
Abstract
Purpose:
To evaluate the outcome of flexible ureteroscopy training with or without an active mentor.
Materials and Methods:
Thirty-six flexible ureteroscopy naive practicing urologists and urology residents, after an initial introductory refreshment course, underwent training under a mentor for 15 minutes each in a high-fidelity nonvirtual reality Endo-Urologie-Modell (Karl Storz). The trainees were then randomized into two equal groups for training: One under a mentor and the other without. These two groups completed the training for 2 hours. Global rating scale (GRS) for the performance of flexible ureteroscopy was measured by a blinded expert at the beginning and end of the training. A specific task completion time (TCT) was noted at the end of the training. The trainees noted their own global rating scale at the end of the training.
Results:
The GRS by the expert at the end of the training was significantly higher in the mentor group. TCT was significantly lower in the mentor group. TCT correlated well with the GRS as measured by the expert rather than the trainee.
Conclusion:
Mentorship during flexible ureteroscopy training results in higher GRS and lower TCT at the end of the training. Self-assessment GRS by trainee does not correlate well with the skills acquired.
Introduction
It has been shown that training in flexible ureteroscopy using either virtual reality or high-fidelity nonvirtual reality models improves performance. 1 Although active mentoring during the performance of initial procedures in surgery has been shown to decrease the learning curve, 2 the same has not been studied in training models. We studied the influence of active mentoring during flexible ureteroscopy.
Materials and Methods
Subjects
The participants included were urology residents and board-certified urologists with the majority having previous experience with semirigid ureteroscopy. Those who had previous experience with flexible ureteroscopy were excluded. A total of 36 participants took part in the training.
Model
The high-fidelity nonvirtual reality bench model used for the study was Endo-Urologie-Modell (Karl Storz™) (Fig. 1). It consists of a mannequin of the male genitourinary tract through which standard instruments may be passed. The trainees practiced with a real flexible ureteroscope (Flex-X2, Karl Storz™), which they will be using subsequently in their operating rooms. The trainer allows the user to simulate several endourologic techniques including visualization of the entire urinary tract, guidewire insertion, placement of stent, lithotripsy. and stone retrieval.
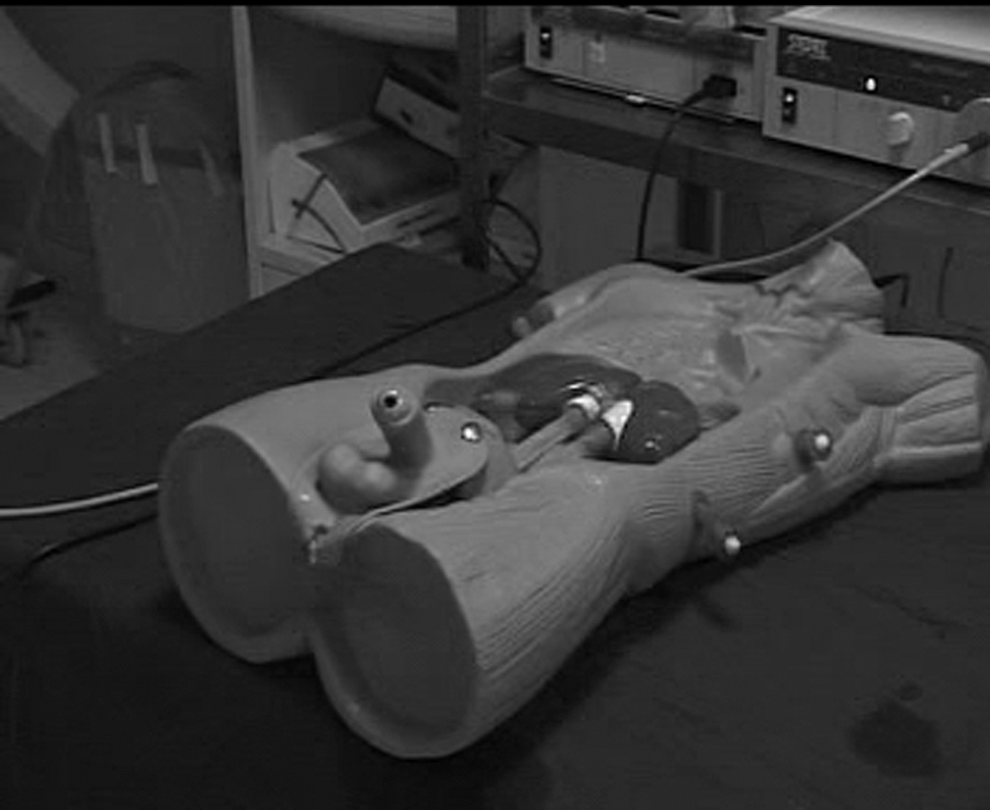
The high-fidelity bench model used in the study (Endo-Urologie-Modell).
Study design
All the participants were given didactic lectures and a video session about flexible ureteroscopy by an expert. After these, they were given hands-on training in high-fidelity nonvirtual reality Endo-Urologie-Modell for 15 minutes by a flexible ureteroscopy expert (mentor). Then they were randomized into two equal groups—one under the mentor and another without. All the participants in both the groups completed 2 hours of training.
Evaluations
The performance of the trainees was evaluated by another blinded expert ureteroscopist using a global rating scale (GRS). The GRS, adapted from Matsumoto and associates, 3 was modified, as per White and colleagues, 4 to exclude bladder and urethra and standardize the models for flexible ureteroscopy. The expert assigned a value of 1 to 5 for each of the seven aspects on the GRS. The value of the score increased with better performance. GRS was noted both at the beginning and end of the 2-hour training period. The trainees were also asked to fill their own GRS at the end of the training period.
