
Abstract
Background and Purpose:
While nephroureterectomy (NU) remains the gold-standard treatment for upper-tract carcinoma in situ (UT-CIS), it may be unnecessarily aggressive in comparison with the treatment of bladder CIS. Upper-tract administration of bacillus Calmette-Guérin (BCG) has shown promise for UT-CIS, but with limited reports and varied results. Furthermore, all previous reports included patients with positive cytology results without biopsy-proven CIS, or combined BCG with other topical therapies that are used for bladder CIS. We report our experience using a novel technique to directly instill BCG with interferon-α2B (BCG/IFN) into the upper-tract in patients with biopsy-proven UT-CIS.
Patients and Methods:
Patients who received a diagnosis of isolated, biopsy-proven UT-CIS from September 2003 to January 2012 were included. After biopsy, all patients received a 6-week induction course of BCG/IFN, administered via an open-ended ureteral catheter. Initial follow-up was scheduled 1 month after the completion of the intrarenal therapy and consisted of flexible ureteroscopy, selective urinary cytology, retrograde pyelography, and rebiopsy of the upper tract. Complete response (CR) was defined as the absence of visualized lesions on ureteroscopy, negative selective cytology results, and absence of clinical progression. Absence of visualized lesions with persistently positive cytology results or persistence of lesions after induction was considered no response (NR). New upper-tract lesions after an initial CR were considered recurrences. Patients with a CR were placed on maintenance therapy for 2 years. Surveillance was performed every 3 months with ureteroscopy, selective cytology, and imaging.
Results:
Eleven patients (mean age=73 years) were followed for a median of 13.5 months (3.7–103.3 mos). Eight patients had an initial CR, while three initially had NR. Two of the NR patients had negative biopsy results but persistently positive cytology results; both of these patients underwent a second induction course and achieved a CR. The third NR patient had persistence of lesions after induction and was offered a nephroureterctomy. Total kidney preservation rate was 91% (10/11). There were no treatment-related adverse events.
Conclusion:
This study demonstrates the safety and efficacy of intrarenal BCG/IFN maintenance therapy for patients with UT-CIS. Unlike other mechanisms of delivery, including percutaneous administration or reflux via double pigtail stents, this office-based technique spares the morbidity of a chronically indwelling nephrostomy tube or ureteral stent.
Introduction
Traditionally, chemotherapeutic agents (eg, mitomycin C, epirubicin) and immunomodulatory agents (bacillus Calmette-Guérin [BCG], interferon [IFN]) are instilled directly into the bladder as adjuvant therapy for non–muscle-invasive bladder cancer and have been shown to prevent tumor recurrence and progression. 5 This concept was subsequently expanded to the treatment of UTUC, although for patients with high-grade lesions, such as carcinoma in situ (CIS), the gold standard treatment remains NU. This is in stark contrast to the treatment of urothelial cancer of the bladder, where intravesical therapy can be a first-line treatment option for high-grade non–muscle-invasive tumors, including CIS. 6
There are limited reports in the literature of using BCG monotherapy as primary treatment for upper-tract CIS (UT-CIS), and these studies have varied outcomes and limited long-term results. The reports also describe various techniques of BCG administration that either necessitate an indwelling ureteral stent and/or percutaneous nephrostomy tube. In addition, the presumptive diagnosis of UT-CIS in these studies was made exclusively cytologically. To our knowledge, there are no reports in the literature on UT-CIS where the diagnosis was confirmed with biopsy or where routine ureteroscopy and biopsy were used as part of the follow-up protocol. Furthermore, there are no reports that use combination therapy with BCG and IFN to treat UT-CIS.
In this study, we present our experience in treating ureteroscopic biopsy-confirmed UT-CIS with intrarenal BCG/IFN, using an office-based retrograde technique of administration.
Patients and Methods
Patients
Our Institutional Review Board-approved patient database was retrospectively reviewed to identify all patients with isolated, biopsy-proven UT-CIS who were treated with BCG-Interferon-α2B (BCG/IFN) from September 2003 to January 2012. Patients with concomitant upper-tract papillary and/or invasive lesions or bladder cancer were excluded. Nonextirpative therapy was electively performed in all patients. Demographic data and patient characteristics were collected, including incidence of previous urothelial cancer and related treatments. All patients underwent initial ureteroscopic evaluation in the operating room under general or regional anesthesia. The entire upper tract was examined with a combination of semirigid and flexible ureteroscopy. Narrow band imaging technology was routinely used from the time it became available in our operating room suites and was used to aid in identifying suspicious lesions. Ureteroscopic biopsy samples were taken from all suspicious lesions using the Piranha biopsy forceps (Boston Scientific, Natick, MA). In addition, random biopsy samples were taken from other calices and segments of the ureter to ensure sampling of the entire upper tract.
