
Abstract
Background and Purpose:
Digital light processing-based hyperspectral imaging (DLP®-HSI) was adapted for use during laparoscopic surgery by coupling the spectral illumination source with a conventional laparoscopic light guide and incorporating a customized digital charge-coupled device camera for image acquisition. The system was used to characterize renal oxygenation during robot-assisted laparoscopic partial nephrectomy (RALPN) in humans.
Patients and Methods:
After Institutional Review Board approval, laparoscopic DLP-HSI was performed in consecutive patients undergoing RALPN at our institution. Time trends in relative tissue oxygen saturation (%HbO2) were descriptively analyzed. Associations between %HbO2 and patient age, comorbidities, and estimated glomerular filtration rate (eGFR) were investigated using the Kendall tau test.
Results:
Laparoscopic DLP-HSI was performed in 18 patients between May 2011 and February 2012. Median (interquartile range; IQR) age was 55.9 (49–67.5) years. Of the patients, 10/18 (56%) were men and 12/18 (66.7%) had a history of hypertension, diabetes, and/or tobacco use. Median (IQR) %HbO2 before, during, and after ischemia was 60.8% (57.9–68.2%), 53.6% (46.8–55.1%), and 61.5% (54.9–67.6%), respectively. Baseline %HbO2 was inversely associated with preoperative eGFR (τ=−0.38; P=0.036), and eGFR at most recent follow-up (τ=−0.38; P=0.036). Baseline or ischemic %HbO2 did not correlate with hypertension, diabetes, and/or tobacco history. Younger patients (<56 years) had a lower median baseline %HbO2 (P=0.07) and a higher median preoperative eGFR (P=0.038), than their older counterparts.
Conclusion:
The laparoscopic HSI system successfully characterized dynamic changes in renal oxygenation during RALPN. Intraoperative laparoscopic HSI outcomes have the potential to predict postoperative individual kidney function.
Introduction
The ability to monitor the renal response to ischemia in real time would be advantageous to the urologist and could influence intraoperative decision making with regard to specific strategies to minimize the impact of ischemia-related renal injury. Holzer and associates 8 recently reported the first clinical characterization of the renal response to ischemia in real time using digital light processing hyperspectral imaging (DLP®-HSI). 8 By incorporating a DLP-based Agile Light source (OL 490, Optronic Laboratories, Orlando, FL), a conventional laparoscopic light guide, a 0-degree laparoscope, and a customized digital charge-coupled device (CCD) camera (DVC, Austin, TX), we adapted DLP-HSI for use during laparoscopic surgery.
We evaluated the utility of the laparoscopic DLP-HSI system in characterizing renal ischemia in real time during RALPN in humans.
Patients and Methods
Study procedures
This study was approved by our Institutional Review Board, and each participant signed an informed consent. Consecutive patients scheduled for RALPN were recruited. RALPN was performed via a transperitoneal approach as described previously. 9 After mobilizing the kidney within the Gerota fascia and exposing the tumor, the laparoscopic DLP-HSI camera was inserted and a baseline surface oxygenation map (see below) was recorded. The renal artery alone or renal hilum en bloc was then occluded, and kidney oxygenation status during ischemia was recorded at several intervals. Finally, kidney oxygenation status was recorded shortly after restoring renal perfusion. Patient demographics, clinical features, and perioperative outcomes were also recorded in a prospective database.
Laparoscopic DLP-HSI system
The laparoscopic DLP-HSI system is shown in Figure 1. Similar to the previously described DLP-HSI system for open surgery, 8,10,11 the illumination source is a 500 W xenon arc lamp. Broadband white light from the source is diffracted and directed to a digital micromirror device (DMD) (Texas Instruments, Dallas, TX) (Fig. 2). The DMD is a digitally programmable micromirror array, which can be programmed such that discrete wavelengths of light fall onto distinct columns of micromirrors, allowing selection of a predetermined spectrum for illumination of the target (in our study, the selected spectrum spanned the reflectance range for oxy- and deoxyhemoglobin; 520–645 nm).

Laparoscopic DLP®-HSI system.

Digital light processing chip containing the digital micro-mirror device apparatus.
