
Abstract
Background and Purpose:
Ureteroneocystostomy can be used for the treatment of patients with a wide variety of ureteral pathology. Over the last decade, robot-assisted surgery has become more commonly used as a minimally invasive approach for reconstructive upper urinary tract procedures. The aim of this study is to present our experience with robot-assisted ureteroneocystosctomy (RUNC) with a comparison with that of open ureteroneocystostomy (OUNC).
Patients and Methods:
Medical records of 25 patients who underwent RUNC and 41 patients who underwent OUNC or at our institution between 2000 and 2010 were retrospectively analyzed. Perioperative and postoperative data including demographics, surgical outcomes, and clinical and radiographic findings at postoperative follow-up were considered in the comparative analysis. Descriptive statistics were used to present the data. The significance of the difference between variables was evaluated using the Wilcoxon rank sum test for continuous and Fisher exact test for categorical variables.
Results:
No significant differences were detected in terms of baseline patient characteristics between the two groups. The OUNC procedures were performed with a shorter median operative time (200 vs 279 min., P=0.0008), whereas RUNC patients had a shorter hospital stay (median 3 vs 5 days, P=0.0004), less narcotic pain requirement (morphine equivalent, mg 104.6 vs 290, P=0.0001), and less estimated blood loss (100 vs 150 mL, P=<0.0002). There as no significant difference in the rate of reoperation between groups: RUNC 2/25 (7.6 %) vs OUNC 4/41 (9.7%) P=0.8. Limitations include the retrospective nature of the study and the difference in indications for surgery.
Conclusion:
RUNC provides excellent outcomes with shorter hospital stay, less narcotic pain requirement, and decreased blood loss when compared with the open procedure. Advantages of the robotic platform for dissection and suturing can be useful for complex minimally invasive urologic reconstructive procedures.
Introduction
Despite longer operative times, laparoscopic UNC was performed with excellent outcomes and associated with less hospital stay and narcotic requirements compared with the open procedure. 6,7 Nevertheless, laparoscopic UNC is technically demanding and needs significant experience and skill. 6
The adoption of robot-assisted surgery allowed urologists to shorten the learning curve of 8 and facilitate suturing during laparoscopic reconstructive procedures. 9 Thus far, several robot-assisted UNC (RUNC) series have been reported. Indications for surgery covered a wide variety of ureteral diseases, including urothelial cancer, ureteral strictures after stones, iatrogenic injuries, endometriosis, and lymphoma. All these series confirmed the safety and efficacy of robot-assisted surgery for performing UNC. 3 –5,7,10 –13
The aim of this study is to describe in detail the surgical technique of RUNC at our institution, to report its outcomes, and to compare them to those of the open approach.
Patients and Methods
Study population
After obtaining Institutional Review Board approval, our institutional database was queried by using pertinent International Classification of Diseases-9 billing codes to retrieve the medical records of patients who had undergone UNC at our institution between 2000 and 2010.
Twenty-five patients who had undergone RUNC from 2007 to 2010 were identified and included in the analysis. Of 79 eligible patients who had undergone open UNC (OUNC) from 2000 to 2010, 41 were included for comparison to allow matched comparison based on the surgical technique used. Patients with bilateral ureteral reimplantation, procedure as part of other surgery, ureterectomy for treatment of urothelial tumor and vesicoureteral reflux, or incomplete charts were excluded from the study.
Baseline demographics, including age, body mass index (BMI), American Society of Anesthesiologists (ASA) score, previous surgery, laterality, and etiology of ureteral pathology were collected as well as peri- and postoperative data, including operative technique, operative time, estimated blood loss (EBL), intraoperative complications, length of hospital stay, narcotic requirements in morphine equivalents, postoperative glomerular filtration rate (GFR), postoperative complications, follow-up in months, and success based on radiographic and symptomatic factors.
RUNC: Surgical technique
The patient is placed in the lithotomy position in stirrups with all pressure points padded. The table is placed in the steep Trendelenberg position and tilted so that the ipsilateral side of the surgery is somewhat elevated. The camera port is placed about 4 to 5 cm cranial to the umbilicus, and the robotic ports are placed approximately 4 cm caudal and 9 to 10 cm lateral to the camera port. The ipsilateral robotic port is usually positioned slightly more cranial than the contralateral robotic port. The fourth robotic arm is not routinely used. A 12-mm assistant port is usually placed lateral to the right robotic port. The robot is usually docked at the base of the table, between the legs of the patient, similar to the configuration for robot-assisted prostatectomy.
