
Abstract
Background and Purpose:
Urinary stones >2 cm are traditionally managed with percutaneous nephrolithotomy (PCNL). Recently, flexible ureteroscopy and laser lithotripsy) (FURSL) has been used to manage them with comparable results. In a comparative study of renal stones between 2 and 3 cm, FURSL was reported to need less second-stage procedures and be just as effective as PCNL. Our purpose was to review the literature for renal stones >2 cm managed by ureteroscopy and holmium lasertripsy.
Materials and Methods:
A systematic review and quantitative meta-analysis was performed using studies identified by a literature search from 1990s (the first reported large renal stones treated ureteroscopically) to August 2011. All English language articles reporting on a minimum of 10 patients treated with FURSL for renal stones >2 cm were included. Two reviewers independently extracted the data from each study. The data of studies with comparable results were included into a meta-analysis.
Results:
In nine studies, 445 patients (460 renal units) were reportedly treated with FURSL. The mean operative time was 82.5 minutes (28–215 min). The mean stone-free rate was 93.7% (77%–96.7%), with an average of 1.6 procedures per patient. The mean stone size was 2.5 cm. An overall complication rate was 10.1%. Major complications developed in 21 (5.3%) patients and minor complications developed in 19 (4.8%) patients. A subgroup analysis shows that FURSL has a 95.7% stone-free rate with stones 2–3 cm and 84.6% in those >3 cm (P=0.01), with a minor complication rate of 14.3% and 15.4%, respectively, and a major complication rate of 0% and 11.5%, respectively.
Conclusion:
In experienced hands, FURSL can successfully treat patients with stones >2 cm with a high stone-free rate and a low complication rate. Although the studies are from high-volume experienced centers and may not be sufficient to alter everyday routine practice, this review has shown that the efficacy of FURSL allows an alternative to PCNL.
Introduction
The last decade has witnessed not only technical advancements in endoscopic procedures and equipment, but also an increase in surgical skills using them. 3,6,7 The development of smaller diameter scopes, increased scope flexibility, improvement of accessories, and holmium laser technology has led more urologists to attempt management of large renal stones with flexible ureteroscopy and laser lithotripsy (FURSL). The resulting SFRs were comparable to those of PCNL. 3,4,8 Indeed, studies report a SFR of 88% to 92% in patients with large stones. 3,4
To this end, we aimed to conduct a systematic review and a meta-analysis to assess the efficacy and safety of FURSL in the treatment of patients with renal stones larger than 2 cm. Our secondary aim was to assess the operative times, number of procedures per patient needed to achieve a SFR, average stone size, and the use of ureteral access sheaths.
Materials and Methods
Search strategy and study selection
The systematic review was performed according to the Cochrane reviews guidelines. The search strategy was conducted to find relevant studies from MEDLINE (1990–August 2011), EMBASE (1990–August 2011), Cochrane Central Register of Controlled Trials-CENTRAL (in The Cochrane Library-Issue 1, 2011), CINAHL (1990–August 2011), Clinicaltrials.gov, Google Scholar, and individual urologic journals.
Terms used included: “ureteroscopy,” “flexible ureteroscopy,” “large stones,” “stones >2 cm,” “urolithiasis,” “renal,” “calculi,” “laser,” and “lasertripsy.”
Mesh phrases included: (“Ureteroscopy"[Mesh]) AND “Urinary Calculi"[Mesh] and (“Ureteroscopy”[Mesh]) AND “Urinary Calculi”[Mesh]) AND “Lasers, Solid-State”[Mesh].
Articles in languages other than English were included if data were extractable and references of searched papers were evaluated for potential inclusion. Authors of the included studies were contacted wherever the data were not available or not clear.
Two reviewers (OA and BS) identified all studies that appeared to fit the inclusion criteria for full review. Each reviewer independently selected studies for inclusion in the review. Disagreement between the two extracting authors was resolved by consensus by all authors.