The processed light output is coupled to a conventional laparoscopic light guide (Karl Storz, GmBH and Co. KG, Tuttlingen, Germany) and transmitted to the target through a 0-degree, 10-mm laparoscope (Karl Storz). Spectral reflectance is transmitted back through the laparoscope to a high performance, digital CCD camera, which digitizes the reflectance images and transfers the data to a laptop computer for processing.
As described by Zuzak and colleagues, 11 a computer program synchronizes the DMD light source and the digital CCD camera and processes its output using a customized chemometric algorithm, delivering a color-coded image whereby the percentage of oxyhemoglobin (%HbO2) at each detector pixel is presented continuously as an oxygenation map in real time. The %HbO2 at each detector pixel is color encoded using a combination of colors between blue (deoxyhemoglobin) and red (oxyhemoglobin) (Fig. 3). From each image, a representative 100 pixel-square area was selected as an “optical biopsy,” and the mean %HbO2 of this region was recorded as a variable representing the oxygenation status of the kidney. All measurements were obtained at a fixed distance of 6 cm from the target, which was reproducibly achieved using a custom-built range finder consisting of a translucent 3.5F Tom Cat catheter (Tyco Healthcare, Mansfield, MA) taped to the end of the laparoscope. Previous experiments had established that this distance best optimized image acquisition by minimizing glare and enabling adequate focus.
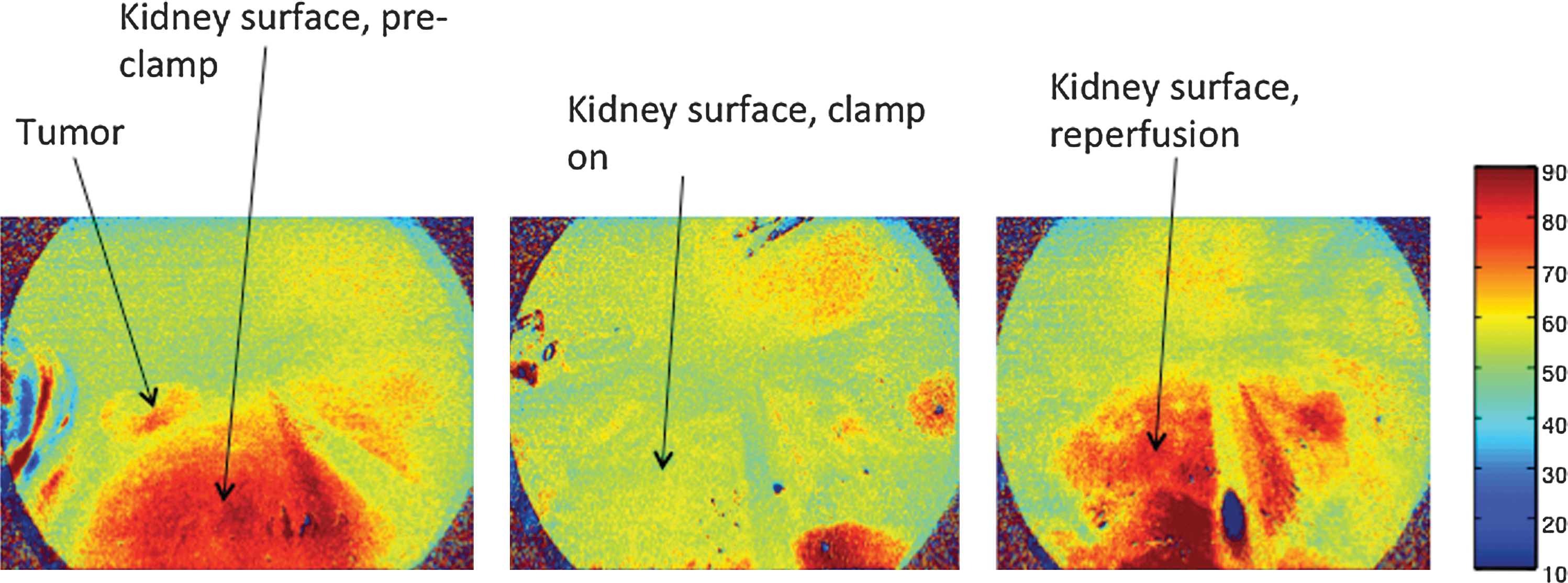
Color-coded kidney surface oxygenation maps. The color bar to the right of the images shows the combination of colors between blue (deoxyhemoglobin) and red (oxyhemoglobin) used to color code the %HbO2 at each pixel.
