
Abstract
Background and Purpose:
Previous studies using pulsed fluoroscopy have shown variable effects on radiation exposure because of the ramp and trail effect in older C-arm systems. This study compares radiation delivered in pulsed and continuous modalities using a modern C-arm system.
Materials and Methods:
Thermoluminescent dosimeters (TLDs) positioned in three body locations directly measured radiation dose during simulated ureteroscopy. Thirty pedal activations were administered using a pulsed or continuous mode to visualize an implanted guidewire and a radiopaque stone. TLD absorbed radiation and image quality were compared between imaging modes.
Results:
Pulsed fluoroscopy delivered less radiation compared with continuous fluoroscopy at each site: Anterior skin (0.10 vs 0.26 mGy, P<0.001), kidney (0.15 vs 0.40 mGy, P<0.001), and posterior skin (0.92 vs 2.62 mGy, P<0.001). Mean fluoroscopy time differed between continuous and pulsed modes (12.5 vs 3.0 seconds; P<0.001). Fluoroscopy time positively correlated with radiation exposure at all sites: Anterior skin (0.017 mGy/s, R2=0.90), left kidney (0.026 mGy/s, R2=0.96), and posterior skin (0.18 mGy/sec, R2=0.98). When evaluated by blinded urologists, 100% of reviewers felt pulsed images were adequate to identify guidewire position and 90.5% felt pulsed images were adequate for stone localization.
Conclusion:
Pulsed fluoroscopy reduced fluoroscopy time by 76% and radiation dose by 64% compared with continuous fluoroscopy. Pulsed fluoroscopy images were adequate for most tasks of ureteroscopy and should be considered for reduction of radiation during ureteroscopy.
Introduction
This study compared the fluoroscopy time, radiation dose, and picture quality obtained when operating a modern C-arm in the continuous and pulsed modes.
Materials and Methods
This study protocol was approved by the Department of Anatomic Pathology and was performed in accordance with the institutional policies for use of anatomic specimens. Thermoluminescent dosimeters (TLDs) (Harshaw TLD-100 chips; Thermo Fisher Scientific, Waltham, MA) were positioned at the left posterior skin in line with the left renal hilum, the left renal hilum, and the left anterior skin in line with the left renal hilum in a female human cadaver to directly measure the radiation dose at these sites. The cadaver was positioned in the lithotomy position identical to that of clinical patients undergoing ureteroscopy. With the fluoroscopy beam positioned in line with the left kidney, the cadaver received 30 short pedal activations to produce an image in either the continuous or pulsed mode at 1 PPS using a modern C-arm system (GE OEC® 9900 Elite; GE Healthcare; Salt Lake City, UT) at fixed settings of 69 kVp and 1.51 mAs to visualize an inserted 0.038″ Teflon-coated guidewire and a 1 cm calcium oxalate stone. Fifteen trials of 30 pedal activations were performed in both the continuous and pulsed modes with new TLDs implanted at each site for each trial.
TLDs were processed and read in a standardized fashion that has been published. 6 All images were saved to an IMPAX (AGFA Healthcare; Greenville, SC) imaging system. Image quality was assessed by 13 urology attendings and 8 urology residents who compared quality of images showing a 0.038″ standard guidewire and a 1 cm calcium oxalate stone. Participants were specifically asked whether continuous and pulsed fluoroscopic images were adequate to visualize the stone and guidewire, and were then asked which image was superior, and whether the images provided adequate information to perform ureteroscopy.
Statistical analysis was performed using SPSS 17 (SPSS, Chicago, IL). The absorbed radiation dosages between the two modalities were compared using a paired two-tailed Student t test (α=0.05) and least-squares analysis. The images of the two modalities were compared with a Wilcoxon signed-rank test.