Data extraction and analysis
Studies relevant to ureteroscopic management of patients with stones larger than 2 cm were included. The following variables were extracted from each study: Period of the study, country of origin of the study, number of patients included, operative time, SFRs after completion of management, number of procedures per patient, stone sizes, and complications. The data of each study were grouped into a meta-analysis, in an intention to treat basis, to allow a numerical representation of the results. Data that were similar were pooled and included for the meta-analysis. Furthermore, a subgroup analysis was conducted to evaluate the SFR, mean number of procedures, and complications in patients with stones 2 to 3 cm and in those with stones >3. For continuous data a Mantel-Haenszel chi-square test was used and for dichotomous data an inverse variance was used.
A quality assessment of harms using the McHarm scale, was conducted for each included study. 9 This was deemed appropriate by all reviewers because we were analyzing safety as well as efficacy of ureteroscopic treatment of large stones. We used Review Manager (RevMan 5.0.23) to plot the quality assessment of harms tables.
Results
The literature search yielded 296 studies, of which 273 were excluded because of nonrelevance based on titles (252) and abstracts (21) (Fig. 1). These titles and abstracts of the studies did not focus on FURSL or large stones; hence, the exclusion. Full manuscripts were evaluated in 23 studies, of which, 9 were included into the review. 4 –8,10 –13 The majority of the studies were published within the last 3 years, reflecting the increased use of FURSL for fragmentation of large stones. 4 –6,10,11,13
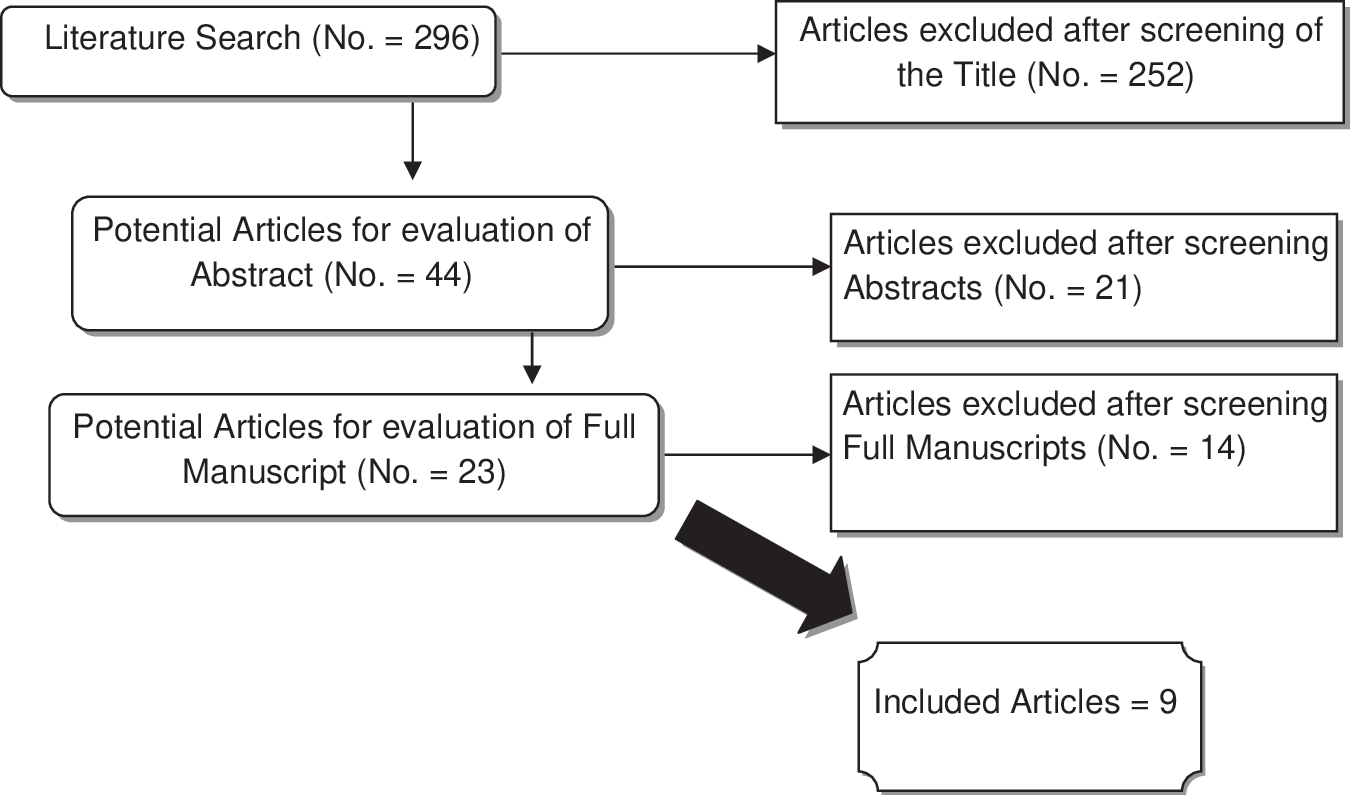
Flowchart for article selection of the review.
