
Abstract
Background and Purpose:
With the increased incidence of low-stage renal cancers, thermal ablation technology has emerged as a viable treatment option for extirpation in selected persons and is supported by the current American Urological Association guidelines. We present a 9-year, single institution experience with radiofrequency ablation (RFA) using real-time peripheral temperature monitoring of small renal masses focusing on oncologic outcomes.
Patients and Methods:
We reviewed our prospectively collected database of patients with renal masses who were treated between November 2001 and January 2011 with laparoscopic (LRFA) or CT-guided percutaneous RFA (CTRFA) with simultaneous real-time peripheral fiberoptic thermometry. Patients were followed radiographically at 1 month, 6 months, 1 year, and then annually. Clinicopathologic outcomes were collected and analyzed.
Results:
A total of 274 patients (211 male) aged 18 to 88 years (mean 67 years) with 292 renal tumors underwent LRFA (112) or CTRFA (180). Mean tumor size was 2.5 cm (0.7–5.3 cm). An intraoperative preablation biopsy showed 197 (67.4%) renal-cell carcinomas (RCC), and 77 (26.4%) benign tumors. Mean follow-up was 26 months (1–98 mos). The single ablation treatment radiographic success rate was 96% for all tumors and 94% for RCC. Metastatic RCC developed in one patient, who died. The Kaplan-Meier (KM) 3-year and 5-year cancer-specific survival was 100% and 98.6%, respectively. The KM 3-year and 5-year overall survival was 90.4% and 74.2%, respectively.
Conclusion:
RFA is a clinically effective and safe nephron-sparing treatment of patients with small renal masses. Our large cohort and intermediate-term experience adds to the building evidence for the efficacy of RFA for small renal cancers.
Introduction
Over the past two decades, treatment options for SRM have expanded, with nephron-sparing surgery and active surveillance gaining wider acceptance. Available therapies for surgical treatment of renal masses include extirpative techniques (radical nephrectomy [RN], partial nephrectomy [PN]), and thermal ablation (TA) with technologies such as cryoablation and radiofrequency ablation (RFA) most frequently being used. Mixed results have been reported on complication profiles and renal outcomes for both TA and PN. TA potentially offers a decreased morbidity profile, shorter recovery period, and improved renal functional outcomes. 5 –8 Extirpative techniques may be associated with increased morbidity 9,10 and carry increased risk of chronic kidney disease compared with TA, 11 –13 which may augment the risk of hospitalization, cardiovascular events, and death. 14
RFA has a definite role in the treatment of patients with SRM, with several series reporting on its use 15 and short-term oncologic success being clearly demonstrated. The 2009 American Urological Association (AUA) guidelines for the treatment of patients with SRM recommend that TA be reserved for clinical T1a disease in patients with increased surgical risk, yet remains an option for healthy patients with clinical T1a tumors and all patients with clinical T1b disease. 16 These guidelines were based on 10 reported studies of 528 patients with the median follow-up of 19.4 months. Long-term oncologic follow-up, therefore, was not yet available at the time the document was formulated.
A current review of the literature reveals an emerging body of evidence on the long-term efficacy of RFA in the treatment of patients with SRM. 17 –23 Our unique approach involves the use of fiberoptic nonconductive thermometry yielding real-time temperature that is used to determine therapy end point, defined as the tumor plus a small (5 mm) surrounding rim of tissue achieving a minimum of 60°C. We report our experience with peripheral thermometry-guided RFA (PTG-RFA) in the treatment of SRM in 274 patients (292 tumors) over the previous 9 years with focus on the long-term oncologic outcomes in patients with clinical stage I RCC.