The DLP-HSI system currently operates in two illumination modes—the “bandpass” and ‘”spectral” illumination modes. 11 The spectral mode, in which three color-coded images per second are generated, was used in the present study.
Statistical methods
Temporal trends in %HbO2 were analyzed using descriptive statistics. Associations between %HbO2 and baseline clinical features (eg, diabetes and hypertension), as well as between %HbO2 and estimated glomerular filtration rate (eGFR) as determined by the Modification of Diet in Renal Disease equation, were investigated using the Kendall tau test. Age-adjusted eGFR and %HbO2 values were compared using the Mann-Whitney U test. Two-tailed analyses were performed in each case, with a P value≤0.05 considered statistically significant. Stata v10 statistical software (StataCorp, College Station, TX) was used.
Results
Between May 2011 and February 2012, a total of 18 patients undergoing RALPN were recruited. Patient demographics, clinical characteristics, and perioperative outcomes are outlined in Table 1. Median (interquartile range; IQR) age was 55.9 (49–67.5) years and 10/18 (56%) were male. 12/18 (66.7%) had a history of hypertension, diabetes and/or smoking.
9/18 (50%) of patients had two or more of these factors.
IQR=interquartile range; ASA=American Society of Anesthesiologists; DM=diabetes mellitus; HTN=hypertension; eGFR=estimated glomerular filtration rate; %HbO2=percentage of oxyhemoglobin.
Median (IQR) %HbO2 at baseline was 60.8% (57.9–68.2%), dropping to 53.6% (46.8–55.1%) after a mean of 8.7 minutes of warm ischemia, and returning to 61.5% (54.9–67.6%) after restoring perfusion (Fig. 4). The %HbO2 during ischemia was significantly lower than the baseline value (P=0.0004), while %HbO2 at reperfusion was statistically similar to that at baseline (P=0.22).
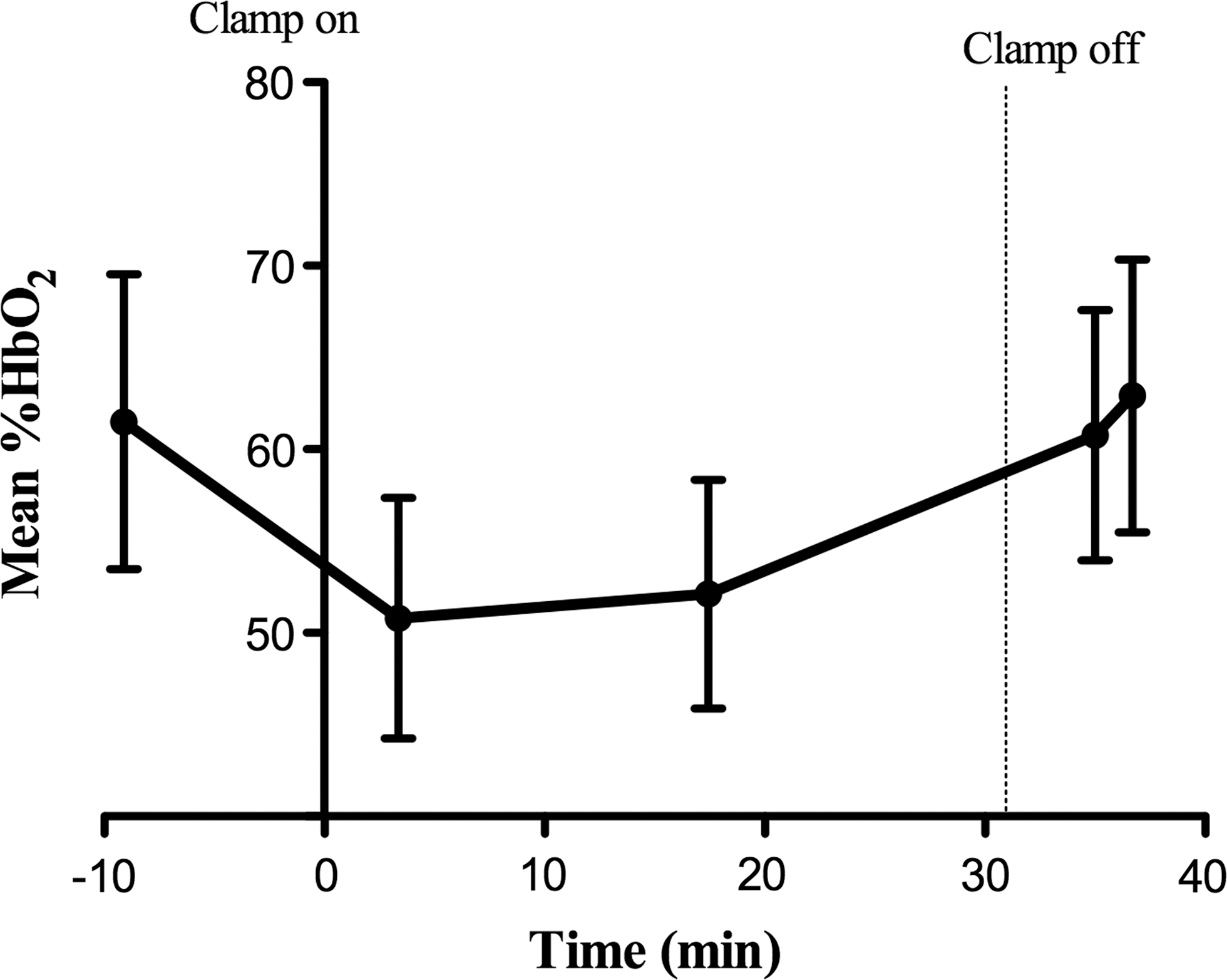
Mean percentage of oxyhemoglobin (%HbO2) vs time.