All included studies were cohort observational studies, with no randomization or control groups and reported on FURSL for renal stones larger than 2 cm. All studies reported on the variables indicated in the data extraction section and are plotted in Tables 1 and 2. Tables 3 and 4 delineate patients grouped into stone size 2 to 3 cm and >3 cm.
USA=United States of America; UCLA=University of California, Los Angeles; UK=United Kingdom.
SFR=stone-free rate; CVA=cerebrovascular accident; UTI=urinary tract infection.
Study mentions that after 18-month follow-up, 3/120 patients needed reoperation for residual stones.
The surgical time was what was counted into the meta-analysis.
SFR=stone-free rates; UTI=urinary tract infection.
SFR=stone-free rates; ITU=intensive treatment unit; UTI=urinary tract infection.
After reading the full manuscripts, we excluded 14 studies. Eight of these studies were not related to FURSL of large stones. Three looked at combined electrohydraulic and holmium laser treatment of stones where the electrohydraulic treatment was the main procedure. 1,14,15 Two other studies had patients with stones larger than 1 cm. 3,16,17 The last study overlapped with a similar included study from the same authors. 13,18 While the included study was more focused on the FURSL treatment of large stones, the excluded study was aimed at comparing PCNL with FURSL. 18
Characteristics of the included studies
The studies were published between 1998 and 2011, with majority conducted in the United States (5/9), three conducted in Europe, and one in Africa. There were 460 renal units in 445 patients with an age range between 10 and 78 years. There were 1.4 times as many men as there were women (Table 1). All the studies reported on FURSL of stones >2 cm.
With regard to the main outcome of efficacy, all nine studies reported on SFRs, and eight studies reported on complications; however, Breda and associates (2009) was not clear on whether complications occurred in patients with stones larger or smaller than 2 cm and therefore this information was left out of the meta-analysis. 4,6 –8,10 –13 Two studies were from the same institute, but were on different cohorts of patients; therefore both studies were included. 7,11 Hussain and colleagues 5 only reported on SFRs of varying sized stones with no mention of any other outcome that could be included. Six studies reported on the average number of procedures performed, 4,6 –8,10,11 with seven studies reporting on the average operative time. 4,6,7,10 –13 A further five studies reported their use of ureteral access sheath. 4,6,7,10,11,13 All studies reported on stone size. One article had included one child with a large renal stone, while the remaining cohort were adults; therefore, the study was included because the authors did not think one patient's results can skew the final outcome. 8 Furthermore, two of studies just mentioned that the stones were larger than 2 cm rather than the average and therefore this information was excluded from the meta-analysis.
In five studies, the data for the subgroup analysis were performed; however, only SFR data were available for all five of the studies. 4,6,7,10,12 Mean procedure number and minor complications were analyzed in three studies in the 2 to 3 cm group and two in the 3 cm group (Tables 3 and 4), while major complications were analyzed in four studies in the 2 to 3 cm group and two in the 3 cm group (Tables 3 and 4).
Meta-analysis results
The combined data of the included studies showed that FURSL had an average SFR of around 93.7% (77%–97.5%) with an average of 1.6 procedures per patient.
Concerning complications, the combined data had an overall complication rate of 10.1%, with minor complications developing in 19 (4.8%) patients, major complications developing in 21 (5.3%) patients, and a 0% mortality rate.
