostatectomy.
It was calculated that a sample size of 20 patients per group would have 80% power to detect a 25% difference in postoperative pain scores between groups using a two-sided alpha=0.05.
Data collection
Demographic data were collected preoperatively. A list of prescribed and over-the-counter medications as well as preoperative oncologic parameters were recorded prospectively. Patients were familiarized with a 10 cm VAS on which 0 represented no pain and 10 represented severe pain to facilitate its use in the immediate postoperative period.
After RARP, patients were assessed hourly for 6 hours and once again at 24 hours. Pain was assessed using a 10 cm VAS. Cumulative doses of analgesic agents were documented on standardized data collection forms. Narcotic requirements were converted to morphine equivalents to facilitate statistical analysis. All patients were reviewed at the time of urinary catheter removal 14 days after surgery, and adverse events since discharge were documented.
Surgical procedure
Patients undergoing RARP were administered a standardized general anesthetic consisting of induction and intubation with propofol 1 to 2 mg/kg and rocuronium 0.6 mg/kg. Anesthesia was maintained with oxygen, air, and sevoflurane or desflurane to maintain a minimum alveolar concentration of 1 to 1.2. RARP was performed via a transperitoneal antegrade approach with early division of the bladder neck. A bilateral pelvic lymph node dissection was performed for all patients, except those with low-risk disease as defined by the D'Amico criteria. 10,11 Patients with high-risk disease as defined by the D'Amico criteria or with gland volumes in excess of 150 cm3 are not routinely offered RARP at our center.
At the completion of the vesicourethral anastomosis, a 20F urinary catheter was placed. The catheter was irrigated while visualizing the anastomosis to exclude the presence of an anastomotic leak. Syringes containing the intravesical agents were prepared by a clinical trials pharmacist according to the study protocol. In each case, the contents of three separate syringes (20 mL 1% ropivacaine/placebo, 0.75 mL 8.4% 1:20 sodium bicarbonate, 5 mL 0.9% saline) were instilled sequentially through the catheter. The 5 mL 0.9% saline flush was used to evacuate the small volume of solution remaining in the catheter lumen after instillation to ensure complete and consistent administration. A catheter plug was placed, and the patient was transferred to the operating room recovery area. After 1 hour, the catheter plug was removed.
Statistical analysis
Statistical analysis was performed by a statistician independent of the study protocol using Statistical Package for the Social Sciences version 20 (IBM Corporation, Armonk, NY). Demographic and preoperative oncologic variables were subjected to direct comparison using mean for continuous variables. Differences in mean pain score and analgesic use were evaluated with unpaired two-tailed Student t tests. Significance was assessed at the P<0.05 level.
Results
Fifty-one consecutive patients presented for RARP at our institution between May 2011 and March 2012. After prescreening, eight patients were deemed ineligible based on the predefined exclusion criteria (Table 1), and one patient was withdrawn because of an intraoperative robotic malfunction early in the procedure, necessitating conversion to open retropubic prostatectomy, which was completed without complication. Two patients declined participation. Complete data for 40 patients were analyzed. The two cohorts were equivalent with regard to preoperative demographic and oncologic characteristics (Table 2). RARP was completed without intraoperative complications in all 40 patients. No anastomotic leaks were identified. All patients tolerated catheter clamping for 60 minutes postoperatively.
SD=standard deviation; PSA=prostate-specific antigen.
At 6 hours postoperatively, the cumulative required dose of ketorolac was significantly less in the treatment group (Table 3). There was a consistent trend toward less acetaminophen use at each time point beyond 3 hours, although this did not reach statistical significance (Table 4). Statistical analysis of the VAS pain scores (Fig. 1) revealed that intravesical ropivacaine did not result in a significant reduction in postoperative pain at any time in the early postoperative period. Likewise, no difference was seen regarding the required cumulative dose of morphine (Table 5).
