
Abstract
The objective of this study was to estimate the treatment effect of Pneumatic Lithotripsy (PL) versus holmium: YAG laser lithotripsy (LL) in the treatment of distal ureteric calculi. A bibliographic search covering the period from 1990 to April 2012 was conducted using search engines such as MEDLINE, EMBASE, and Cochrane library. Data were extracted and analyzed with RevMan5.1 software. A total of 47 studies were scant, and 4 independent studies were finally recruited. Holmium: YAG LL conveyed significant benefits compared with PL in terms of early stone-free rate [odds ratio (OR)=4.42, 95% confidence interval (CI) (1.14, 17.16), p=0.03], delayed stone-free rate [OR=4.42, 95%CI (1.58, 12.37), p=0.005], mean operative time [WMD=−16.86, 95%CI (−21.33, −12.39), p<0.00001], retaining double-J catheter rate [OR=0.44, 95%CI (0.25, 0.78), p=0.004], and stone migration incidence [OR=0.26, 95%CI (0.11, 0.62), p=0.003], but not yet in the postoperative hematuria rate and the ureteral perforation rate according to this meta-analysis. Precise estimates on larger sample size and trials of high quality may provide more uncovered outcomes in the future.
Introduction
Ureteroscopic lithotripsy incorporates abundant subtypes, such as pneumatic lithotripsy (PL), laser lithotripsy (LL), electric hydraulic gravel, and ultrasonic lithotripsy. Among them, PL and holmium LL are two major approaches favored by urologists. A proportion of researchers recommended LL, because they found it more effective in ureteric calculus clearance with less-associated complications than please. 3 –7 On the contrary, in another study from Garg et al, though LL may seem to provide a stone-free state within a comparatively short postoperational period, it also required longer operational time and aroused an equivalent amount of complications compared with please. 8 In the latest report from Kassem et al, both PL and LL are equally effective and safe in handling large ureteric stones, while the pneumatic system may be more efficient with regard to the cost–benefit ratio. 9
Aimed at uncovering more robust evidence and providing valid guidelines for clinical practice, we conducted this formal meta-analysis to compare the effectiveness of LL and PL in the treatment of distal ureteric calculi.
Materials and Methods
Methods of the analysis and inclusion criteria were specified in advance and documented in a protocol.
Inclusion and exclusion criteria
1. Type of studies: Randomized clinical trials comparing the efficacy of Holmium: YAG laser and pneumatic lithoclast in treating distal ureteric calculi were consulted. Published, as well as unpublished, investigations were both looked up. Studies were excluded if they were case reports, meeting abstracts, conference proceedings, or publications with regard to upper ureteral calculi. No language, publication date, or publication status restrictions were imposed.
2. Type of participants: The age of patients must be above 16. ureteral stones must be definitely diagnosed preoperative, and the diameter of the ureteric stone was ranging from 4 mm to 20 mm. Patients with cystine stones must be excluded since the composition of stone might be a cofounding factor. Furthermore, participants with ureteric stricture were also not a choice of consideration.
3. Types of intervention: The experimental group used Holmium: YAG laser for distal ureteric stone, and the control group used a pneumatic lithotripter. Trails using basket to stop stone migration were excluded.
4. Type of outcome measures: mean operative time, stone clearance rate, ureteral perforation rate, hematuria rate, stone migration, and retaining JJ catheter rate.
Literature research
Several search strategies were applied
1. An electronic search was conducted in the following databases: MEDLINE (1990.1–2012.5), EMBASE (1990.1–2012.5), and the Cochrane library (1990.1–2012.5). Databases were searched for the occurrence of the keywords Swiss Lithoclast, pneumatic, YAG laser, holmium laser, ureteral stone, and calculi anywhere in the record, taking the search strategy of Medline, for example (Appendix 1).
2. Additional manual searches of the reference lists included studies, reviews, meta-analyses, and guidelines on comparing the efficacy of Holmium: YAG laser and pneumatic lithoclast in treating distal ureteric calculi.
3. We contacted the first authors of all identified studies comparing the efficacy of Holmium: YAG laser and pneumatic lithoclast in treating ureteric calculi and asked them for unpublished material, ongoing research, and whether they knew of any other researchers having unpublished data or ongoing studies.
Quality assessment and data extraction
Two reviewers (Xiangrui Yin and Ziwei Tang) independently assessed study quality using the checklist developed on the basis of quality assessing the items provided by Cochrane organization. According to Cochrane, quality assessment shall be conducted on the premise of the following aspects: the details of randomization, allocation concealment, blinding of investigators, participants, outcome assessors, intention to treat analysis, selective outcome report, completeness of follow-up, and comparable basic characteristics. Based on the quality components, studies were subdivided into the following three categories: (1) all quality components adequate: low risk of bias; (2) one or more of the quality components unclear: moderate risk of bias; (3) one or more of the quality components inadequate: high risk of bias.