Of the 19 minor complications, self-limiting hematuria occurred in six patients, postoperative pyrexia or pain in three patients, urinary tract infection treated with simple oral antibiotics in five patients, and minor intraoperative bleeding and postoperative urinary retention in one patient each.
Of the 21 major complications, Steinstrasse occurred in five patients, subcapsular hematoma in four patients, and obstructive pyelonephritis in four patients of which one went to the intensive care unit. The remaining three major complications were cerebrovascular accident, acute prostatitis, and hematuria causing clot retention in one patient each.
The average operative time was 82.5 minutes with a range of 28 to 215 minutes. The average stone size of the combined data was 2.5 cm. The combined use of ureteral access sheaths came to 86%. A subgroup analysis grouped into stones 2 to 3 cm and >3cm was also performed (Tables 3 and 4). There were 162 patients in the 2 to 3 cm stone group and 52 in the >3 cm group. It was evident that the success rate for FURSL for stones 2 to 3 cm was higher than for stones >3 cm with 95.7% vs 84.6% (P=0.01; odds ratio: 4.03; 95% confidence interval [CI]: 1.38–11.72) SFR, respectively. Furthermore, the 2 to 3 cm stone group had fewer procedures per patient (mean 1.46±0.2 vs 1.85±0.02 (P<0.0001; 95% CI: −0.42–0.36)). There were also fewer minor and major complications than the >3 cm group (14.3% vs 15.4%, and 0% vs 11.5%).
Methodologic quality assessment
Overall, the quality of the reported studies was poor, because six of the studies were reported as retrospective while two were unclear, although they seemed to be retrospective from the methodology. All the included studies may be subject to bias because they recruited patients from databases retrospectively; this could lead to selection as well as reporting bias. Some of the studies did not prospectively define the selection of patients for FURSL as opposed to PCNL. 5,7,12,13 The majority of the studies, however, mentioned that FURSL was attempted because of previous PCNL or SWL failure, patient preference after counseling, or if PCNL was contraindicated. 4,6,8,10,11 None of the studies was randomized or had a control group. Blinding was not an issue, because this is a surgical procedure and all groups will know the modality of treatment eventually. All the studies had clearly focused aims and used appropriate methodology to address those aims. There seemed to be no or little risk of classification bias because all the studies had the numbers accounted for, and all the patients had similar treatments.
The quality assessment of harms indicates that the studies generally have a low risk of bias concerning reporting the harms that could potentially be caused by the procedure (Table 5). The harms quality assessment could not be performed on one study because that study had not reported on any complications and did not mention an intention to do so. 5
Discussion
Principal findings
In this review, FURSL had an average SFR of around 93.7% (77%–97.5%) for a mean stone size of 2.5 cm, with an average of 1.6 procedures per patient and a mean operative time of 82.5 minutes. On a subgroup analysis, the SFR for stones between 2 and 3 cm was statistically significantly better than for stones >3 cm (95.7% vs 84.6%; P=0.01). Minor and major complications were seen in 4.8% and 5.3%, respectively.
Meaning of the study and comparison of FURSL in various studies (possible mechanism and implications for policy and practices)
Ureteroscopy and laser fragmentation of stone in the upper urinary tract has undergone development and refinement. 4,19 –22 Rigid ureteroscopy (URS) has been proven to be as efficient in stone clearance as SWL for proximal ureteral stones and superior in treating distal ureteral stones. 19,20
Harmon and coworkers 23 reported that because of the decrease in size of the ureteroscope, their complication rates for URS dropped from 6.6% to 1.5%. With advancements in ureteroscopic technology, the overall complication rates have decreased with major complication rates reported to be <1% to 1.5%. At the same time, the overall complication rates in PCNL have been reported to be as high as 83% with a 15% to 20% major complication rate. 1,13,24 –26 FURSL has become the procedure of choice in patients in whom other modalities have failed and is a viable alternative for patients with obesity, anatomic deformity such as kyphoscoliosis, and in pregnancy. 4,7,10,22
The use of a ureteral access sheath facilitates easy passing of the ureteroscope, allows the removal of stone fragments, allows additive benefit of protecting the ureter from repeated insertion and removal of the scope, in addition to decreasing the intrarenal pressures during prolonged procedures by maintaining continuous drainage. 6,11 This review found that 86% of the FURSL procedures were ureteral sheath-assisted. It is worth noting that the two studies that did not use a ureteral access sheath were Grasso and associates 8 and El-Anany and coworkers, 12 published in 1998 and in 2001 respectively, while the first article published on assessing ureteral access sheath use was in 2001. 28 Therefore, it is safe to say this technology was not readily available at the time these two studies were conducted.
