
Abstract
Purpose:
To compare outcomes between patients undergoing surgical and percutaneous cryoablation for treatment of renal masses and identify prognostic variables that determine survival.
Patients and Methods:
We retrospectively evaluated the medical records of 194 patients who underwent cryoablation for renal tumors between 1997 and 2008 at a single large center. Patient demographics, tumor characteristics, perioperative data, and follow-up details were recorded. Univariate and multivariate Cox proportional hazards analysis was performed to identify predictors of overall (OS), cancer-specific (CSS), and recurrence-free survival (RFS).
Results:
Cryoablation was performed percutaneously (PCA) in 141 patients for 154 tumors, while 53 patients were treated surgically (SCA) using an open or laparoscopic approach for 54 tumors. Mean follow-up was 44.5 months in SCA and 36.1 months in PCA. PCA had a shorter duration of hospital stay (0.7 days vs 3.2 days, P<0.0001). The rate of residual (P=0.38) and recurrent disease (P=0.18) was not significantly different between the two groups. Five-year OS, CSS, and RFS were 78.81%, 100%, and 85.23% for SCA, and 77.71%, 98%, and 95.56% for PCA, respectively; the type of approach was not predictive of OS, CSS, and RFS.
Conclusions:
SCA and PCA both provide adequate oncologic control for renal masses. Duration of hospital stay was lower in patients undergoing PCA.
Introduction
Cryoablation can be performed either surgically (open/laparoscopic) or using a percutaneous approach. Because there are no strict published guidelines, the decision to use surgical cryoablation (SCA) or percutaneous cryoablation (PCA) for tumor ablation largely rests on the anatomic location of the tumor, comorbidity profile of the patient, and surgeon discretion. Anterior and medially situated tumors are preferably ablated surgically whereas a percutaneous approach is used in lateral and posterior tumors, which are easily accessible through the skin.
The comparative efficacy of the two approaches for renal tumor ablation has been studied by a few groups. 6 –9 The sample sizes of these studies, however, are relatively small and the follow-up duration is short. We present our experience with surgical and percutaneous renal cryoablation and report intermediate-term oncologic outcomes and evaluate the factors that influence these outcomes. To our knowledge, we report the largest comparative series of renal cryoablation with an intermediate-term follow-up published in the literature.
Patients and Methods
After obtaining the approval of our local Institutional Review Board, we retrospectively examined the medical records of patients who underwent renal cryoablation as a primary treatment at our hospital from 1997 to 2008. The variables studied included patient demographics, pertinent laboratory values, perioperative details, and follow up data. The Charlson Comorbidity Index (CCI) was used to compare the comorbidity profile of the patients. 10 Renal function was assessed by calculating the glomerular filtration rate (GFR) using the Chronic Kidney Disease-Epidemiology Collaboration equation. 11
Changes in GFR were calculated on day 1 postoperatively and on long term through scheduled clinic visits. The technique used for SCA has been described by various authors. 12,13 Cryoablation was performed under general anesthesia using an argon-based cryoablation system (Endocare, Irvine, CA). A sequential dual freeze-thaw cycle was used. Intraoperative ultrasonography was used for confirmation of effective cryoprobe placement and adequate ice-ball formation at least 1 cm beyond the edge of the tumor. We have described our technique for PCA earlier. 5 Cryoprobes are deployed under CT fluoroscopic guidance ensuring appropriate intratumoral placement and adequate tumor ablation. An intraoperative biopsy was performed to confirm tumor pathology.
Follow-up
Patients were followed up after cryoablation and evaluated for any evidence of recurrence/residual tumor using contrast-enhanced CT. We used a standardized 3 monthly follow-up schedule for the duration of the study. At each visit, patients underwent relevant laboratory workup along with CT scans (or MRI scans). Residual disease was defined as persistent enhancement on the first follow-up imaging study performed 3 months after cryoablation and recurrent disease as a new hyperenhancing/enlarging tumor nodule after an initial negative imaging study. 14 Patients with positive results on scans were offered additional extirpative/ablative therapies. Patients who had no evidence of recurrent/residual disease were seen on an increasingly longer interval after a few negative scans. We did not routinely perform postoperative biopsies to confirm tumor recurrence as a part of the follow-up schedule. Biopsies were performed, however, wherever deemed fit to confirm the diagnosis in suspicious lesions. Recurrence-free survival (RFS) was defined as negative radiographic evidence of disease at the cryoablation site. Overall survival (OS) was defined as the interval from cryosurgery to death from any cause. Cancer-specific survival (CSS) was defined as absence of death from renal cancer.