The procedure is transperitoneal and begins with mobilization of the colon and identification of the ipsilateral ureter. In general, it is advisable to identify the ureter and begin dissection cranial to the area of pathology. Often, ureteral identification is more straightforward on the right side, because peristalsis may be noted deep to the undisturbed peritoneal layer. On the left, the sigmoid colon often obscures the location of the ureter and must be mobilized significantly before ureteral identification. In women, the ureter is identified medial to the ovary. The ureter is exposed and dissected free of the surrounding tissues, progressing distally until the site of the ureteral pathology is reached. The ureter is transected proximal to the site of pathology, which is noted by periureteral induration.
The ureter is spatulated and the bladder is mobilized. The bladder is filled with 300 to 400 mL of sterile saline and a 2 to 3 cm vesicotomy is performed posteriorly and on the ipsilateral side of the ureteral anastomosis. A tension-free refluxing anastomosis using interrupted 3-0 polyglactin sutures is performed. After three sutures are placed, a ureteral stent is passed through the assistant port over a guidewire, and the proximal end is fed up the ureter while the distal end is placed in the bladder. If the length of the ureteral stricture does not allow a tension-free direct anastomosis of the ureter to the urinary bladder, a vesicoileopsoas hitch technique with suture fixation of the urinary bladder to the tendon of the ipsilateral ileopsoas muscle 14,15 or a Boari flap is created to bridge the defect. 16,17 For the ileopsoas hitch, the bladder is sutured to the psoas muscle tendon using two sutures of 2-0 polydioxanone while making sure to preserve the genitofemoral nerve.
For longer gaps, a Boari flap procedure is selected by following the same principles of an open procedure. A wide base of the flap is used to maintain adequate blood supply (Fig. 1a). The ureter is anastomosed directly to the tip of the flap (Fig. 1b) followed by tubularization of the flap with successive interrupted sutures and a U-stitch (Figs. 1b, 1c). The remaining bladder defect is then sutured with 2-0 polyglactin suture in a running fashion. A J-P drain in placed alongside the anastomosis.
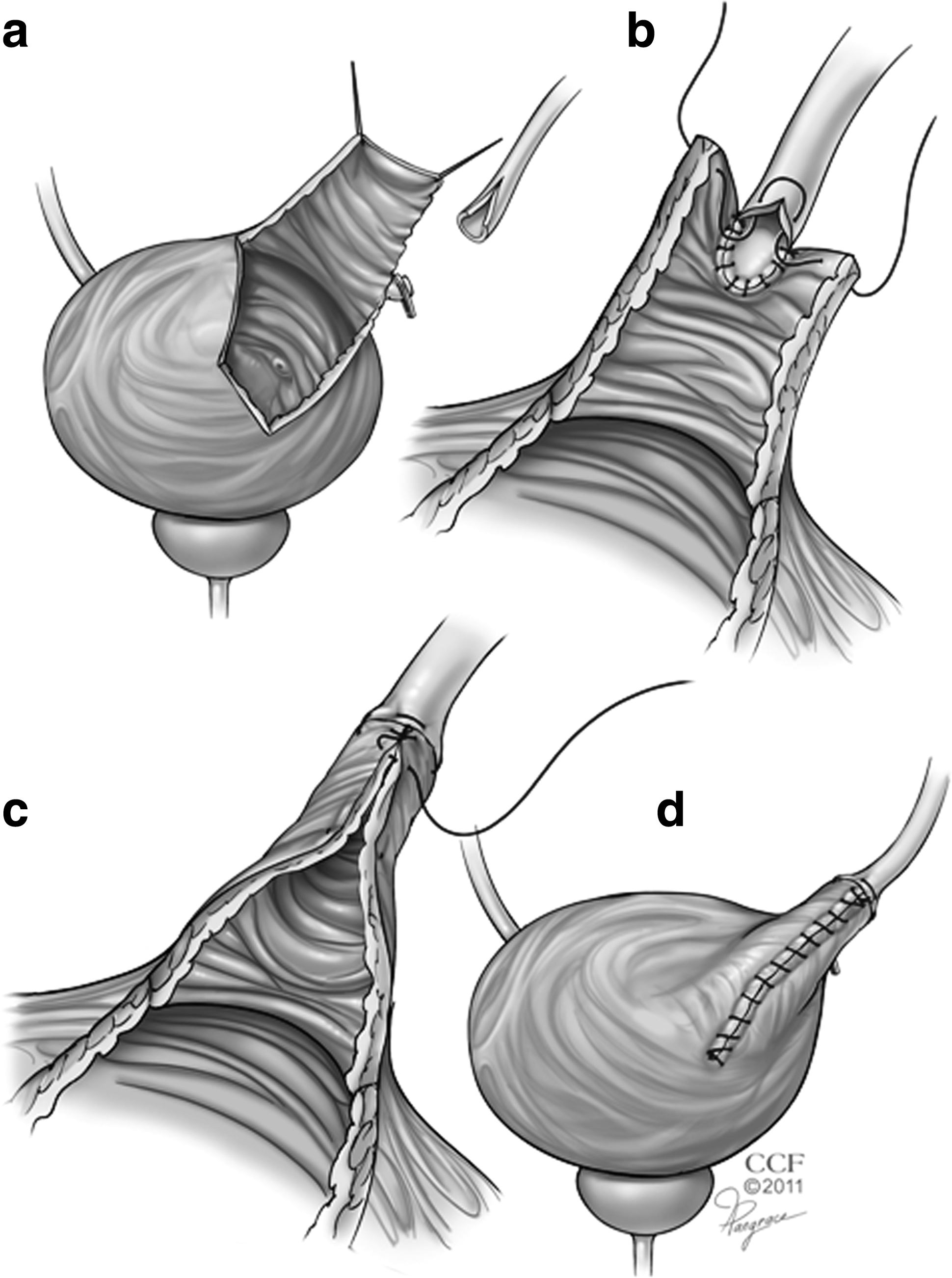
Creation of the Boari flap.