Eligibility assessment and data extraction were performed independently in an unblinded standardized manner by two reviewers (Xiangrui Yin and Ziwei Tang). Extracted data included eligibility criteria, baseline characteristics, interventions, outcomes, and methodological quality. The primary outcome referred to mean operative time, stone clearance rate, ureteral perforation rate, hematuria rate, stone migration, and retaining JJ catheter rate. Trial methodological quality was assessed by the Cochrane risk of bias tool. Disagreements between reviewers were resolved with the involvement of a third reviewer.
Statistical analysis
We used Review Manager software version 5.1 provided by The Cochrane Collaboration for the statistical analysis. Odds ratios (OR) were calculated for dichotomous data and mean divergence with 95% confidence interval for continuous data. We examined heterogeneity in studies with the χ 2 and I 2 statistic. 10 If significant heterogeneity was found (p<0.1), we proceeded to subgroup analysis or sensitivity test. In case the heterogeneity still existed, the random-effects model 11 was applied. Otherwise, we used a fixed-effects model with the Mantel–Haenszel method to calculate the pooled OR. The Mantel–Haenszel method with a treatment arm continuity correction was adopted to verify the results in studies with zero events, because the trial arms were unbalanced. 12
Publication bias was also checked in a funnel plot of log OR against its standard error using Begg's test, and the degree of asymmetry was tested by Egger's unweighted regression asymmetry test. 13,14
Results
Search result
Database searches yielded forty-seven references. Exclusion process is demonstrated in Figure 1. We excluded 35 because of irrelevance after reviewing the title, abstract, and eventually the full text. Eight studies were further removed, because four of them were not related. Four of them were retrospective control trails. Finally, four prospective control trials remained, which all fulfilled the inclusion criteria. Two hundred ninety-five patients were included. All patients were followed postoperatively by recording and evaluating any of the postoperative symptoms, kidney, ureter, and bladder radiograph (KUB) or computed tomography (CT) on postoperative day 1 to assess the early stone-free rate. Follow-up after 1 month, urine culture, KUB, or CT. Complications were assessed using the Clavien Classification of Surgical Complications. 15