Patients and Methods
Patient selection
We queried our Institutional Review Board approved, prospectively collected database of all patients who were undergoing laparoscopic or percutaneous TA for solid enhancing renal mass(es) from 2001 to 2010. Patients with solid renal mass(es) demonstrating contrast enhancement (≥20 Hounsfield units [HU]) on a multiphase iodinated CT scan were offered RFA as an alternative option to active surveillance or extirpation (total nephrectomy or PN) along with a detailed discussion of the risks and benefits of each therapy. We offer this technique currently to all patients who present with solid enhancing renal masses and do not reserve it only for the debilitated, elderly, or those with medical comorbidities. The laparoscopic or percutaneous CT-guided RFA approach was recommended based on tumor location and proximity to adjacent organs/structures (ie, bowel or ureter). Generally, anteriorly located tumors were selected for the laparoscopic approach while posteriorly located tumors were approached by CT-guidance. In addition, tumors with adjacent structures that it was felt would not be amenable to hydrodissection were performed laparoscopically. CT-guided treatment is performed by the urologist with the assistance of the interventional radiologist in the CT suite.
Inclusion criteria for this study were adult patients with primary clinical T1 renal tumors (<7 cm) who were undergoing either laparoscopic or percutaneous RFA. Patients who were undergoing salvage operations or nonstandard ablation techniques (microwave ablation or flat-panel detector CT guidance) were excluded. In the oncologic outcomes subanalysis, those having intraoperative biopsy results of angiomyolipoma, oncocytoma, nonneoplastic lesions (cystic masses, fibrosis, inflammation), nondiagnostic biopsy, or nonrenal origin cancers (one patient with metastatic lung cancer) were excluded.
Radiographic success was based on contrasted CT scans and defined as a lack of enhancement (<20 HU increase) of the ablation zone (comparing plain CT with cortical and delayed phases). 24 Because of the lack of strict radiologic criteria in defining viability of tissue (“enhancement”) on MRI, ultrasonography (US), and noncontrast studies, patients who were not undergoing contrasted CT imaging were excluded from all analyses with the exception of those with diagnostic tissue samples obtained >6 months postoperatively. In addition, no distinction was made between patients with “incomplete ablation” and “local recurrence” as previous authors have reported. 25 All patients with persistent enhancement were considered radiographic failures. For this reason, a minimum follow-up of only 1 month was used to ensure that patients with radiographic recurrence and shorter follow-up were not excluded (falsely lowering the number of radiographic failures).
Treatment success was defined as lack of radiographic recurrence or, alternatively, a negative tissue sample in the event of radiographic “recurrence.” Our database contains information on 336 renal ablations performed in 309 patients. Using the criteria described above, 292 tumors in 274 patients were identified and included in this study. Some patients had more than one tumor treated, and these were followed as independent events if nonsynchronous.
Surgical technique
Laparoscopic RFA (LRFA) with peripheral fiberoptic temperature monitoring
LRFA was performed in a technique previously published. 5 Although more time consuming and labor intensive, the placement of up to four temperature extrinsic fiberoptic probes in the areas thought to be most difficult to treat (ie, the deep margins) allows for a logical approach to any TA; that is, a well-defined scientifically valid end point. Needle probes that are deployed with temperature sensors built in can only measure the temperature where the ablation needle/tissue interface. It does not yield a reliable global temperature grid. When treating larger tumors with multiarray expandable deployable needles, the space between each tine increases and thus may lead to “gaps” of undertreated areas. When using a single needle probe (as with the cool tip), the geometry of the ablated areas is much more uniform.
A transperitoneal approach was used to gain exposure to the kidney and dissect away any adjacent structures (vessels, ureter, bowel) in the vicinity of the tumor to avoid any collateral damage. Next, a laparoscopic ultrasound probe (Aloka, Wallingford, CT) aided in the localization and measurement of the tumor as well as placement of two to four 5.0F/10 cm Yueh centesis catheter needles with radiopaque sheaths (Cook Vascular, Inc, Vadergrift, PA) 5 mm from the tumor periphery. Fiberoptic thermal sensors (Lumasense, Santa Clara, CA) were inserted through these catheters. Before ablation, 18-gauge core-needle biopsies are performed. Finally, a 2 or 3 cm Cool-tip™ water-perfused RFA probe (Covidien Inc, Boulder, CO) or a RITA® StarBurst® (Angiodynamics, Latham, NY) was advanced into the tumor, and RFA commenced with simultaneous peripheral fiberoptic thermometry (Fig. 1). The treatment end point was defined as a temperature of ≥60°C in all temperature sensors. If all temperature sensors did not achieve ≥60°C or sustained ≥50°C, then multiple RFA probes were placed or a single RFA needle was redeployed within the tumor until the treatment end point was met, thus varying the treatment time.