Diagnosis of CIS was confirmed by ureteroscopic biopsy in all patients. Detailed mapping of the upper tracts, including biopsy sites, was notated for each patient. This was to ensure that subsequent ureteroscopic imaging and biopsy locations would remain consistent. After initial endoscopic diagnosis of UT-CIS, the patients were transitioned to the office for BCG/IFN treatment.
Technique of BCG-IFN delivery
Our office-based technique of intrarenal BCG/IFN has been described previously. 7 Briefly, flexible cystoscopy is performed with 2% intraurethral lidocaine jelly as anesthesia, and the ureteral orifice is cannulated with a 0.038″ guidewire. A 5F open-ended ureteral catheter is then advanced over the wire into the renal pelvis and the distal end secured to the patient's thigh. Retrograde pyelography is performed to confirm proper positioning of the catheter in the renal pelvis and to make sure that for each patient, the catheter is placed in the same location at every visit. Using a Buretrol volume control chamber (Baxter, Deerfield, IL), the BCG/IFN formulation (40 mg Tice BCG + 50 million units of IFN-α2B in 50 mL of sterile saline) is infused under low pressure gravity drip, at a rate of 1 mL/min, for a total instillation time of 1 hour. To prevent any increased intrarenal pressure, the Buretrol chamber was never located more than 20 cm above the level of the kidney. After completion of the infusion, the ureteral catheter is removed, and the patient is instructed to retain the fluid for an additional hour before voiding. All patients have confirmation of sterile urine before instrumentation.
Definitions of treatment response
Complete response (CR) was defined as the absence of visualized lesions on ureteroscopy, negative selective cytology results, and absence of clinical progression on imaging. A no response (NR) was defined as either complete absence of lesions with persistent positive selective cytology results or actual persistence of upper-tract lesions after completion of induction therapy. Recurrence was defined as evidence of new biopsy-proven upper-tract lesions after an initial CR. Progression was defined as tumor of a higher grade and/or stage.
Treatment schedule and follow-up
BCG/IFN was administered in 6 weekly instillations. Initial follow-up was scheduled 4 to 6 weeks after the completion of the intrarenal therapy and consisted of flexible ureteroscopy, selective urinary cytology, retrograde pyelography, and rebiopsy of the upper tract. The previously diagrammed map of the renal pelvis, which was created at the time of initial diagnosis, was used to aid in follow-up biopsy to ensure the same area of urothelium was being sampled. Patients with an initial CR were placed on a standardized maintenance schedule that included 3 weekly instillations of BCG/IFN at 3, 6, 12, 18, and 24 months. Patients on maintenance therapy continued to be monitored at 3-month intervals with ureteroscopy, biopsy, and selective cytology. In addition, patients underwent surveillance CT imaging every 6 months.
Patients with NR because of persistence of positive cytology results at initial follow-up were offered a second induction course with intrarenal BCG/IFN; if CR subsequently occurred, they were then started on maintenance therapy. Patients who had a NR because of persistence of upper-tract lesions, however, were offered definitive surgical therapy with NU.
End points and statistical analysis
The primary end points to be analyzed were the presence of a complete response to intrarenal therapy as well as recurrence-free survival. Secondary end points included overall survival, disease-specific survival, therapy subsequent to intrarenal management, as well as renal preservation. Recurrence-free, progression-free survivals were calculated from date of initial BCG/IFN instillation to date of first recurrence or progression, respectively. Disease-specific survival was calculated from date of initial BCG/IFN instillation until date of death from progressive UTUC. Overall survival was calculated from date of initial BCG/IFN instillation until date of death from any cause. Patients free of recurrence were censored at date of last follow-up appointment. Survival estimates were calculated by the Kaplan-Meier method. All statistical analysis was performed on Stata 11.0 (StataCorp LP, College Station, TX).