Results
Pulsed fluoroscopy delivered a significantly lower mean radiation dose compared with continuous fluoroscopy at each site. The pulsed mode reduced the dose at the anterior skin by 62%, (0.10 vs 0.26 mGy, P<0.001), at the kidney by 63% (0.15 vs 0.40 mGy, P<0.001), at the posterior skin by 65%, (0.92 vs 2.62 mGy, P<0.001), and at all sites combined by 64% (0.39 mGy vs 1.09 mGy, P<0.001) compared with the continuous mode (Fig. 1). Mean fluoroscopy time differed significantly between continuous (12.5 seconds, range 12.2–13.7 seconds) and pulsed modes (3.0 seconds, range 2.9–3.0 seconds; P<0.001). A positive correlation between time and radiation exposure was noted when combining imaging modalities: Anterior skin (R 2 =0.90), left kidney (R 2 =0.96), and posterior skin (R 2 =0.98).
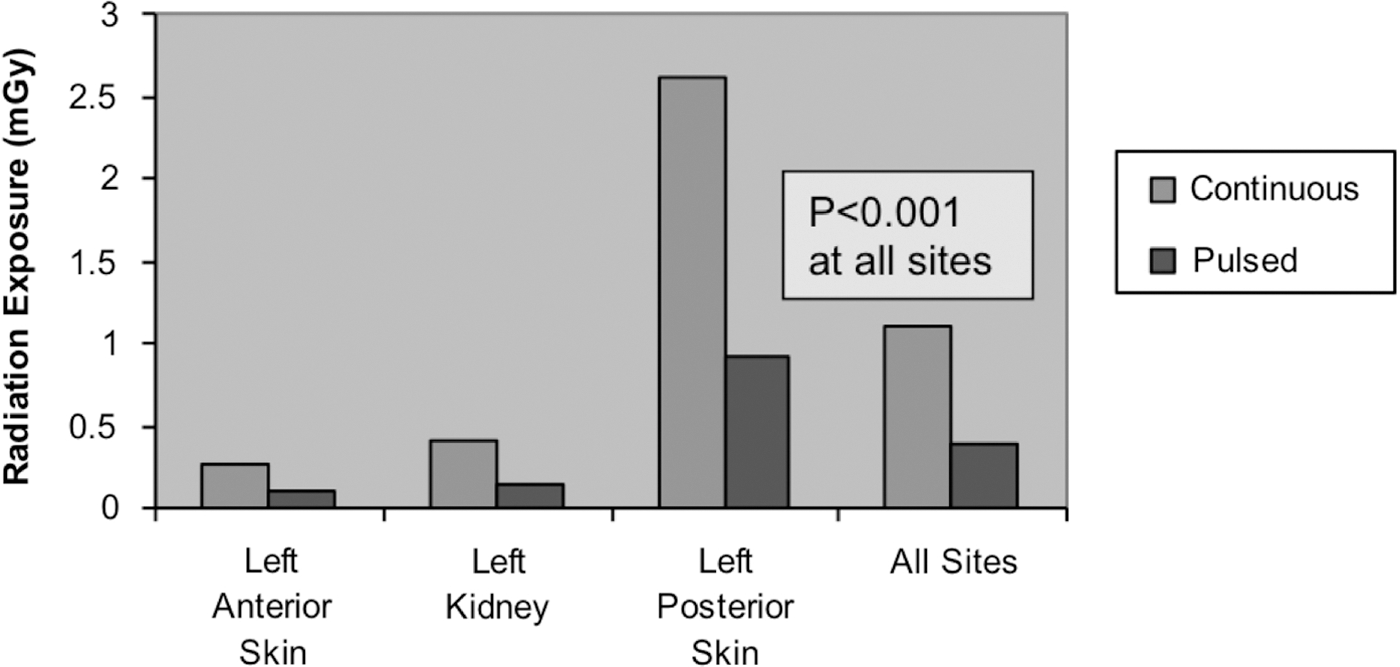
Mean radiation dose by location in continuous and pulsed fluoroscopy.
The pulsed mode delivered more radiation per second of fluoroscopy time compared with the continuous mode overall and at individual sites: Anterior skin increased by 36%, (0.033 vs 0.021 mGy/sec, P<0.001), the kidney increased by 36% (0.050 vs 0.032 mGy/sec, P<0.001), the posterior skin increased by 32%, (0.307 vs 0.209 mGy, P<0.001), and all sites combined increased by 31% (0.13 mGy vs 0.09 mGy/s, P<0.001). The pulsed mode, however, delivered less radiation per standardized pedal depression when compared with the continuous mode overall and at all sites: The anterior skin decreased by 67%, (0.003 vs 0.009 mGy/pedal depression, P<0.001), the kidney decreased by 62% (0.005 vs 0.013 mGy/pedal depression, P<0.001), the posterior skin decreased by 64%, (0.031 vs 0.087 mGy/pedal depression, P<0.001), and all sites combined decreased by 64% (0.013 vs 0.036 mGy/pedal depression, P<0.001).