Intraoperative view of laparoscopic peripheral thermometry-guided radiofrequency ablation (RFA) technique. The tumor is seen in the center of the image. Peripheral nonconducting fiberoptic thermometry is placed under guidance of ultrasonography (yellow arrows). The Cool-tip® RFA probe is placed through the center of the tumor, also by ultrasonography guidance (white arrow).
CT-guided percutaneous RFA (CTRFA) with peripheral fiberoptic temperature monitoring
CTRFA was performed in a technique previously published. 5 Once the patients were under general anesthesia and placed in a prone position in a CT gantry, a preliminary CT scan was performed with or without the use of contrast. Once the targeted tumor was visualized, up to four 5.0F/10 cm Yueh centesis catheter needles with radiopaque sheaths were placed in the periphery of the tumor and, if necessary, adjacent to vital structures such as large bowel or ureter. Fiberoptic thermal sensors were inserted through the Yueh sheaths. Before ablation, multiple 18-gauge core-needle biopsies were taken. A 2 or 3 cm Cool-tip water-perfused ablation probe or a RITA StarBurst was advanced into the tumor and RFA commenced with simultaneous peripheral fiberoptic thermometry (Fig. 2). We carefully monitored temperatures adjacent to bowel and ureter, when appropriate, to avoid any temperature >40°C.
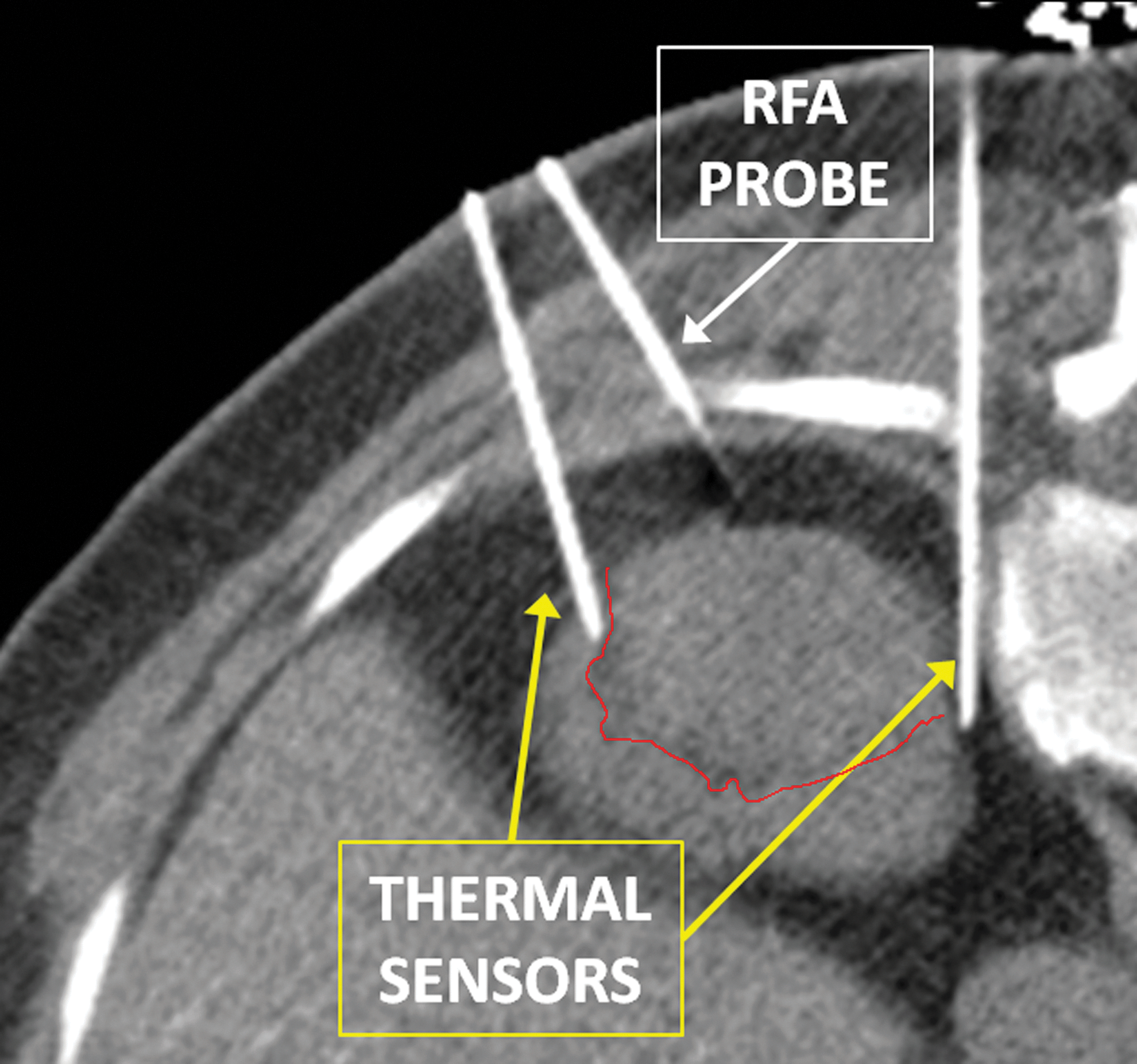
Intraoperative view of percutaneous (CT-guided) peripheral thermometry-guided radiofrequency ablation (RFA) technique. The tumor is seen in the center of the image with tumor borders demarcated with a red line. Peripheral nonconducting fiberoptic thermometry is placed under CT guidance (yellow arrows). The Cool-tip® RFA probe is placed through the center of the tumor also by CT-guidance (white arrow).
Patient surveillance