There was a significant inverse association between baseline %HbO2 and baseline eGFR (τ=−0.38; P=0.036), as well as between baseline %HbO2 and eGFR at the most recent follow-up (τ=−0.38; P=0.036). Correlations between baseline %HbO2 and diabetes, hypertension, or smoking history were not statistically significant (Table 2). Similarly, correlations between %HbO2 during ischemia and the above variables were not statistically significant, while correlations for %HbO2 during reperfusion mirrored those for baseline %HbO2 (Table 2). Patients younger than 56 years (median age) had a lower median baseline %HbO2 (58.7 vs 65.4; P=0.07) and a significantly higher median preoperative eGFR (100.1 mL/min/m2 vs 80.2 mL/min/m2; P=0.038) than their older counterparts. There was a positive correlation between baseline %HbO2 and patient age, which approached statistical significance (τ=0.31; P=0.09).
eGFR=estimated glomerular filtration rate; DM=diabetes mellitus; HTN=hypertension; %HbO2=percentage of oxyhemoglobin.
%HbO2 during ischemia did not significantly differ for patients who underwent artery only (n=6) vs artery + vein (n=12) occlusion (54.3% vs 53.0%, respectively; P=0.60). Warm ischemia time did not independently predict postoperative eGFR during acute (median 1 day) or most recent (median 18.5 days) follow-up (P=0.93 and 0.65, respectively).
Discussion
Imaging spectroscopy, whereby spectroscopy is combined with remote satellite or aerial imaging to deliver an image in which each pixel carries spectroscopic information about the illuminated target, was developed in the 1980s, 12 and its use in the clinical setting was first described in 2001. 13 Zuzak and coworkers 13 developed an HSI system for tissue imaging spectroscopy, which quantitated the oxygen saturation of hemoglobin using separation chemometrics. Image processing times with early HSI systems were between 30 and 40 seconds and were significantly reduced by incorporating DLP with HSI.