Postoperative management
If the J-P drainage is consistent with peritoneal fluid on serologic analysis, the J-P drain is removed on postoperative day 2. Cystography is performed 1 week after the procedure, and if no urinary extravasation is noted, the Foley catheter is removed. The ureteral stent is removed 4 weeks after surgery. Diuretic renography is performed 6 weeks after stent removal and repeated at 6 months. Narcotic requirement was calculated using a morphine equivalent calculator.
Renal function was assessed by estimating GFR using the Modification of Diet in Renal Disease study equation. 18 The postoperative complications were graded using the Clavien-Dindo classification. 19
Data analysis
The mean (standard deviation) or median (interquartile range) was calculated for variables. The Wilcoxon rank sum test was used for continuous and the Fisher exact test for categorical variables. P value was considered significant if P<0.05, using JMP® 9.0.0 (SAS Institute Corp.) software.
Results
Baseline characteristics
No difference was noted in terms of age, BMI, sex, ASA score, or laterality of pathology between the RUNC and OUNC groups (Table 1). For the robotic group, 16 patients had ureteral stricture after management of stone disease, 4 patients had ureteral obstruction secondary to endometriosis, and 5 patients had iatrogenic injury to the ureter. For the OUNC, 32 (78%) patients had ureteral stricture, while 9 (21%) had surgery to repair iatrogenic injury to the ureter. Forty-four percent had previous stone surgery in the robotic group compared with 14.6% in the OUNC group (P=0.09).
Values expressed as median (interquartile range) unless otherwise specified.
RUNC=robot-assisted ureteroneocystostom; OUNC=open ureteroneocystostomy; BMI=body mass index; ASA=American Society of Anesthesiologists.
Operative data
Forty percent of patients in the robotic group underwent primary UNC vs 46.3% in the OUNC group (Table 2). Forty percent of patients underwent UNC with a Boari flap (UNC-B) in the robotic group compared with 19% in the open group (P=0.1). Operative time was significantly longer in the robotic group (median 279 vs 200 min, P=0.0008), while EBL (100 vs 150 mL, P=0.0002) and change in hematocrit (−2.6 vs−5.6, P=0.02) were significantly less in the robotic group. No patient needed conversion either to an open or laparoscopic procedure.
Values expressed as median (interquartile range) unless otherwise specified.
Wilcoxon rank sum test for continuous and Fisher exact test for categorical variables.
RUNC=robot-assisted ureteroneocystostomy; OUNC=open ureteroneocystostomy; UNC=ureteroneocystostomy.
Postoperative data
Hospital stay was significantly shorter in the robotic compared with the OUNC group (median 3 vs 5 days, P=0.0004 [Table 3]). Postoperative pain medications as measured by morphine equivalents was significantly less for RUNC (median 104.6 mg vs 290 mg, P=0.0001).
Values expressed as median (Iinterquartile range) unless otherwise specified.
Wilcoxon rank sum test for continuous and chi square test for categorical variables.
RUNC=robot−assisted ureteroneocystostomy; OUNC=open ureteroneocystostomy; eGFR=estimated glomerular filtration rate.
Postoperative complications/failures
In the RUNC group
A 39-year-old woman underwent robot-assisted UNC-B for a ureteral stricture after numerous endoscopic procedures for stones. Two years later, after a bout of pyelonephritis but no direct endoscopic or radiographic evidence of restricture, the patient underwent open ureteral reimplantation with psoas hitch at an outside hospital. Pyelonephritis recurred, and she underwent open ileal interposition repair at the same institution (Clavien IIIb).
