
Abstract
Background and Purpose:
The discovery of thick, adherent, perinephric sticky fat (PSF) is relatively common during open or laparoscopic retroperitoneal surgery. To our knowledge, however, there has been no previous analysis of clinical or radiographic features associated with the development of PSF or of perioperative outcomes for those patients in whom it is found. Our objective is to analyze potential predictive features and determine whether there is any effect on clinical or pathologic outcomes for patients with perinephric sticky fat.
Patients and Methods:
Patients undergoing partial nephrectomy or laparoscopic cryoablation with available preoperative imaging were identified from 2005 to 2011. Operative records were reviewed to identify patients with and without PSF. Preoperative images and medical records were examined to obtain patient data regarding potential predictors as well as clinical and pathologic outcomes.
Results:
A total of 29 patients were identified—16 with PSF and 13 controls. Statistically significant factors associated with PSF included sex, tumor size, presence of perinephric stranding, tumor >50% exophytic, and thickness of perinephric fat (P<0.05). Median total operative time for patients with sticky fat was nearly 40 minutes longer than the control group (228 min vs 190 min, P<0.05). All four (17%) patients with Fuhrman grade 3 or 4 renal-cell carcinoma were from the sticky fat group (P=0.09).
Conclusions:
Despite the small sample size, multiple possible factors associated with perinephric sticky fat were identified and may provide guidance for future investigation of this phenomenon.
Introduction
Patients and Methods
After Institutional Review Board approval, patients were identified who had undergone open or minimally invasive partial nephrectomy or laparoscopic cryoablation between June 2005 and December 2011 and also had available preoperative cross-sectional imaging. Operative records for these patients were then reviewed to identify patients for whom the surgeon had specifically noted the presence or absence of “sticky fat.” Patients for whom the perinephric fat was described as “dense,” “adherent,” “sticky” or similar terms were classified in the PSF group, while those for whom the description included “not adherent,” “easily dissected,” or “not sticky” were classified in the control group. Patients with no specific mention of the perinephric fat were excluded. Preoperative imaging and medical records were then reviewed to obtain the relevant data for patients in the two groups.
Demographic information and clinical parameters proposed to be potentially associated with PSF were identified from the medical record. These included age at the time of surgery, sex, and body mass index (BMI), as well as medical treatment for hypertension, history of smoking, history of chronic kidney disease (defined as baseline estimated glomerular filtration rate [eGFR] <60 mL/min/1.73m2), and previous ipsilateral retroperitoneal surgery.
Preoperative CT scan closest to the date of intervention was used preferentially; MRI was used when no CT imaging was available. From the images, tumor size and location (upper, mid, or lower) were recorded, as well as the R.E.N.A.L. (radius; exophytic/endophytic; nearness; anterior/posterior; location) nephrometry score. 1 Thickness of perinephric fat was determined by measuring posteriorly from the kidney to the posterior abdominal wall at the level of the renal artery. Mean Hounsfield units (HU) of the perinephric and subcutaneous fat were recorded at the same level for the patients with CT images (Fig. 1). Presence or absence of perinephric stranding, renal cysts, and discernible Gerota fascia were also noted for each patient.