Patients were followed for tumor recurrence by contrast abdominal CT scans at 1 month, 6 months, 1 year, and annually thereafter. The surveillance schedule was similar in all patients regardless of pathology results. Complications were recorded in the first 90 days of the postoperative period according to the Clavien-Dindo classification of surgical complications. 26
Statistical analysis
Chi-square tests for categorical variables and independent Student t test for continuous variables were performed using SPSS 18.0 (SPSS Inc, Chicago, IL). Survival analysis was performed using Kaplan-Meier estimation. Multivariate analysis was performed using Cox regression.
Results
A total of 274 patients (211 male) with 292 renal tumors met the inclusion criteria for evaluation. One hundred and twelve (112) underwent LRFA (38%) and 180 percutaneous CTRFA (62%). Twelve patients had synchronous ablations. Mean tumor size was 2.54 cm (0.7–5.3 cm) with comparable mean tumor size in CTRFA and LRFA groups (P=0.072). Patient and tumor demographics are detailed in Table 1. Comparison of the CTRFA and LRFA cohorts with chi-square tests for categorical variables and independent Student t test for continuous variables showed the CTRFA group to have younger age (P=0.047, 66 vs 69 years), more right-sided procedures (44% vs 40%, P=0.011), and a larger body mass index (BMI) (28 vs 27, P=0.024). As shown in Table 1, all other comparisons stratified by approach showed no statistical difference.
CTRFA=computed tomography guided radiofrequency ablation; LRFA=laparoscopic radiofrequency ablation; BMI=body mass index; AACCI=Age-adjusted Charlson Comorbidity Index; RCC=renal-cell carcinoma; SD=standard deviation; RF=radiofrequency; IQR=interquartile range; eGFR=estimated glomerular filtration rate.
P value.
Endophytic tumors are those completely enclosed by renal parenchyma with no exophytic components.