The task given to the trainee in both groups was introducing the flexible ureteroscope into the ureteral orifice without previous guidewire across, reaching the left kidney. and visualizing the stone placed in the lower calix. The task completion time (TCT) was measured at the end of the training period. GRS by the trainee and mentor were compared and separately correlated with the TCT.
Statistics
The demographic comparison between both the groups was performed using the chi-square significance test for comparing two proportions. The paired t test was used to compare the pre- and post-training GRS. The correlation between GRS and TCT was evaluated using Spearman rank correlation. P value<0.05 was considered statistically significant.
Results
There was no significant difference between the two randomized groups with respect to age, previous experience, and subspecialty interest (Table 1). There was no difference in the initial GRS between the two groups (19.1±3.8 vs 18.2±4.0, P=0.509). The GRS of both the groups improved significantly at the end of the training period (Table 2). The GRS was significantly higher in the mentor group compared with the self-trained group. The TCT was significantly lower in the mentor group compared with the self-trained group (Table 3). The Spearman ρ for the correlation between expert GRS and TCT in self-trained and actively mentored groups were −0.868 (P<0.001) and −0.932 (P<0.001), respectively. The Spearman ρ for the correlation between self-GRS and TCT in self-trained and actively mentored groups were −0.338 (P=0.205) and 0.113 (P=0.678), respectively. Thus, GRS of expert assessment in both the groups correlated with TCT while there was no correlation between GRS by self-assessment and TCT in both the groups (Fig. 2).

Correlation between global rating scale (GRS) (expert assessment and self-assessment) and task completion times (TCTs) in the groups with and without a mentor.
Discussion
The use of flexible ureteroscopy has increased tremendously in the recent years with more patients presenting with smaller renal stones and continuous improvement in the quality of flexible ureteroscopes. Moreover, because many patients are choosing retrograde intrarenal surgery (RIRS) over percutaneous nephrolithotomy because of its less invasive nature, the indications for RIRS are expanding. There are reports of even staghorn calculi being managed with RIRS. 5 With this global shift toward flexible ureteroscopy in the management of renal calculi, both urology residents and practicing urologists are required to acquire and improve their skills in RIRS.
It is a well-known fact that the outcomes of surgeries improve with the number of procedures performed by the surgeon. In a study on semirigid ureteroscopy for ureteral stones, experienced endourologists who had been working as endourologic consultants for more than 3 years achieved more favorable results than general urologists who had been working as consultants in other urologic subspecialties, such as oncology, female urology, and pediatric urology. 6 With reducing opportunities to get hands-on training, simulator based training has an important role in developing endourology skills.
In this era of evidence-based medicine, learning basic surgical skills on the patient is no longer acceptable. There is ample evidence to show that using training models significantly improves the surgeon's skills. 7 –9 It has been shown that the ureteroscopy skills acquired from a simulator are transferred to the patient and that simulator training is helpful in improving clinical skills. 10 –12 Therefore, to improve patient outcome, reduce patient morbidity and increase the life of the costly instruments, adequate training in high-fidelity models is needed before one can perform surgery in a patient.
We conducted this study in a high-fidelity bench model (Uro-Scopic TrainerTM). Chou and coworkers 1 found no significant difference between two groups of inexperienced medical students trained in either a high-fidelity bench model (Uro-Scopic Trainer) or a VR simulator (URO Mentor™). 1 Because we are moving away from the Halsteadian way of developing surgical skills, more research into newer training models and methods of training are needed to optimize training and efficiently use resources. Although the presence of an expert throughout the training period in models may be desirable, this may be difficult in the busy schedule of a consultant urologist. Also it is not clear whether the presence of an expert is continuously needed during the training period.
In the present study, we evaluated the skills of the trainees using both Objective Structured Assessment of Technical Skills—ie, GRS and TCT. It was clear that the trainees in the actively mentored group had significantly better GRS and lower TCT than the other group. We also evaluated whether the assessment of skill acquisition by trainees themselves was accurate enough. We found correlation between TCT and GRS given by an expert but not that given by the trainees; ie, an expert is more accurate in assessing the skills of the trainee. From Figure 2, it is also evident that the variation in both GRS and TCT is low in the group with a mentor compared with the group without a mentor. This is in accordance with the goal of proper training—ie, to improve the skills and reduce interpersonal variation.
An intensive mentor-initiated approach has been shown to decrease the learning curve and maintain outcome in real-life laparoscopic surgeries. 2 The same has not been studied in training models objectively, however. The presence of a mentor during the training period may significantly hasten the learning and may decrease the total time spent in the training model before acquisition of the standard skills needed to start operating on a patient, although this remains to be seen. Also, some mistakes during the training period may go unnoticed if not actively monitored and mentored during the training. This may prove costly if the same mistake is made during real-life surgery. These minor mistakes may not be picked up if only some objective criteria such as TCT are used to monitor the progress of the trainee. Therefore, we propose that active mentoring during the initial training period is useful not only to hasten learning but also to prevent mishaps later on during surgeries on the patient.
One limitation of this study is the relatively small number of participants. Another important aspect is the transferability of skills acquired in training to real-life situations. Although it is expected that actively mentored trainees will perform better intraoperatively than an unmentored group, this aspect needs to be validated in future studies.
Conclusion
An expert more accurately assesses the skill acquisition of a trainee. Active monitoring and mentoring during the training in models can lead to faster skill acquisition and reduce mistakes during performance of flexible ureteroscopy. These in turn can potentially reduce complications and improve patient outcome in the longer run, although these aspects remain to be validated.
Footnotes
Acknowledgment
The authors would like to thank Karl Storz for lending their armamentarium Endo-Urologie-Modell and Flex-X2 scope to be used for training without charge. Source of support is the Muljibhai Patel Society for Research in Nephrourology.
Disclosure Statement
No competing financial interests exist.