Results
Eleven patients with isolated, biopsy-proven UT-CIS underwent intrarenal instillation of BCG/IFN between 2003 and 2012 as definitive, primary treatment. Baseline patient demographics are summarized in Table 1. Mean age of the patients was 73 years (59–90 years). Median length of follow-up was 13.5 months (3.7–103.3 mos). Median serum creatinine level at time of diagnosis was 0.85 mg/dL (0.7–1.2 mg/dL). Nine (82%) patients had a history of bladder cancer and had been treated with transurethral resection in the past; five of the nine patients previously received intravesical BCG, but none of the patients received BCG/IFN previously. One of the patients had evidence of residual bladder cancer at the time of upper-tract management; this, however, was not an exclusion criterion.
BCG/IFN=bacillus Calmette-Guérin/interferon-α2B.
Eight (73%) patients experienced an initial CR, while three (27%) patients had an initial NR. Of the nonresponders, two (18% of total group) patients had negative ureteroscopic biopsy results but were classified as a NR because of a positive selective cytology report. The third patient (9% of total group) with an initial NR was classified as such because of follow-up biopsy results that were positive for CIS.
All eight patients with an initial CR remained disease-free for the length of follow-up. Of the three patients with NR, the two with persistence of positive cytology results alone subsequently underwent a second 6-week induction course of BCG/IFN. One was successfully converted to a CR, initiated on maintenance therapy, and remained free-of-recurrence during the follow-up period. The other patient initially experienced a CR, which lasted for more than 1 year, but after being treated with steroids for severe degenerative disc disease and gross hematuria developing, this patient was found to have recurrent CIS. At this point, the patient was started on intrarenal mitomycin C treatment. The patient eventually expired 2 years later as a result of multiple medical comorbidities; death was unrelated to cancer. Finally, the NR patient with persistence of a biopsy-proven CIS lesion after induction therapy underwent NU with the final pathology report revealing CIS of the proximal ureter without extraureteral extension and negative lymph nodes. Results are detailed in Table 2.
Overall, nine (82%) patients had a CR, one (9%) patient had NR, and one (9%) patient experienced a recurrence. Total kidney preservation rate was 91% (10/11). Overall survival rate was 91% with a disease-specific survival of 100% (Fig. 1). Therapy was well tolerated in all patients and there were no treatment-related adverse events reported.
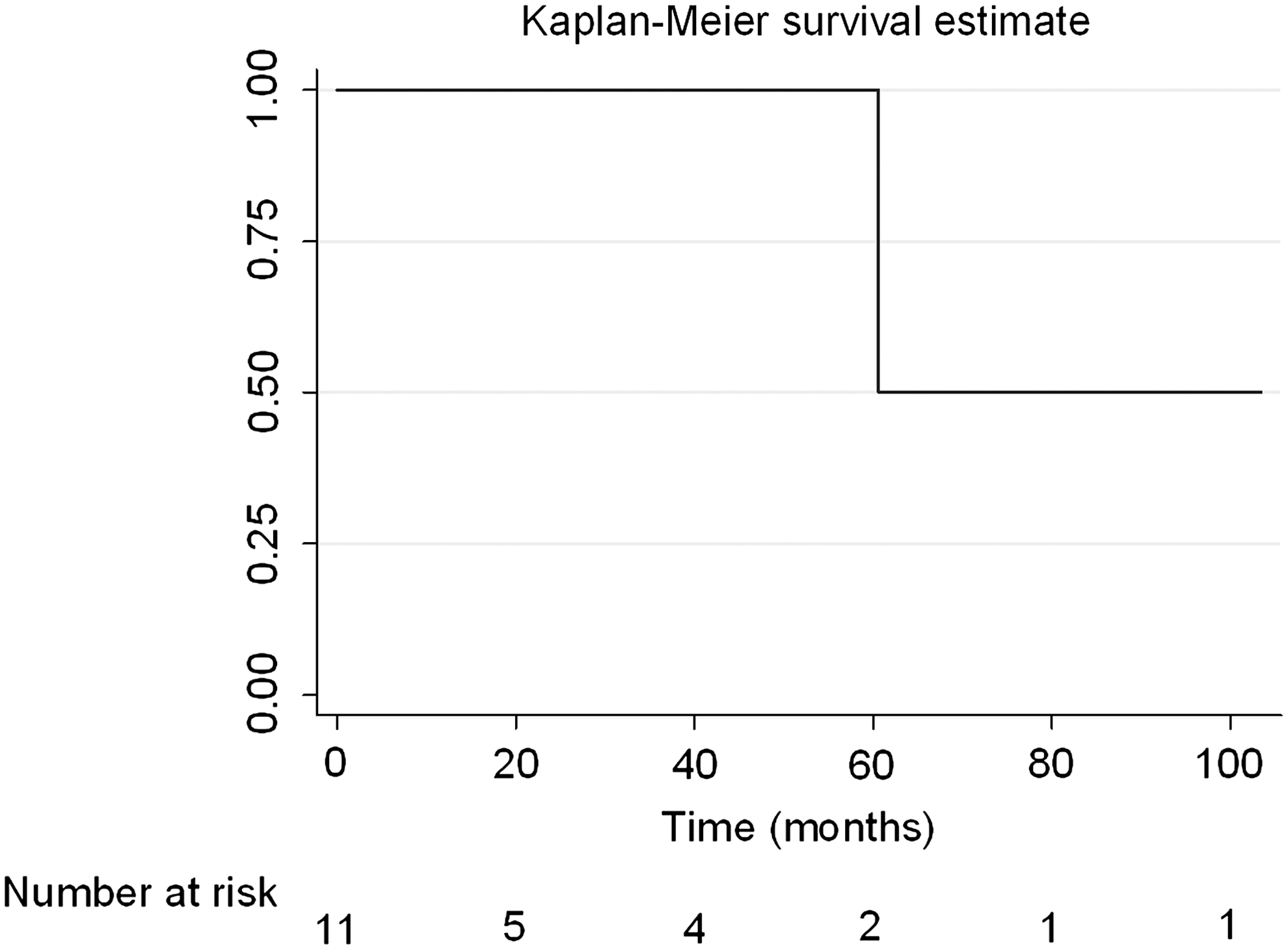
Kaplan-Meier survival estimate.
Discussion
NU remains the reference standard for UTUC, including CIS, resulting in definitive control of ipsilateral local recurrence. In cases where preservation of renal function is imperative, however, such as renal insufficiency, solitary kidney, or bilateral synchronous tumors, nephron-sparing endoscopic techniques can be used. In the current era of minimally invasive techniques, some patients may opt for a less invasive approach, even when the contralateral kidney is normal. Unfortunately, endoscopic ablation is not a successful therapeutic approach for UT-CIS.