Statistical analysis
Statistical analysis was performed using STATA, version 10.1. A P value of less than 0.05 was considered statistically significant. Comparisons between the two subgroups of patients were performed using chi-square tests for categorical variables and Student t test for continuous data. OS, CSS, and RFS probabilities were estimated using Kaplan-Meier analysis. Survival curve differences were evaluated using log-rank test. While all patients undergoing cryoablation were included for OS, only those patients who were confirmed to have renal cell carcinoma on biopsy were included for CSS and RFS. Also, rates of recurrence and residual disease were also calculated only among patients with confirmed renal carcinoma on histologic examination. Risk factors for recurrence and death were analyzed using the Cox proportional hazards model.
Results
A total of 194 patients with a mean follow-up of 38.14±25.29 months underwent cryoablation for 207 renal tumors at our institution. The demographic features, tumor characteristics, and the perioperative details of patients in the two groups are summarized in Table 1. The complication profile of cryoablative treatment performed at our center has been reported. 15 On comparison with SCA, the PCA cohort had a lower immediate postoperative GFR (62.0 vs 73.3 mL/min/m2, P=0.02), but no statistical differences were seen for percentage change in GFR on postoperative day 1 (P=0.66) and time of last follow-up (P=0.72). Furthermore, the PCA cohort had a significantly shorter duration of hospital stay (0.7 days vs 3.2 days, P<0.0001). In the surgical group, the subset of patients undergoing open cryoablation (n=7) stayed in the hospital for a mean of 5.1 days compared with patients undergoing laparoscopy who stayed for an average of 2.8 days.
Charlson Comorbidity Index was calculated using the parameters described in the original publication.10
Glomerular filtration rate has been calculated using Chronic Kidney Disease-Epidemiology Collaboration equation.11
USG=Ultrasonography; GFR=glomerular filtration rate; AML=acute myeloid leukemia.
At the time of last follow-up, 11 SCA (21.15%) patients and 23 PCA (16.3%) patients had died. Of the 160 patients alive at the time of last follow-up, 144 had rigorously adhered to the follow-up schedule while 16 patients were lost to follow-up. The survival distributions of the two sample groups were determined to be statistically nonsignificant on log rank test. Figure 1 depicts the comparative Kaplan Meier OS (log rank P=0.70), CSS (log rank P=0.48), and RFS (log rank P=0.75) curves while Figure 2 shows the curves for the whole cohort. Table 2 outlines the survival data of the two groups. Multivariate proportional hazards models (Table 3) revealed that CCI (P=0.04) and duration of hospital stay (P=0.001) were independent predictors of OS. Interestingly enough, the type of treatment received was not found to predict OS, CSS, or RFS.

Kaplan-Meier curves for comparative overall, cancer-specific, and recurrence-free survival for surgical cryoablation (SCA) and percutaneous cryoablation (PCA).