This includes the number of procedures necessitating thermometer placement next to an organ because hydrodissection (CTRFA) or laparoscopic dissection was unable to achieve adequate separation from the intended ablation area.
The Cool-tip™ RFA probe was used in the majority of cases, but the RITA® StarBurst® was also used.
Intraoperative biopsy, before ablation, was performed in 288 (98.6%) tumors (four were not biopsied), of which 197 (67.5%) were RCC, 77 (26.4%) were benign tumors, and 14 (4.8%) were classified as nondiagnostic biopsies. Tumor pathologies are shown in Table 2.
RCC=renal-cell carcinoma.
Post-RFA radiographic surveillance results
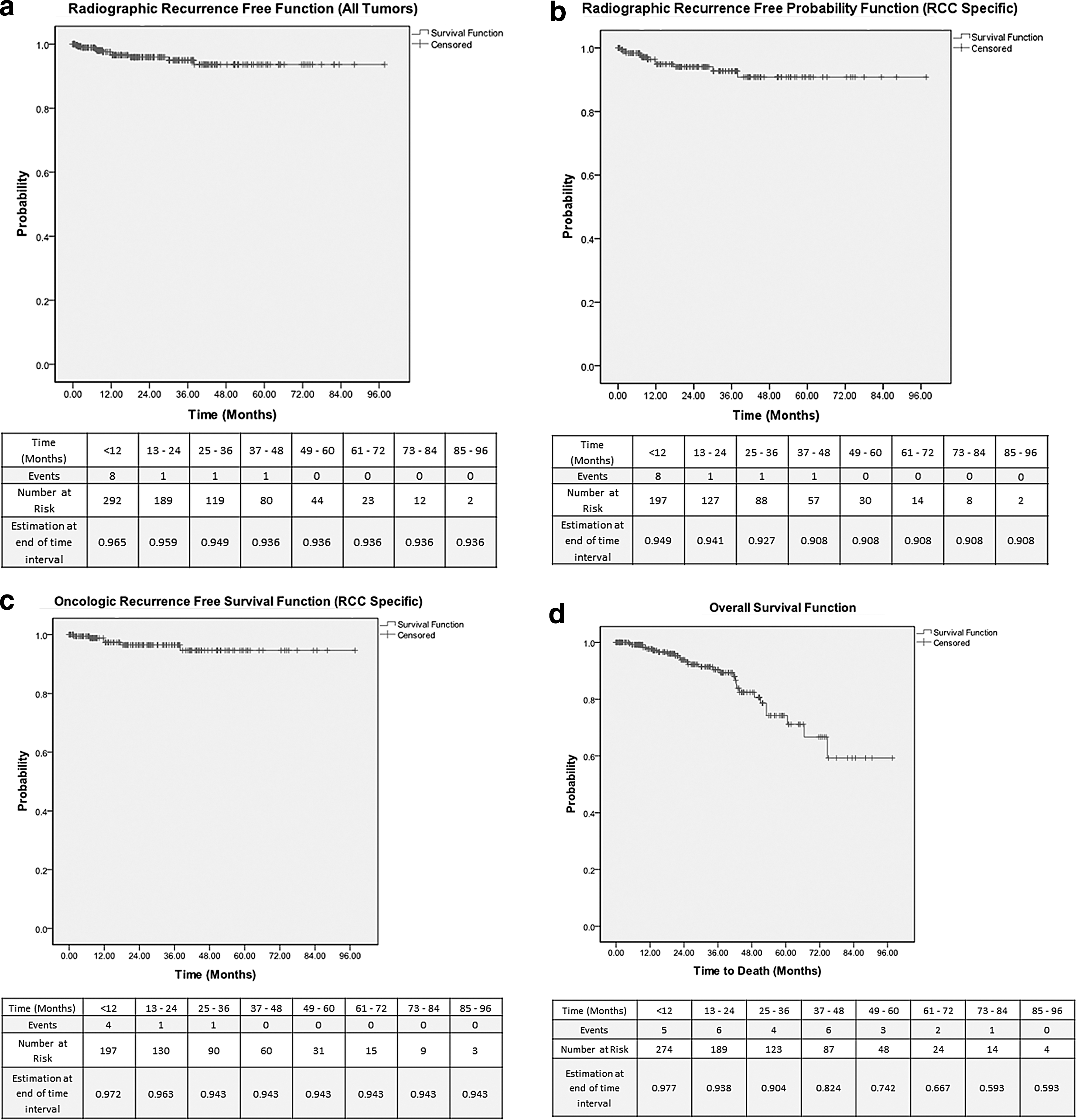
Mean follow-up was 26 months (1.0–98 mos). Of the 292 treated tumors, 11 (3.8%) had persistent enhancement on follow-up imaging. All 11 radiographic failures were in the biopsy-proven RCC cohort (no benign tumors had failure). Six of the 11 “radiographic failures” were found to contain viable tumor on follow-up intervention (ie, true positives), whereas 5/11 had nonviable tumor or scar tissue. This could be because of sampling error in the samples that were biopsied, however. The clinical course of patients with radiographic failure is shown in Table 3. Kaplan-Meier (KM) curves are depicted for radiographic recurrence-free probability of all tumors (Fig. 3A) and RCC-specific tumors (Fig. 3B).
LAP=laparoscopic; RCC=renal-cell carcinoma; FG=fuhrman grade; RFA=radiofrequency ablation; NED=no evidence of disease; CTRFA=computed tomography guided radiofrequency ablation; LRFA=laparoscopic radiofrequency ablation.
Oncologic outcomes
Of the 11 radiographic recurrences (7 CTRFA and 5 LRFA), 6 patients had rebiopsy pathology results confirming viable RCC. Thus, the primary ablation success (tumors necessitating only one ablation) rate was 96% for all tumors and 94% for RCC-specific tumors. The 3-year and 5-year cancer-specific survival was 100% and 98.6%, respectively. The KM estimation of oncologic success is shown in Figure 3C, with 3-year and 5-year recurrence-free survival in this group being 94.3% and 94.3%, respectively. The 3-year and 5-year overall survival was 90.4% and 74.2%, respectively (Fig. 3D). Multivariate analysis accounting for surgical approach, age-adjusted Charlson Comorbidity Index, BMI, tumor laterality, tumor depth (exophytic vs meso/endophytic), collecting system involvement (<5 mm from collecting system), and tumor size showed only tumor size to be a significant predictor of radiographic failure (P=0.007, odds ratio 2.2, 95% confidence interval 1.2–3.9).