In the OUNC groups, a 44-year-old woman underwent OUNC for iatrogenic injury. After surgery, a colocutaneous fistula developed that was surgically repaired (Clavien IIIb).
A 54-year-old woman underwent ureteral reimplantation for ureteral stricture after multiple abdominal surgeries because of Crohn's disease. Recurrent stricture developed that failed endoscopic incision and needed repeated open UNC-B. Postoperatively, she also had a wound infection necessitating reopening of the wound.
A 51-year-old man had a history of multiple ureteral procedures as well as colon cancer for which he had undergone chemotherapy and radiation. Long segments of ureteral stricture developed for which he underwent ureteral reimplantation with a Boari flap. He had recurrent pain after his Boari flap procedure, and radiologic studies suggested obstruction. Despite offering the patient further treatment for his ureteral stricture disease, the patient decided to undergo nephrectomy (Clavien IVa).
An 87-year-old woman who underwent OUNC with psoas hitch for ureteral stricture needed blood transfusion (Clavien II).
Discussion
The use of robotic platforms for various urologic procedures is gaining ground. In this study, we present our experience with 25 patients who underwent robot-assisted ureteral reimplantation for ureteral obstruction because of a wide variety of pathologic processes.
This study aimed to present our single institution experience with robot-assisted ureteral reimplantation and to compare our outcomes with those of the open procedures. To the best of our knowledge, this represents the largest report of RUNC published to date.
There was no significant difference between groups regarding age, sex, BMI, ASA score, or laterality of pathology. The choice of surgery was based on the length of the ureteral defect after the ureter is transected. Forty percent of patients undergoing robot-assisted surgery had a Boari flap reconstruction compared with 19% of the open group. Although this difference did not reach statistical significance, this may, in part, account for the difference in operative times because Boari flap procedures are more complex.
We found a significant difference in terms of narcotic pain requirement (105 mg vs 290 mg) favoring the robotic approach. In the robotic group, pain control was managed with oral pain medications and intravenous narcotics for breakthrough pain. None of the patients within the robotic group needed epidural analgesia or narcotics through patient-controlled analgesia (PCA). For the open ureteroneocystostomy group, pain was controlled with epidural analgesia in eight (14%) patients, and otherwise pain was controlled in many with PCA narcotics. For the robotic group, the EBL was significantly less than in the OUNC group, although estimation of EBL admittedly may be inexact. A more objective comparison may be change in hematocrit, which was also significantly less for the RUNC group (P=0.02). None of the RUNC group needed blood transfusion, while one patient in the OUNC group received a blood transfusion postoperatively. Finally, RUNC patients had a shorter hospital stay at 3 days compared with 5 days with OUNC (P=0.0004).
Two patients of 25 undergoing RUNC needed eventual further reconstructive procedures: Autotransplantation in one and a psoas hitch followed by ileal interposition in the second at an outside institution. Review of the second case confirmed pyelonephritis, but with no obvious evidence of recurrent stricture before repeated reconstruction. Recurrent stricture disease developed in two patients undergoing OUNC leading to UNC-B in the first and nephrectomy in the second. Wound complications were more common in the open series, including one wound infection, one dehiscence, and one cutaneous fistula.
Recently, several groups presented their series for RUNC. 10,11,20 In their data, the authors have shown that RUNC can be performed with excellent success rates (Table 4). Our series had comparable results to these previously published studies in terms of low EBL, LOS usually 4 days or less, and rare complications. Operative time in our study was among the highest of published series, but once again this could be associated with the higher complexity of strictures as evidenced by the large number of Boari flap procedures for our patients.
EBL=estimated blood loss; LOS=length of stay; UNC=ureteroneocystostomy.
One study compared outcomes of 10 RUNC with 10 OUNC for strictures secondary to stone disease or iatrogenic injury. EBL and hospital stay were less in the robot-assisted surgery patients compared with the open group. The robot-assisted surgeries had a longer operative time, and patients needed less narcotics, although these differences did not reach statistical significance. 21
Limitations of this study include its retrospective nature. There was also no pain scale used to evaluate postoperative pain. Although most of our patients in the robotic group had pre- and postoperative evaluation of kidney obstruction using diuretic renal scan, these studies were not available for most in the OUNC group.
Conclusion
RUNC represents a safe and effective procedure for the surgical treatment of distal ureteral pathology. The robotic approach demonstrates significant advantages regarding lower postoperative narcotic requirements, shorter hospital stay, and decreased blood loss compared with the open procedure.
Footnotes
Disclosure Statement
Dr. Kaouk is a speaker for Intuitive and a consultant for Covidien. Dr. Haber is a speaker for Intuitive Surgical. For the remaining authors, no competing financial interests exist.