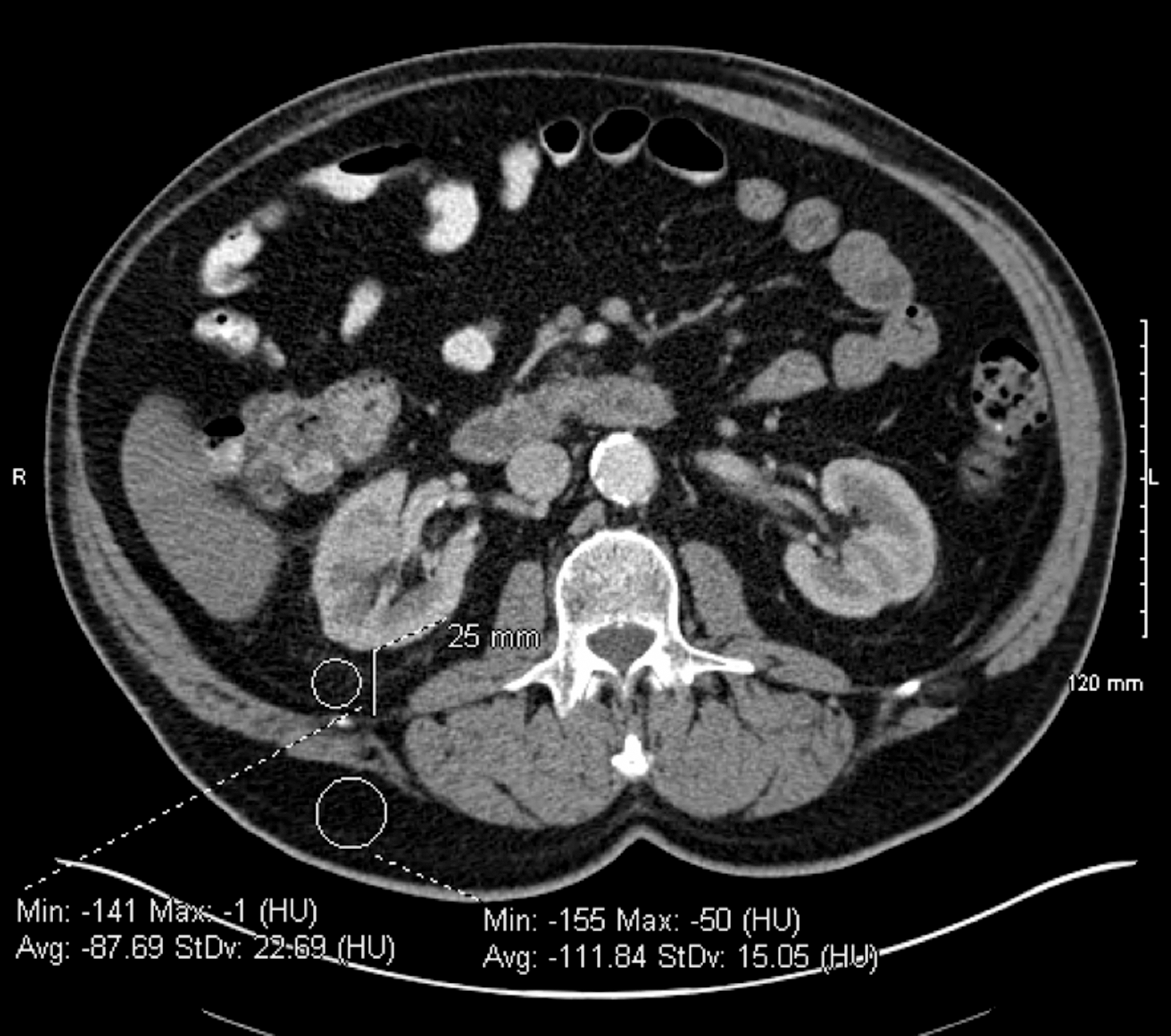
70-year-old man with 3.8-cm right upper pole renal tumor found to have perinephric stranding, perinephric fat thickness of 25 mm, mean perinephric fat Hounsfield unit (HU) of -88, and mean subcutaneous fat HU of -112.
Perioperative details were obtained from the operative records for comparison between PSF and control groups. These included type of intervention, total operative time, ischemia time, estimated blood loss (EBL), hospital stay in days, and occurrence of postoperative urine leak or need for transfusion. Baseline eGFR was calculated using the latest preoperative serum creatinine level and the Modification of Diet in Renal Disease equation. 2 Postoperative eGFR was calculated using the nadir serum creatinine level from 1 to 6 months after surgery whenever available, and in the immediate postoperative period otherwise. Percent change in eGFR was then calculated for each patient. Pathologic data were also reviewed to classify the tumors as malignant or benign and to record Fuhrman grade for those with renal-cell carcinoma.
Group comparisons were made using the Mann-Whitney U test for continuous variables and the Fisher exact test for categorical variable. Significance level was set at P<0.05. All statistical analyses were performed using SAS 9.2.