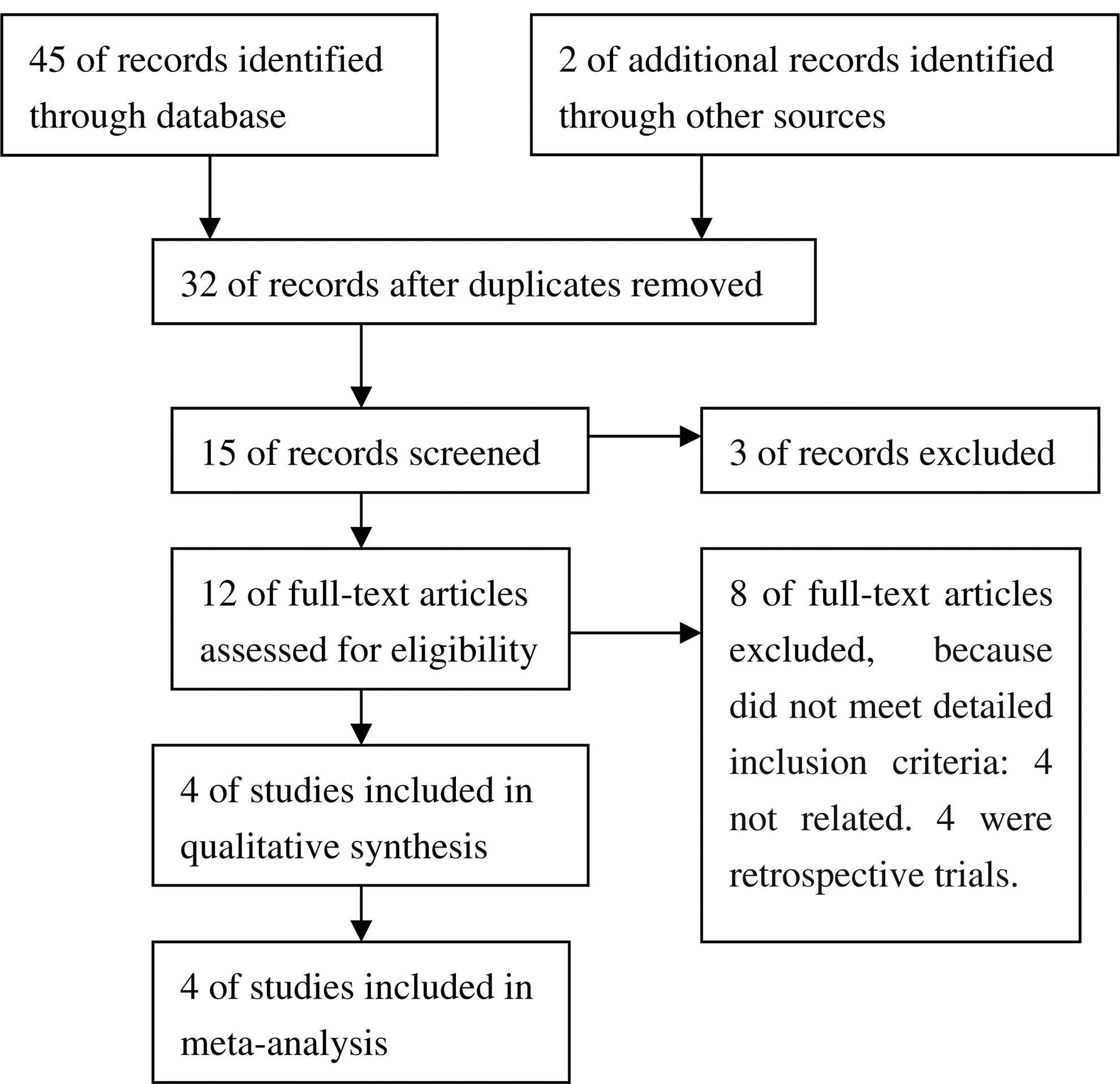
Flowchart of search results.
Methodological quality and baseline characteristics
All included 4 trials were randomized controlled trials (RCTs) and reported to be published in 2008–2012 4,5,8,9 (Table 2); however, all of them were level of B and did not match the best standard required for RCTs for lack of clear description of their methods (Table 1). The standard format should be comprehended in the following section: (1) General information about the study, including the authors, publication year, nationality of the study, interval of time in which the subjects were enrolled, total number of patients, gender, and age (range and mean). (2) Inclusion and exclusion criteria, stone diameter, and stone location. (3) Type of surgical procedure, type of stone fragmentation device, antibiotic prophylaxis, and time of surgical procedure. (4) Early and delayed stone-free rate, stone migration rate, ureteral perforation rate, and number and type of complications. Overall, the baseline similarity of the included four trials was certified. There were 294 participants were involved in this meta-analysis.
mm2.
N1=perforation; N2=hematuria; N3=D-J catheter; N4=delayed stone-free rate (%); NR=not reported; PL=pneumatic lithotripsy; LL=laser lithotripsy.
Outcomes
Mean operative time
All trials, except for Maghsoudi, 4 explicitly compared the mean operative time. We excluded the Garg, 8 because it only counted the lithotripsy time. Low level of heterogeneity was detected among the trials. Thus, we used the fixed-effects model. The result showed that the two groups were significantly different in the mean operative time [WMD=−16.86, 95% confidence interval (CI) (−21.33, −12.39)7, p<0.00001] (Fig. 2).
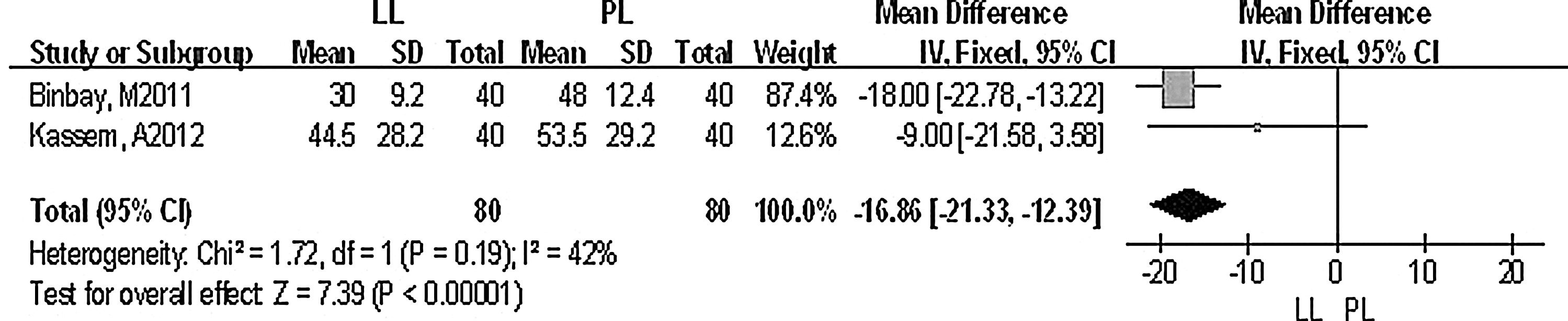
Comparison of laser lithotripsy (LL) versus pneumatic lithotripsy (PL) on the mean operative time.