Intravesical BCG has been widely accepted as a first-line treatment option for the management of bladder CIS, 8 but it was not used in the management of UT-CIS until 1985 when Herr 9 first reported its role for this disease. Over the past 25 years, there has been a growing number of reports that have consistently shown a reduction in tumor recurrence and progression of UT-CIS with BCG monotherapy. 10 –18 In fact, upper-tract BCG therapy appears to be more efficacious for UT-CIS than for Ta/T1 lesions. 19,20 Although this modality was initially reserved for patients who were not surgical candidates, recent reports have suggested that upper-tract instillation with BCG may be appropriate even when used electively. 14,17 Yet, on the whole, there are still only limited reports with a collective total of approximately 100 patients.
The vast majority of these reports are limited in several areas. First, most lack long-term outcomes. Perhaps more importantly, all previously published reports on UT-CIS use cytology alone to diagnose CIS. Specifically, these articles define UT-CIS as the presence of selective upper-tract cytology in the setting of negative random bladder and urethral biopsy results. Furthermore, the majority of previous reports use cytology as the primary component of surveillance protocols; only one study used ureteroscopy as well. 14 This is in stark contrast to the management of bladder CIS where the diagnosis is pathologically confirmed and routine cystoscopic surveillance is used in addition to the use of urine cytology. In the present study, all patient diagnoses were based on biopsy, and to our knowledge, this is the first time a biopsy-confirmed cohort of patients with isolated UT-CIS has been studied. In addition to the use of ureteroscopy for diagnostic purposes, this study also represents the first time that the routine use of ureteroscopy was a key component of surveillance, mimicking the treatment paradigm of bladder cancer.
The current study confirms the utility of BCG for UT-CIS, with 82% of the patients having a durable CR and with a 91% rate of kidney preservation. There was only one (12%) patient who experienced a recurrence. This is drastically lower than other reports that have recurrence rates as high as 40% to 50%. 14,17,19 This includes a recently published report by Giannarini and associates 19 who have the largest patient cohort of UT-CIS with the longest follow-up. In that study, which is an update of the authors' experience with 42 renal units treated with upper-tract BCG, the authors report a 40% recurrence rate. In addition to our reassuring recurrence-free rates, these results appear to be more durable than previous studies. Overall, the mean duration of negative cytology results across published reports, which is used as a surrogate for response, has been less than 2 years. 13 In contrast, of the patients in the present study who had a CR or partial response, all have been disease free for a mean of more than 2 years.