Results
A total of 29 patients were identified who met the inclusion criteria. Of these, 16 were categorized in the PSF group based on the description by the operating surgeon. Representative descriptions included: “The perinephric fat was densely adherent and was difficult to remove,” and “The fat was extremely adherent to the capsule of the kidney and was extremely difficult to dissect.” Thirteen patients were identified for the control group, based on operative descriptions such as: “The fat was not adherent to the kidney at all,” and “The dissection plane here was not difficult. There was no evidence of sticky fat.”
Table 1 shows the demographic and clinical characteristics for the two groups. The majority (75.8%) of the patients were male, and the overall median age was 58.6 years (interquartile range [IQR] 51.0, 70.0). Twenty-six of the patitents had available CT imaging; the remaining 3 had only MRI preoperatively. The median BMI for the group was 31.2 kg/m2 (IQR 28.0, 34.4), and only three patients had a BMI of less than 25. The median tumor size was 2.8 cm (IQR 2.4, 4.0). All but three patients underwent partial nephrectomy; the remainder were treated with laparoscopic cryoablation.
n=12 for control group.
n=12 for control group, n=15 for sticky group.
Median (Interquartile range) shown for continuous variables.
BMI=body mass index; CKD=chronic kidney disease; eGFR=estimated glomerular filtration rate.
The PSF group had a median age more than 8 years older than the control group (63.2 years vs 55.1 years), a difference that approached statistical significance (P=0.06). Fifteen of the 16 (94%) patients with sticky fat were men, compared to only 54% of the control group (P<0.05). The remainder of the baseline factors were similar between the two groups.
Summary of the radiographic features of the two groups is found in Table 2. Increasing tumor size, presence of perinephric stranding on CT, and greater than 50% of the tumor exophytic were all radiographic features that showed a statistically significant association with presence of PSF. Neither polar location nor any of the described scoring systems demonstrated a relationship, however. There was no significant difference in the HU of the perinephric fat in the two groups, nor was there a relative difference when compared with subcutaneous fat. Although BMI was not associated with the presence of PSF, thickness of the perinephric fat was clearly different between the two groups, with the median thickness of the sticky fat group over three times that of the control group (36.5 mm vs 12 mm). Neither presence of benign cysts nor visible Gerots fascia was associated with PSF.
Median (IQR) shown for continuous variables.
n=12 for nonsticky fat, n=15 for sticky fat.
CT=computed tomography; HU=Hounsfield units.
Overall, the outcomes after partial nephrectomy for the patients in the PSF group were similar to those of the control group, although there were some important differences (Table 3). Most notably, the patients in whom PSF was encountered were in the operating room significantly longer, with a median operative time of 228 minutes compared with 190 minutes for the control. The other perioperative parameters examined (ischemia time, blood loss, hospital stay, renal function outcomes) were not significantly different among the two groups. The PSF group did include two patients who needed blood transfusion perioperatively and one patient who had a postoperative urine leak, while the control group did not have any such events. In this small sample, however, these differences did not reach statistical significance.
Median (IQR) shown for continuous variables.
n=11 for nonsticky, n=12 for sticky group.
OR=operative; EBL=estimated blood loos; eGFR=estimated glomerular filtration rate
Only four patients in the total sample had Fuhrman grade 3 or 4 renal -ell carcinoma, but all four were from the PSF group. The rate of malignancy at final pathology determination was not statistically different between the groups, with both groups primarily composed of renal-cell carcinoma. The difference in higher grade disease, however, did approach statistical significance (P=0.09) despite the small sample size.