When 21 blinded urologists evaluated images acquired in each mode, they found the image quality to be superior when locating a stone in the continuous mode compared with the pulsed mode (P=0.02). Specifically, in detecting the 1 cm calcium oxalate stone, 14 (67%) reviewers rated the continuous images as superior to the pulsed images, 6 (29%) thought both images were equal, and one (4.8%) said the continuous stone image was inferior. When evaluating the guidewire position, the group found no difference in image quality between the two imaging modes (P=0.70). Specifically, 8 of 20 (40%) reviewers thought that the continuous fluoroscopy picture was superior, 10 of 20 (50%) thought that the images were identical, and 2 of 20 (10%) thought that the pulsed images were better. However, 90.5% and 100% of the reviewers thought that the pulsed images of the stone and guidewire, respectively, supplied adequate information to perform ureteroscopy (Fig. 2).
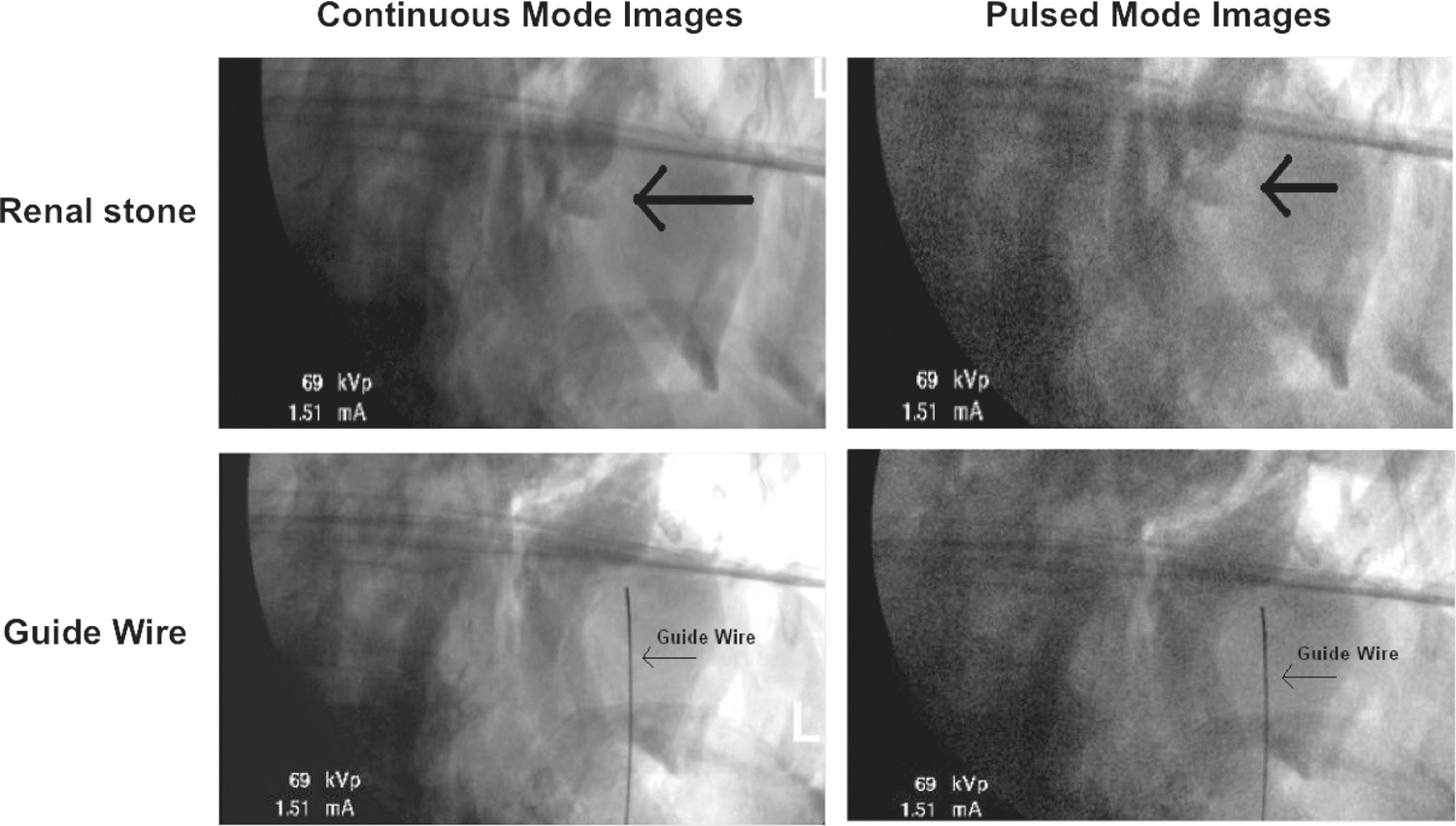
Image comparison between continuous and pulsed fluoroscopy.