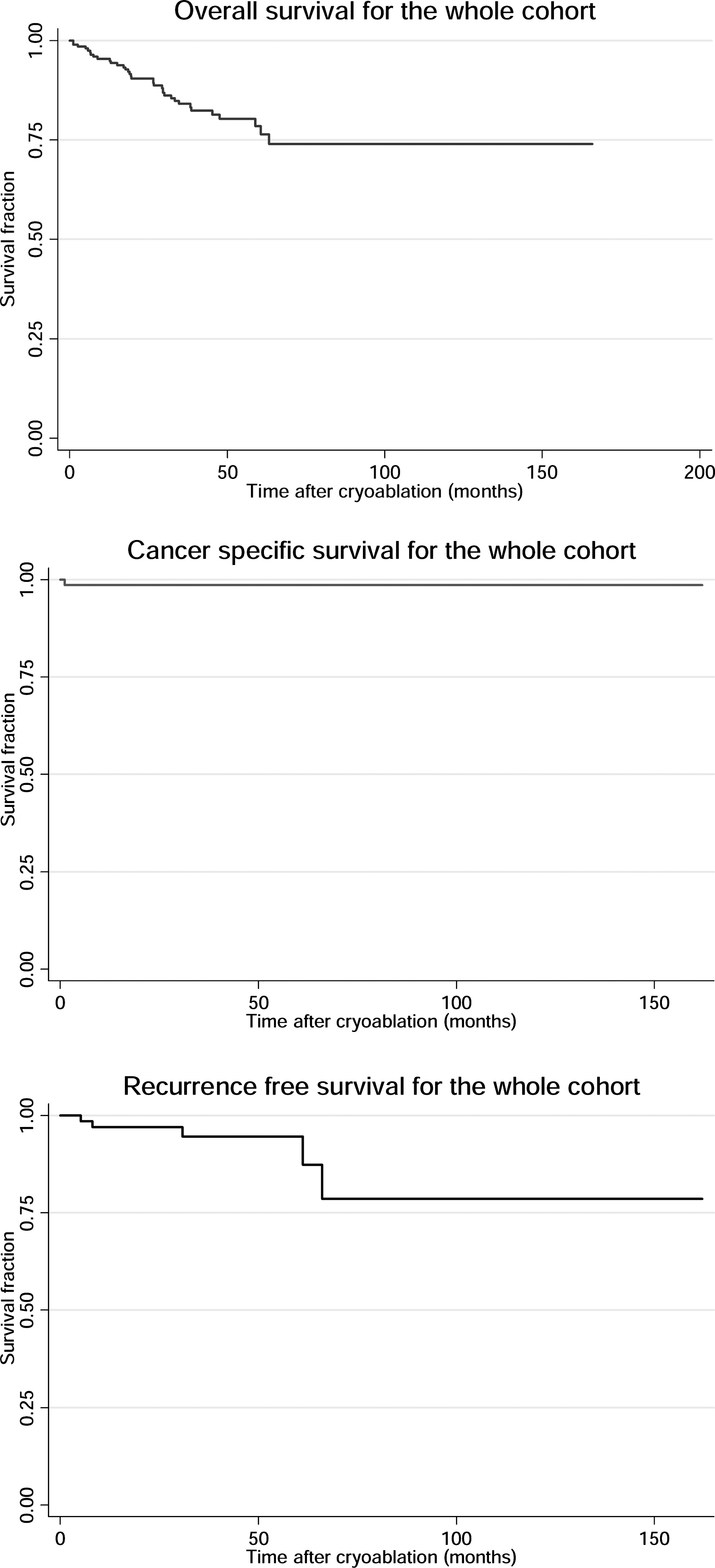
Kaplan-Meier curves for overall, cancer-specific, and recurrence-free survival of the whole treatment cohort.
SCA=surgical cryoablation; PCA=percutaneous cryoablation; CI=confidence interval.
OS=overall survival; CSS=cancer-specific survival; RFS=recurrence-free survival; HR=hazards ratio; CCI=Charlson Comorbidity Index; GFR=glomerular filtration rate.
Table 4 lists the patients in whom residual/recurrent disease developed after cryoablation. Postcryoablation follow-up imaging revealed 12 patients with residual disease in whom a successful ablation could not be achieved in a single operative setting. Eleven of these patients had been operated on percutaneously of whom 7 were confirmed renal-cell carcinoma while one was performed laparoscopically (13.72% vs 4%, P=0.38). A subsequent PCA was performed in 10 of these patients, 9 of whom remain disease-free until the time of last follow-up. One patient was lost to follow-up after repeated cryoablation. Two patients with small residual tumors opted for continued surveillance. In one patient, the tumor size has remained stable for up to 2 years. The second patient, however, had a rapid increase in tumor size and died 30 months postcryoablation.
Cryo=cryoablation; PCA=percutaneous cryoablation; RCC=renal cell carcinoma; NED=no evidence of disease; LCA=laparoscopic cryoablation; RN=radical nephrectomy; OCA=open cryoablation.
Local recurrence of disease was discovered in three SCA (12%) patients and two PCA (3.92%) patients on follow-up (P=0.18). Also, distant metastases developed in one patient each (1.9% and 0.6%, respectively, P=0.42). Four of these patients with recurrent tumors underwent a subsequent cryoablation, three of whom were disease free at the time of last follow-up while lung cancer developed in the fourth patient. The fifth patient was lost to follow-up, whereas in the sixth patient (treated by laparoscopic cryoablation [LCA]), developed a local recurrence of disease developed along with widespread metastases 5 years later. Osseous metastatic disease also developed in a PCA patient 13 months after cryoablation, and he succumbed to the disease 4 months later.
Discussion
Cryoablation was initially offered as a minimally invasive nephron-sparing option for patients who were not considered ideal candidates for partial nephrectomy. 3,12 It has been shown to minimize morbidity, providing cancer control matching that of surgery while being considered technically less challenging. 1,13,16 Emerging evidence regarding the short- and intermediate-term oncologic efficacy of cryoablation has been instrumental in advancing its clinical application regardless of tumor characteristics and patient morbidity. 17 Many groups have investigated the relative efficacy of cryoablation and partial nephrectomy and have found these techniques to be similar in terms of morbidity and oncologic and functional outcomes. 18 –20 Partial nephrectomy, however, is still considered gold standard for tumor extirpation.