Discussion
The underlying physiology associated with the development of thick, adherent PSF is unclear, although there are several possible factors, including inflammation, desmoplasia, idiopathic fibrosis, or autoimmune response. The strong association of perinephric stranding with sticky perinephric fat may suggest that inflammation is the underlying process, because similar findings are encountered in other conditions that provoke an inflammatory response, such as pyelonephritis and ureteral obstruction. Increasing understanding of the role of adipose tissue in inflammation may also support this possibility. For example, in Crohn disease, “thickened and stiff” mesenteric adipose tissue associated with increased local inflammatory mediators and fibrosis often develops. 3
Fibrosis as a desmoplastic response is seen in the setting of other malignancies. One of the hallmarks of small bowel carcinoid tumors, for example, is the occurrence of fibrosis both locally and distant from the primary tumor, including in the retroperitoneum. 4,5 The etiology in these cases is thought to be mediated by serotonin, and treatment with somatostatin analogs may contribute to reduced fibrosis in some patients. 4 In a review of CT findings in 31 such patients, Druce and associates 4 noted the presence of soft tissue stranding in 76% of the patients with a visible mesenteric mass. Thirteen of 15 (86.7%) PSF patients with CT scans in our sample had perinephric stranding on preoperative imaging, compared with only 2 of 12 (16.7%) who did not (P<0.001). We anticipated that there would also be a discernible difference in the HU of the perinephric fat between the groups, but no absolute or relative differences were seen.
Increasing BMI was not associated with the presence of sticky fat in our series, but thickness of perinephric fat was. In a review of outcomes of 349 patients undergoing major hepatectomy, Morris and colleagues 6 found that amount of “intra-abdominal fat”—determined by thickness of perinephric fat—was associated with mortality, complications, and length of stay, while BMI and “outer abdominal fat” were not. Furthermore, in their series, the correlation between BMI and amount of intra-abdominal fat was quite weak, suggesting that there may be underlying biologic differences in these patients. Although differences in complications between the groups in our series were not statistically significant, both patients who needed transfusion and the patient who had a postoperative urine leak all had sticky fat, and patients from the PSF group did have longer operative times.
In recent years, there has been increasing evidence to guide the surgeon in the management of the small renal mass. Options for these patients include active surveillance, radical or partial nephrectomy, and thermal ablation. The American Urological Association (AUA) guideline for the treatment of small renal masses emphasizes the importance of nephron-sparing, but concedes that there is still uncertainty about selecting the “ideal” treatment for a given patient. 7 Unfortunately, situations often arise where, based on patient age, preference, comorbidities, or other factors, the optimal approach is not clear. While we do not suggest that our findings are likely to drive the decision process in general, a clearer understanding of the predictors of sticky fat, and the consequences of encountering it, may add to the pool of data that surgeons use in counseling their patients.
For example, a patient similar to Index Patient #2 in the AUA guideline, 7 with a small mass but multiple comorbidities, who is an older man with obvious perinephric stranding and thick perinephric fat on CT scan, could be counseled that the presence of sticky fat could prolong the procedure and be associated with higher rates of anesthetic or postoperative complications, suggesting laparoscopic ablation or surveillance as a more palatable approach. On the other hand, if we were to determine that the presence of PSF was indeed associated with higher-grade disease, a more aggressive approach to the mass might be warranted. For those less comfortable with minimally invasive partial nephrectomy, findings suggestive of PSF might lead to the decision to proceed with an open approach. 8
While our findings may be of interest to those who have encountered PSF and questioned its origin and significance, their clinical significance is unclear at this point. Clearly, there are many weaknesses to our investigation. First of all, the selection of the patients, and the small sample, invites the introduction of unforeseen bias. The categorization of the patients is entirely subjective and based on only operative descriptions of a detail in the procedure that is typically not crucial to its completion. Conversely, however, those patients for whom the perinephric fat was described may therefore represent the extremes and actually serve as reasonable comparison groups for analysis. The retrospective nature of the study also limits its usefulness. Despite these weaknesses, however, we feel these data provide a starting place for future investigations into the phenomenon of sticky perinephric fat, including its clinical significance and underlying physiology.
Conclusion
Sticky perinephric fat can be a challenge for the surgeon in the process of mobilizing the kidney for the treatment of the small renal mass. Our data suggest an association of sex, age, tumor size, perinephric stranding, exophytic nature, and thickness of perinephric fat with this phenomenon. Partial nephrectomy for these patients tends to take longer and may also have increased risk of postoperative complications. All of the patients with high-grade disease were in the sticky fat group. These findings provide a first look at potential clinical features associated with perinephric sticky fat and provide a starting place for future investigations.
Footnotes
Disclosure Statement
No competing financial interests exist.