None of the studies predefined the meaning of minor or major complications. The reviewing authors, however, considered minor complications as those that would settle on their own or with minimal support or a grade I of the Clavien-Dindo classification—ie, self-limiting hematuria or urinary tract infection necessitating antibiotics or analgesic 27 —while major complications are those that needed either further procedures or close monitoring, classified as grade II or above of the Clavien-Dindo classification—ie, perforation, obstructive pyelonephritis, steinstrasse, or subcapsular hematoma.
Furthermore, a major discrepancy between the studies was the definition of the SFR. Two studies defined it as fragments <1 mm; however, the same lead author conducted both these studies. 7,11 The majority of the studies considered stone free as those 2 mm and below. 4 –6,8,10,12 In addition, Hyams and associates 13 subdivided the stone-free groups into those who are truly stone free, those who had a 0 to 2 mm retained fragment, and those with <4 mm retained fragment.
With regard to the subgroup analysis, although not all the studies were grouped for a meta-analysis, it is evident from the studies that FURSL has a high SFR in stones 2 to 3 cm compared with stones >3 cm. The SFR, however, decreased with the increase in stone size; furthermore, higher numbers of procedures were needed to achieve stone clearance with a rising risk of major complications.
Strengths and weaknesses of the study
The strength of the study remains the systematic approach taken to review the last 21 years of literature reporting on patients undergoing FURSL for large renal stones. The quality of the evidence was assessed using a validated instrument. Two independent researchers (not involved in any of the studies) performed data extraction to minimize potential for bias. Outcome parameters were predetermined and data were extracted using standard forms. An obvious weakness of all systematic reviews is that they depend on and reflect the evidence from the available primary studies and may not always be in a position to provide specific guidance on interventions as a result. The weaknesses of our conclusions are therefore closely linked to the weaknesses in the individual studies. These nonrandomized studies were potentially prone to large bias in patient selection, outcome assessment, and reporting.
Limitations and future areas of research
One of the limitations of this review was that all the included studies were retrospectively conducted. Full description of the methodology, however, was delineated in all the studies, which might be construed as lowering the risk of bias. Despite these limitations, all the studies had similar comparative parameters, which allowed for a meta-analysis of the data to formulate a more figurative result as well as a subgroup analysis. Another limitation is that the SFR was defined differently in studies. All the studies were from high-volume centers of excellence with procedures performed by trained experienced endourologists, and such high SFR may not be achievable in centers in which there is less experience.
Further research is vital to evaluate the role of URS and laser fragmentation of large urinary stones. Furthermore, a multicentric randomized trial comparing FURSL with PCNL for treatment of stones larger than 2 cm needs to be conducted. The parameters should ideally encompass operative times, number of procedures per patient, length of hospital stay, number of clinic or emergency department visits, SFRs, and complication rates. These parameters need to be explicitly defined. In addition to this, a cost analysis comparison between the two groups should also be performed. The complications should be classified into a known system, such as the Clavien-Dindo classification for surgical complications. 27
Conclusion
Although PCNL remains the gold standard, FURSL can successfully treat patients with stones larger than 2 cm with a high SFR and a low complication rate. The results of observational cohort studies, however, are from high-volume experienced centers and may not be sufficient to alter everyday routine practice; this review has shown that the efficacy of FURSL allows an alternative to PCNL. Because this high SFR may not be reproducible, an informed treatment decision should be made with the patients based on the outcomes for FURSL of the surgeons/centers.
Footnotes
Disclosure Statement
No competing financial interests exist.