PCA has certain definitive advantages over SCA in the form of clear visualization of the tumor depth under CT guidance, lower morbidity, decreased pain, shorter hospitalization, and the ability to perform the procedure under moderate sedation. 3,5 Conversely, surgical cryotherapy confers the advantage of direct visualization along with allowing tumor ablation of sites not amenable percutaneously. The comparative oncologic efficacy of the two treatment approaches has been reported by a few groups. 6,8,9 Through this study, we have attempted to share our experience and identified prognostic indicators that influence long-term outcomes, the results of which can be used as a guide to make treatment decisions.
Our results show that PCA patients could leave the hospital sooner than surgical patients. These results are consonant with our PCA protocol whereby we treat a substantial proportion of our patients on an outpatient basis under moderate sedation, discharging them on the same day. Interestingly, both procedures were found to have minimal deleterious effects on renal function.
The aggregate oncologic outcomes in the entire cohort are very favorable with 5-year OS, CSS, and RFS of 78.52%, 98.65%, and 94.57%, respectively. These rates are in concert with those reported by other studies with similar follow-up. 16 The 5-year OS, CSS, and RSS from our study were 78.81%, 100%, and 85.23% for SCA, and 77.71%, 98%, and 95.56% for PCA, respectively (Table 2). Encouraging results have been reported earlier by many groups who described a 3-year CSS of 100% for patients undergoing LCA and PCA. 2,9,12 We report 5-year cancer-specific survival probabilities of 100% and 98% for SCA and PCA that match the results reported by these series. This further substantiates the oncologic efficacy of both cryoablative approaches.
On examining the risk factors for death, mean CCI emerged as an independent prognostic indicator of OS. This significant, yet nonsurprising result is important because patients with considerable comorbidities face a higher chance of death from all causes. Moreover, duration of hospital stay was also found to be independently predictive of OS. A longer hospital stay was usually needed in the event of perioperative complications or in patients with multiple comorbidities necessitating longer recovery, both of which might contribute to reduced survival.
Our study found SCA and PCA to be equivalent in oncologic control when assessed for recurrence of disease (12% vs 3.92%, respectively, P=0.18). A key meta-analysis performed by Long and associates 21 to compare oncologic efficacy of SCA and PCA found no difference for tumor recurrence between the two cryotherapy modalities (1.4% and 1.1%, respectively, P=0.44). Although the rate of residual disease was higher in PCA patients (13.72% vs 4%), the difference was not statistically significant (P=0.38). Intriguingly, however, higher rates of incomplete tumor ablation in percutaneous patients compared with laparoscopic patients have been reported by other groups. 7,22,23 The relatively higher rate noticed in PCA patients might be because while LCA allows a precise number of probe placements from direct visual feedback, the same might be more difficult to achieve in percutaneous procedures.
Aggressive postablation radiographic follow-up allows early detection of any recurrent lesions and if deemed essential, allows subsequent intervention. All patients in whom residual/recurrent disease (without metastases) developed and who opted for re-treatment had returned to a disease-free state at the time of last follow-up except one patient who was lost to follow-up. A recent meta-analysis found that on considering secondary treatment outcomes, the two techniques did not demonstrate any statistical difference (95% vs 92%, P>0.05). 24
We currently offer cryoablation as a first-line treatment option (along with partial nephrectomy) for small renal masses in patients with a higher comorbidity profile. Our study is one of the largest series with an intermediate follow-up published in the literature that provides comparative oncologic outcomes of renal tumors treated with SCA and PCA at a single center. Our study validates the efficacy and safety profile of renal cryoablation and can be used as a guiding tool for making treatment decisions for patients seeking cryoablative therapy.
Certain limitations of our study deserve to be mentioned. Our study has a retrospective nonrandomized design and is thus prone to selection bias. Furthermore, the patient sample sizes are unequal in the two cohorts. This is in part because although our early experience with cryoablation began with surgical techniques, increasing expertise, lower morbidity, and shorter convalescence period associated with PCA has made us more aggressive in choosing PCA over SCA in the recent past. Also, this study is from a single center with limited sample size and intermediate follow-up. Our study is also limited by the absence of histologic diagnosis in a significant proportion of our patients. Our results require validation, preferably in a large multicenter design with a longer follow-up, allowing a more robust analysis with greater statistical power.
Conclusions
PCA and SCA are both viable procedures for treatment of patients with renal tumors with similar oncologic efficacy on intermediate-term follow-up. Although duration of hospital stay is lower in percutaneous patients, intermediate-term follow-up has revealed no difference in survival or tumor recurrence rates. At our center, PCA has become the procedure of choice for posterior, lateral, and selected anterior renal masses.
Footnotes
Acknowledgments
The authors would like to thank Grace Todd for help with data management and storage.
Disclosure Statement
No competing financial interests exist.