There are several possible explanations for our improved results. One possible reason is the addition of IFN, which was not administered in any of the previous studies. IFN has been shown to increase the recurrence-free rates of bladder CIS compared with BCG alone and was therefore chosen to be administered in our patients in combination with BCG. 21 To our knowledge, this is the first study to report long-term results on the use of combination BCG/IFN for UT-CIS. Another possible explanation for our favorable long-term results is the use of maintenance therapy, on a schedule similar to the one proposed by the Southwest Oncology Group for bladder CIS. 22 Maintenance therapy was selected because previous reports have shown occurrences of both disease progression and recurrence in patients who initially had a negative urine cytology result after initial intrarenal BCG therapy. Another key difference in our study is that all of our patients were electively managed endoscopically despite being appropriate surgical candidates. Therefore, these patients may represent a healthier cohort than those in the other reports that include many patients who were managed nonsurgically because of imperative indications and medical comorbidities.
A final possible explanation for the positive results may be that our technique of upper-tract instillation is more effective. There are varied techniques in the literature by which BCG has been administered to the upper tract. The first method is antegrade instillation through a percutaneously placed nephrostomy tube. This, however, necessitates chronic placement of a nephrostomy tube, which is invasive and has associated comorbidities that negatively impact the patient's quality of life. Furthermore, this method has the potential for renal granuloma, or seeding the tract with cancerous cells, although there are controversial reports regarding the likelihood of these sequelae. 23
The second method is retrograde instillation into the bladder in the presence of a Double-J indwelling stent or after iatrogenic creation of ureteral reflux. The third method is using an open-ended ureteral catheter, which is temporarily placed in a retrograde fashion. Only the open-ended ureteral catheter technique allows for constant and predictable contact between the BCG and the upper-tract urothelium. In contrast, the other retrograde methods rely on reflux to adequately reach the upper tract. Similarly, with the antegrade method, the BCG is likely to drain directly into the ureter, resulting in an unpredictable contact pattern with the remainder of the collecting system. A final advantage of the open-ended catheter method is that it allows for the easy collection of selective upper-tract urine for cytologic evaluation.
The current study utilized this form of retrograde instillation, but in a modified manner, using a Buretrol volume control chamber. This novel technique allows for continual topical exposure of the urothelium at low pressures, thereby minimizing the risk of systemic absorption of the BCG and/or sepsis. Although this technique necessitates repeated insertion of a ureteral catheter, this was accomplished as an office-based procedure in all of our patients, who tolerated this without complication.
Fortunately, none of our patients experienced any adverse effects of the BCG, although it is unclear whether our novel technique impacted this. The most commonly reported complications in the literature include urosepsis from gram-negative organisms, granulomatous changes, ureteral strictures, and symptoms of systemic BCG absorption.
On the basis of our findings, we recommend the use of upper-tract instillation of BCG/IFN combination therapy as a possible first-line therapy in patients with isolated UT-CIS, even in the absence of imperative indications for nephron-sparing management. In addition, routine use of maintenance therapy should be used for patients who have a CR to induction therapy. This treatment appears to be safe and efficacious, with reassuring long-term results. Furthermore, the routine use of ureteroscopy for surveillance may detect disease progression and/or recurrence at an earlier time point than cytology alone. This may result in conversion to surgical treatment at an earlier time frame, which could potentially result in advantageous survival outcomes. For example, one of the patients in our study who had NR to BCG/IFN had ureteroscopic evidence of a suspicious erythematous lesion after induction therapy despite converting to negative selective cytology results. If cytology alone was used to follow patients, this patient would have been misclassified as a treatment success, and definitive therapy would have been delayed.
The major limitations of the study include the small number of patients and retrospective nature. Prospective comparisons with other modes of BCG/IFN delivery should be performed before the oncologic superiority of one method can be established.
Conclusions
Upper-tract administration of BCG/IFN combination therapy can be successfully used with curative intent in patients with UT-CIS, especially when renal preservation is desired. Retrograde instillation is a feasible and effective technique of delivery, with satisfactory long-term oncologic results that parallel those for surgical intervention. Appropriate patient selection as well as close postoperative surveillance with routine ureteroscopic and cytologic evaluation is of paramount importance.
Footnotes
Acknowledgments
Michael Lipsky is supported by a grant from the Doris Duke Charitable Foundation and by the Einstein Research Fellowship.
Disclosure Statement
No competing financial interests exist.