Holzer and associates 8 characterized renal oxygenation in 21 patients undergoing OPN using DLP-HSI. Mean patient age was 56 years (range 29–78). Median baseline %HbO2 was 74.6%, decreasing by 20% during hilar occlusion, and rebounding to 80% to 90% of baseline after restoring perfusion. In the present study, renal oxygenation during RALPN was evaluated using a novel laparoscopic DLP-HSI system. Trends in %HbO2 mirrored those described during OPN. The numerical values for the baseline and nadir %HbO2 in our study, however, were lower than those reported by Holzer and colleagues. A possible explanation for these findings may lie in consideration of the Bohr effect.
The interaction between the hemoglobin molecule and oxygen is characterized by an S-shaped equilibrium curve. Each hemoglobin molecule is capable of binding four oxygen molecules; binding of each oxygen molecule increases hemoglobin affinity for the binding of additional oxygen molecules, until the saturation point is reached. A shift of the dissociation curve to the right (the Bohr effect 14 ) indicates decreased affinity of hemoglobin for oxygen, whereby at a given partial pressure of oxygen (pO2), a lower hemoglobin oxygen saturation is achieved. An increase in the plasma partial pressure of carbon dioxide (pCO2) and a decrease in pH, both of which are known to be associated with a CO2 pneumoperitoneum, 15,16 are among the factors known to create a Bohr effect. Accordingly, baseline %HbO2 measured under a CO2 pneumoperitoneum would be expected to be lower than that measured during open surgery.
An interesting observation in our small pilot study was that younger patients had a lower %HbO2 than their older counterparts but had a significantly higher baseline eGFR. GFR and renal blood flow are known to decline with age. 17 Furthermore, in kidneys with disease-related decline in function, renal blood flow and overall renal oxygen consumption are known to be reduced relative to normal kidneys, despite higher renal oxygen extraction. 18 Renal blood flow is also known to be reduced in a CO2 pneumoperitoneum. 19
In our series, older patients were more likely to have a history of diabetes, hypertension, and/or smoking (89% vs 44%; P=0.05) and were thus more likely to have diseased kidneys. Pneumoperitoneum effects on renal blood flow, although not quantified in our study, could have lowered effective renal plasma flow in younger patients to levels similar to those for older patients. Accordingly, the lower renal oxygen consumption in the older group could have resulted in a higher %HbO2 for this group. Indeed, we observed a nearly significant positive correlation between %HbO2 and patient age. These observations warrant further investigation.
Our pilot study has a few limitations worth discussing. First, with this early prototype laparoscopic DLP-HSI system, the images produced intraoperatively in real time display a color-encoded representation of tissue %HbO2; sampling of representative areas to determine numeric %HbO2 and statistical relevance was performed postoperatively. A newer system offers the ability to probe the color-coded image for numeric data in real time, but this presently requires a skilled technician. Second, variations in ventilation settings and pneumoperitoneum gas flow from case to case may have resulted in variation in concentrations of dissolved oxygen and CO2 in the patients' serum, and in variations in renal plasma flow, each of which could have introduced some variability in %HbO2 measurements. Future studies should consider standardizing patient anesthesia and continuously recording pneumoperitoneum gas flow, so as to appropriately adjust for these variables.
Third, eGFR is an estimate of overall renal function, and postoperative changes in this variable likely do not accurately reflect changes within the individual renal unit subjected to ischemia; however, to date, a standardized technique for measuring postoperative function in individual kidneys subjected to partial nephrectomy in the setting of a normal contralateral kidney has not been described. Despite these limitations, we believe that the laparoscopic DLP-HSI system is a promising new technology that, pending future enhancements, has the potential to aid noninvasive investigation of the impact of ischemia on individual kidneys.
Conclusion
The laparoscopic HSI system successfully characterizes dynamic changes in renal oxygenation during RALPN and has the potential to predict changes in individual kidney function postoperatively. Future clinical application may be aided by further device enhancements and output parameterization, including incorporation of capabilities for simultaneous measurement of spectra for renal ischemia-specific metabolites in addition to those for hemoglobin.
Footnotes
Disclosure Statement
Dr. Karel Zuzak is a senior Biomedical Research Engineer at Digital Light Innovations, a DLP-authorized design house for Texas Instruments. For all other authors, no competing financial interests exist.