Six of 11 patients with initial radiographic treatment failures elected to undergo a repeated CTRFA, with 4 pre-RF biopsy results confirming the presence of viable RCC. RCC was also confirmed in the two patients who elected to undergo a radical nephrectomy.
Two CTRFA treatments failed in one 89-year-old patient with a 5-cm RCC who eventually was found to have lung metastases at 12 months postablation, resulting in death at 40 months from the initial therapy.
Complications
Of the 292 ablations performed in 274 operations, complications occurred in 75 (27%) patients. Table 4 shows the breakdown of complication Clavien grades for this cohort. The CTRFA group accounted for 65% of total complications. Only one patient needed a blood transfusion, and 87% of total complications were minor (Clavien grade I or II).
Major complications are classified as those Clavien grade III or higher. Minor complications are classified as grade I or II.
Discussion
Since the first clinical reports on percutaneous and laparoscopic renal RFA at the turn of the 21st century, 27,28 we have progressively accumulated data on the immediate technical success and safety as well as the short-term functional and oncologic outcomes of this treatment modality whereby we treat patients irrespective of age and who often have unfavorable characteristics. More recent evidence shows some of the intermediate- to long-term efficacy (Table 5). The current series has success similar to other recently reported series in Table 5. The majority of RFAs are performed percutaneously under CT guidance with only a few centers using a laparoscopic approach. 16 Therefore, more than 60% of the published studies cited on the experience with RFA comes from the interventional radiology experience. 29
CT=computed tomography; RF=radiofrequency; HU=Hounsfield unit; RCC=renal-cell carcinoma; RFA=radiofrequency ablation; CTRFA=computed tomography guided radiofrequency ablation; MRI=magnetic resonance imaging; Lap=laparoscopy.