Discussion
The United States Food and Drug Administration recently issued a guideline emphasizing the importance of reducing patient radiation exposure during fluoroscopic studies 7 because ionizing radiation used in medical imaging accounts for up to 3% of cancers per year. 8 Thus, the as low as reasonably achievable principle should be maintained to reduce radiation exposure during medical imaging. 9 –11 Previously published methods for reducing patient radiation exposure during fluoroscopy include minimizing exposure time, collimation, shielding, reducing exposure settings, using last image hold, use of a laser guide for the C-arm, using an experienced fluoroscopy technician, recording fluoroscopy time, and minimizing the number of spot radiographs obtained. 1,10,12,13
In a previous study that compares a protocol using many of these radiation reducing strategies, we reduced fluoroscopy time from 86.1 seconds to 15.5 seconds, an 82% exposure time reduction in the conventional continuous mode. 13 In this current study, we tested whether fluoroscopy in the pulsed mode would result in a further reduction in radiation dose compared with the continuous mode.
Pulsed fluoroscopy was initially developed to decrease patient fluoroscopy time by reducing the number of exposures per second. Early fluoroscopy units, however, produced radiation pulses at the generator resulting in a “ramp and trail” effect. This bell-shaped curve of increasing and decreasing current accounts for the low energy X-rays absorbed by the patient as the pulse approaches a set amperage (Fig. 3A) because of cable resistance. 1 These attendant low energy X-rays increased the radiation dose per pulse causing conventional pulsed fluoroscopy to offer minimal dose savings over continuous fluoroscopy. 1 –5,14
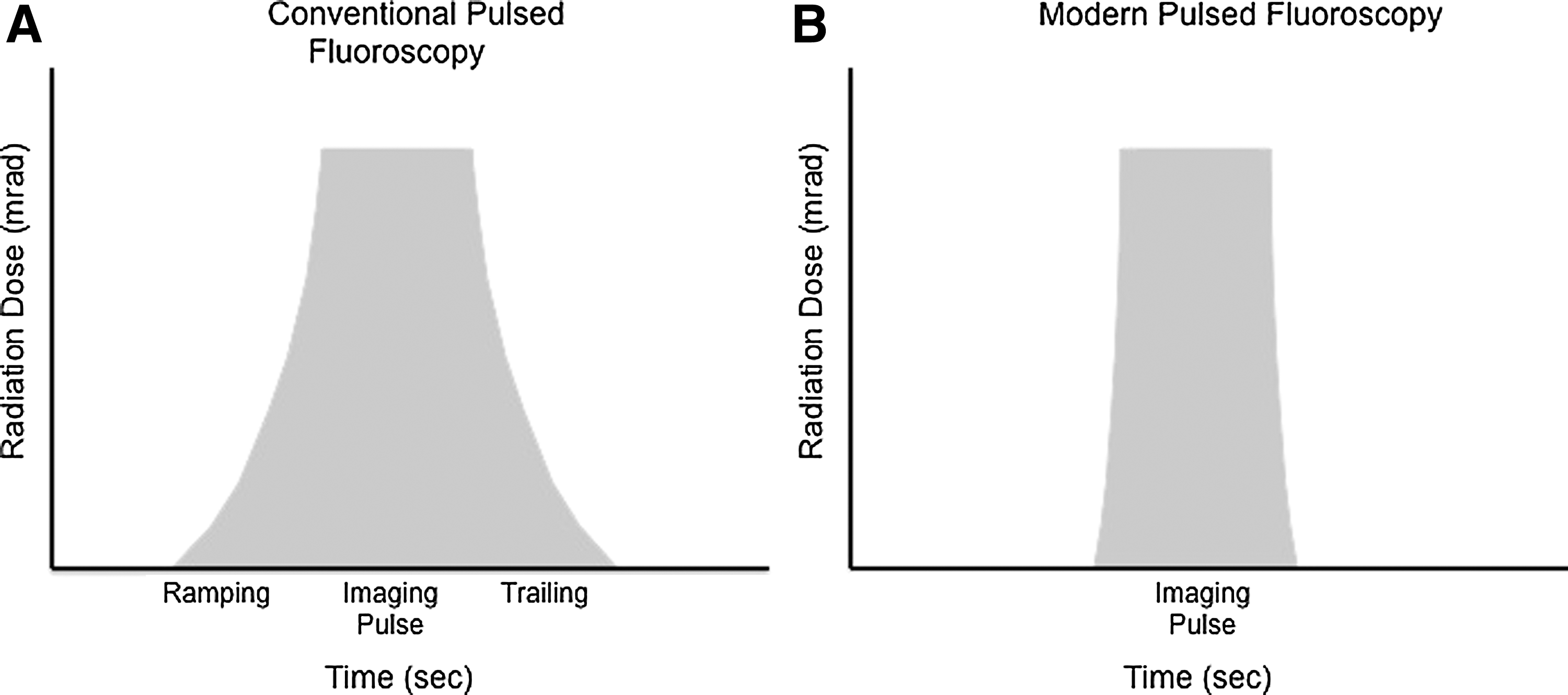
Radiation exposure in conventional and modern pulsed fluoroscopy with time plotted on the x-axis and radiation dose on the y-axis.