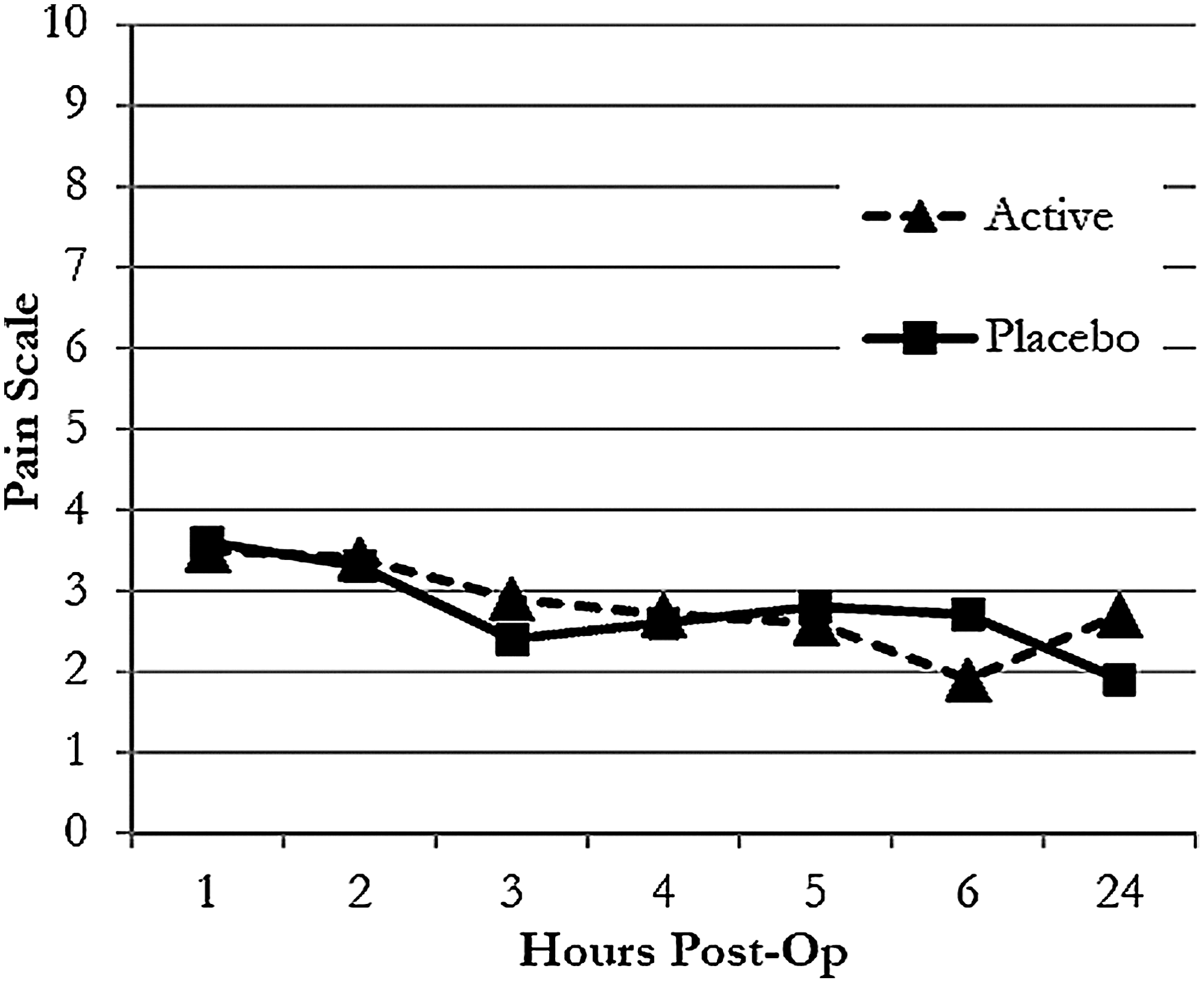
Mean pain scores. No significant difference was demonstrated at any time point.
Indicates significance at the P<0.05 level.
SD=standard deviation.
SD=standard deviation.
SD=standard deviation.
No serious inpatient or outpatient adverse events attributable to the intravesical administration of ropivacaine were identified during follow-up.