The 2009 AUA guidelines for T1 renal masses included RFA as a treatment recommendation and option for selected persons. This was based on these early reports, which revealed local control to be suboptimal when compared with surgical excision. Therefore, our primary goal was to report our interdisciplinary approach combining the efforts of interventional radiology and urology to optimize RFA success with one treatment session and produce superb oncologic control along with maximum nephron sparing. Forty-two percent of our patients were followed for >24 months, and 29% of patients were followed for >36 months. One limitation of this study is the limited follow-up, given the long period of the study. This is largely because of a much higher volume of ablations being performed in more recent years compared with the beginning years of this study.
We attribute our high (96%) single treatment success rate to the PTG-RFA technique. Despite one-fourth of our tumors having unfavorable characteristics or locations (24% endophytic, 28% <5 mm from the collecting system, 5% in danger of thermally damaging adjacent organs), we were able to maintain high success rates. Exclusively following the manufacturer recommendations in impedance-based RF machines may result in treatment failure, especially in central tumors, which may not experience therapeutic temperatures throughout their volume during the irradiation time because of the heat-sink effect of larger centrally located vessels and the collecting system. Performing an immediate post-RFA contrast CT study may increase the risk of false negative scans from distortion of the ablation zone with a hematoma and/or the theoretical presence of temporary post-RFA vasospasm. In addition, no other technique allows for temperature measurement of vital structures such as the ureter or bowel to assure their safety when they are adjacent to the zone of ablation. Finally, visual cues, such as tissue desiccation, color change, and bubbling, may increase the surgeon's confidence in the success of the RF treatment; however, these clues may not be as reliable with more endophytic tumors.
The simplicity of the PTG-RFA technique makes any type of hyperthermic TA (RF, microwave, or any future modality) more reliable to ensure oncologic and nephron-sparing end points until more sophisticated, noninvasive, image-based thermal monitoring becomes widely available. The possible weakness of the technique applies to the LRFA group where the temperature sensor and ablation probe placement is largely dependent on laparoscopic ultrasonography, which is arguably not as precise as CT-guided instrument placement. Nevertheless, the difference in treatment failure rate between the CTRFA and LRFA groups was not statistically significant.
Furthermore, our definition of treatment failure is 10 HU higher than other comparable studies, thus leading to a lower failure rate. Arguably, our patient selection criteria were stricter and defined enhancement as ≥20 HU, to decrease the type 1 error. It has been previously suggested, however, that a 10 to 20 HU increase may be indeterminate and lacking unequivocal enhancement because of unreliability of absolute HU readings. 24 Clinically, however, patients with “pseudoenhancement” between 10 to 19 HU thus far have not shown any progression on follow-up. Finally, our study is limited by the lack of histologic data (biopsy after ablation) on all patients with radiographic success to confirm oncologic success. Again, lack of progression, tumor shrinkage, and time have proven to be reliable indicators.
Conclusion
Our large series of CTRFA and LRFA patients who were treated under peripheral thermometry guidance provides strong evidence for both surgical success of this technique in patients with SRM as well as outstanding intermediate-term oncologic outcomes that are comparable to the PN and RN series. 16
Footnotes
Acknowledgment
We would like to acknowledge the contribution of the Endourology Society Fellows from the University of Miami who contributed to the ongoing data collection and surgical procedures.
Information in this article was presented at the American Urological Association Annual Scientific Meeting in Washington, D.C., May 17, 2011.
Disclosure Statement
Dr. Leveillee has research support in the form of equipment from Covidien, Angiodynamics, and INTIO. He receives no compensation for these studies. For the remaining authors, no competing financial interests exist.