Newer C-arm units control pulses in the X-ray tube and not in the generator, which removes cable capacitance and minimizes the ramp and trail effect. A single-shot exposure in the pulsed mode of newer systems produces an image at a set amount of radiation, reaching that set amount more quickly, reducing the exposure time (Fig. 3B). 1,10 This technology potentially reduces radiation exposure with a lower pulse rate, 15 maintains image contrast using the same voltage, and improves image sharpness. 10,16
Another advantage of pulsed fluoroscopy is reduction of the blooming effect of the image intensifier. 1,17 In the continuous mode, blooming occurs when the image intensifier compensates for movement from a dense area, such as the bony pelvis, to a less dense area, such as the lower pole of the kidney, causing a temporary overexposure. A small time elapses before an automatic exposure device corrects the new field of view to the appropriate exposure. This effect is significantly reduced using pulsed fluoroscopy because each pulse automatically achieves the desired exposure level. 1
Studies with newer C-arm systems have shown that pulsed fluoroscopy decreases radiation exposure to the patient during invasive procedures in the fields of cardiology, urology, and radiology, but no study has evaluated the reductions achievable at 1 PPS. Chida and associates 18 demonstrated a 40% decrease in radiation exposure at 15 PPS using pulsed fluoroscopy during interventional cardiology procedures. 18 Other studies have shown dose savings to the patient of 22% for pulse rates of 15 PPS, 38% for 10 PPS, and 49% for 7.5 PPS, and 50% for 6.25 PPS. 2,3,19
To our knowledge, no previous study has directly compared radiation dose received in the continuous mode and the pulsed mode at 1 PPS. We demonstrated a 64% overall reduction in radiation dosage compared with continuous fluoroscopy at identical exposure settings.