Discussion
The da Vinci Surgical System (Intuitive Surgical, Sunnyvale, CA) was approved by the United States Food and Drug Administration in 2000 and by Health Canada in 2003. When used to perform radical prostatectomy, this device is associated with a number of benefits including shorter duration of hospital stay and reduced blood loss. 1 Benefits in terms of postoperative pain for RARP compared with ORP remain less well defined, with inconsistent results in the published literature. 12,13
In designing this study, we hypothesized that the successful instillation of local anesthetic agents in the management of interstitial cystitis, painful bladder syndromes, ureteral stent symptoms, and after percutaneous nephrolithotomy may equally be applied after RARP. 6 –8,14 –16 Pain management after RARP has traditionally taken the form of agents such as ketorolac and acetaminophen supplemented with narcotics for breakthrough pain. 2,5
The adverse effects associated with opioid analgesic agents are well recognized and include nausea, vomiting, pruritus, impaired intestinal motility, respiratory depression, and altered sensorium. The administration of intravesical local anesthetic agents represents a potentially attractive option to augment other analgesic agents after surgery. These agents are inexpensive, safe, widely available, and easily administered. The rationale for this pilot study was to perform a properly designed trial to test the efficacy and safety of intravesical ropivacaine. Ropivacaine was selected because of its longer half life relative to lidocaine. Sodium bicarbonate (8.4%) was coadministered given the results of previous trials that have demonstrated improved bladder absorption of local anesthetic agents at higher urinary pH. 17,18 To our knowledge, this study is the first of its kind to evaluate intravesical ropivacaine in this context.
Although there was no statistically significant difference in pain score or narcotic use at any time point during the study, intravesical ropivacaine was associated with a significant reduction in the cumulative dose of ketorolac at 6 hours after surgery. In interpreting the results of this study, one should note that pain scores and analgesic requirements were low in both groups at all time points as one would expect given the minimally invasive nature of this surgery. Furthermore, although the benefits of intravesical ropivacaine appear modest, the use of this agent was not associated with any identifiable adverse event during follow-up. We therefore propose that this approach to analgesia warrants further evaluation in a larger study powered to detect small differences in analgesia requirements.
Despite a randomized, double-blind, placebo-controlled study design and standardized general anesthesia, we acknowledge several key limitations of this study. The number of patients in each group was relatively small, and it is likely that the study was underpowered to detect a difference between the groups regarding pain scores and narcotic use at the current sample size. Because there is limited experience with intravesical ropivacaine, the optimal dosing remains to be defined. We opted to administer a dose of 200 mg (20 mL of 1% ropivacaine) as per the manufacturer's recommended maximal dose for peripheral nerve blockade. Measurement of serial serum drug levels during the immediate postoperative period would have been useful to define the pharmacokinetics of this agent when administered intravesically and may well have justified the administration of higher doses. In addition, the optimal duration of administration to maximize absorption across the bladder mucosa remains poorly defined. The decision to drain the intravesical agent after 1 hour was made to reduce the likelihood of compromise to the anastomosis in association with acute urinary retention.
No restriction was placed on the postoperative administration of analgesic agents as deemed necessary by the nursing staff. It is possible that the type and dose of agent may have been influenced by differences in practice among staff. A more standardized, objective means of assessing narcotic requirements would be to have used patient-controlled analgesia for all patients, although this is not standard practice after RARP at most centers and was therefore not incorporated into the study protocol. 2
Conclusion
There is increasing recognition of the benefits associated with a structured, evidence-based approach to the treatment of patients after minimally invasive surgery. 3,4 The provision of effective, safe analgesia facilitates rapid discharge from hospital, with resultant benefits to the patient and the healthcare system. Although the analgesic effect of intravesical ropivacaine appears modest, we maintain that further research directed at optimizing pain control after robotic surgery is indicated based on the results of this trial.
Footnotes
Acknowledgment
Statistical advice was provided by Dr. Yves Bureau, Lawson Health Research Institute, London, Ontario, Canada.
Disclosure Statement
No competing financial interests exist.