While radiation doses per second are higher in the pulsed mode (0.13 mGy/s in pulsed vs 0.09 mGy/s in the continuous mode), the increased number of pulses per pedal depression in the continuous mode accounts for the overall greater radiation dose. In our study, the radiation dose of a single pedal depression is increased in the continuous mode (0.04 mGy/pedal depression) compared with the pulsed mode (0.01 mGy/pedal depression; P<0.001) when comparing all sites.
Overall, we found the exposure time to be significantly more in continuous fluoroscopy when compared with pulsed fluoroscopy (12.5 seconds vs 3 seconds; P<0.001). In our study, the foot pedal was activated in the same manner and the same length of time in both continuous and pulsed modes. In doing so, the fluoroscopy timer indicated that the exposure time was significantly greater in the continuous mode at 12.5 seconds compared with the 3 seconds in the pulsed mode (P<0.001) for 30 pedal activations. Despite significantly greater radiation per second in the pulsed mode, the dramatically reduced exposure time still resulted in a 64% decrease in overall radiation dose.
One potential limitation of pulsed fluoroscopy is a potential for loss of diagnostic information. Cohen 20 demonstrated that fluoroscopy at less than 30 PPS decreased the ability to evaluate the risk of true aspiration through the vocal cords during pediatric swallowing studies. In contrast, two previous studies evaluated the ability of pulsed fluoroscopy for voiding cystourethrography, with both studies concluding that pulsed fluoroscopy resulted in adequate images. 10,21 Boland and colleagues 1 demonstrated no perceptual difference by blinded radiologists with pulse rates as low as 3.75 PPS during gastrointestinal and genitourinary studies. 1
In cardiology, Kotre and coworkers 19 thought that although pulsed fluoroscopy at 6.25 PPS resulted in reduced image quality, it was still adequate to easily visualize pacing wires. They concluded that it is possible to use very low pulse rates during fluoroscopic examinations where high image quality is unnecessary for the successful outcome of the procedure. Similarly, our study showed decreased image quality when detecting a 1 cm calcium oxalate stone, but these 1 PPS images were thought to be adequate to identify the stone by 90.5% of reviewers. Very dense structures such as the guidewire were thought to be adequately visualized 100% of the time.
There are some limitations to this study. First, our study involved a single cadaver and not human subjects. Thus, differences in body mass indices between patients were not determined. The radiation beam path length affects both the patient entrance exposure and the image quality—the larger the human, the more radiation exposure. Also, the cadaver lacked normal patient movement such as breathing that occurs in a living patient during surgery, thus eliminating one potential cause of image degradation. Image degradation in the operating room, however, can be reduced by timing fluoroscopic activation during end-expiration. Furthermore, this study showed adequacy of pulsed images to detect dense structures like a guidewire and a 1 cm calcium oxalate stone. The ability to detect less dense stones and smaller stone pieces was not specifically tested, but would likely be reduced in pulsed fluoroscopy. If during the procedure the image quality does not allow detection of subtle findings, however, the surgeon can easily switch from a pulsed to a continuous mode.
Despite these limitations, this study demonstrates that pulsed fluoroscopy dramatically reduces fluoroscopy time and exposure compared with continuous fluoroscopy. This study also demonstrates that fluoroscopy at 1 PPS produced images that are adequate to perform most steps during ureteroscopy.
Conclusion
Pulsed fluoroscopy significantly reduces radiation exposure compared with continuous fluoroscopy. Using the same pedal activations in each modality, the pulsed mode resulted in higher radiation exposure per second compared with the continuous mode. Pulsed fluoroscopy, however, reduced fluoroscopy time by 76% and overall radiation exposure by 64% compared with continuous fluoroscopy. Using pulsed fluoroscopy at 1 PPS provides adequate images for ureteroscopy. Customization of the fluoroscopy mode commensurate with the quality of the image needed for different steps in the procedure will allow urologic surgeons to dramatically reduce radiation exposure to their patients, staff, and themselves while maintaining adequate image quality for the desired task.
Footnotes
Acknowledgments
Bertha Escobar-Poni, M.D. (Pathology and Human Anatomy Department) donated the cadaver for the study. Steven Rightnar (Radiobiology Research Department) assisted with the measurement and conversion of radiation dose in this study.
Disclosure Statement
No competing financial interests exist.