Early stone-free rate
All trials reported information on early stone-free rate. The hypothesis that the studies were homogeneous was rejected. We did not find obvious sources of heterogeneity by a sensitivity analysis. Therefore, we used the random-effects model, and we were able to find out that LL was more likely to achieve early stone free rate than PL [OR=4.42, 95%CI (1.14, 17.16), p=0.03] (Fig. 3).
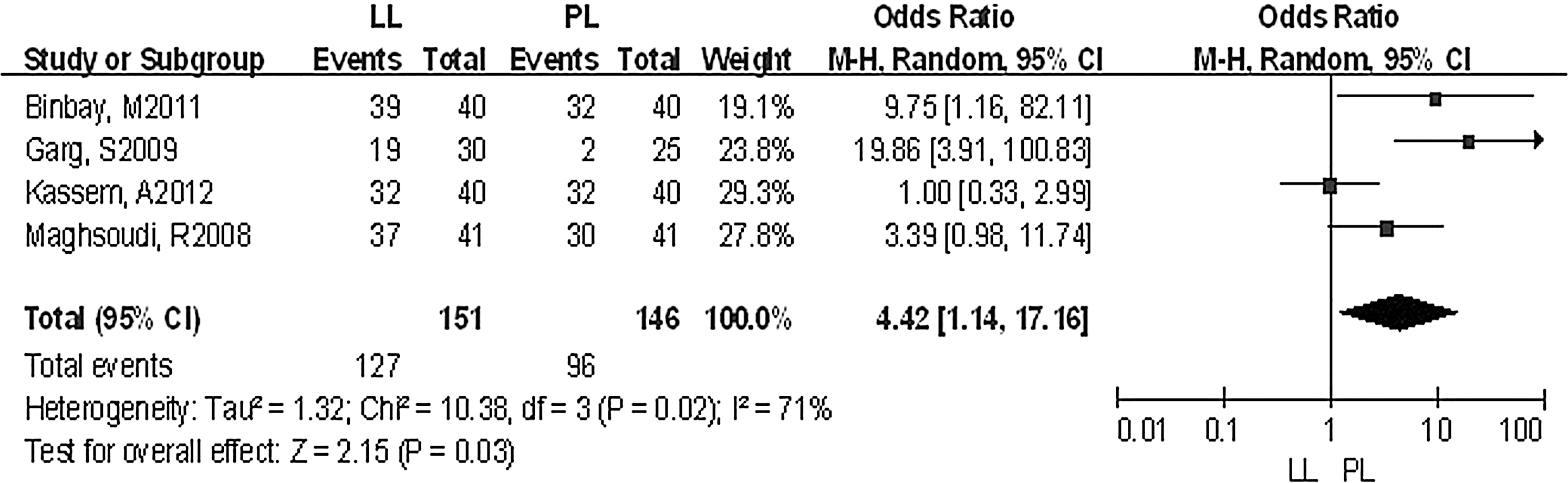
Comparison of LL versus PL on the early stone-free rate.
Delayed stone-free rate
Three trials 5,8,9 described information on delayed stone-free rate. With a 0.90 p-value from chi-square test and a zero score in I 2 statistic, as demonstrated below, it was likely for these mixed studies to present homogeneity when it came to analyze this item. Thus, we used the fixed-effects model. As a result, LL improved a delayed stone-free rate to a larger extent than PL [OR=4.42, 95%CI (1.58, 12.37), p=0.005] (Fig. 4).

Comparison of LL versus PL on the delayed stone-free rate.
Migration rate
All trials carried out comparison on stone migration rate. We contacted the first author by E-mail and telephone, and we proved that the surgery did not use the basket for stopping stone migration. On the basis of heterogeneity analysis, we found the studies combinable and thus used the fixed-effects model to integrate information. When it came to the migration rate, LL seemed to be more beneficial than PL [OR=0.26, 95%CI (0.11, 0.62), p=0.003] (Fig. 5).

Comparison of PL versus LL on the stone migration rate.
Ureteral perforation rate
All trials displayed results on the ureteral perforation rate. Two of the studies were not estimable on the OR. There was no obvious existence of heterogeneity. According to the fixed-effects model analysis, neither PL nor LL had significant advantages over the other in ureteral perforation rate [OR=1.85, 95%CI (0.49, 7.02), p=0.37] (Fig. 6).
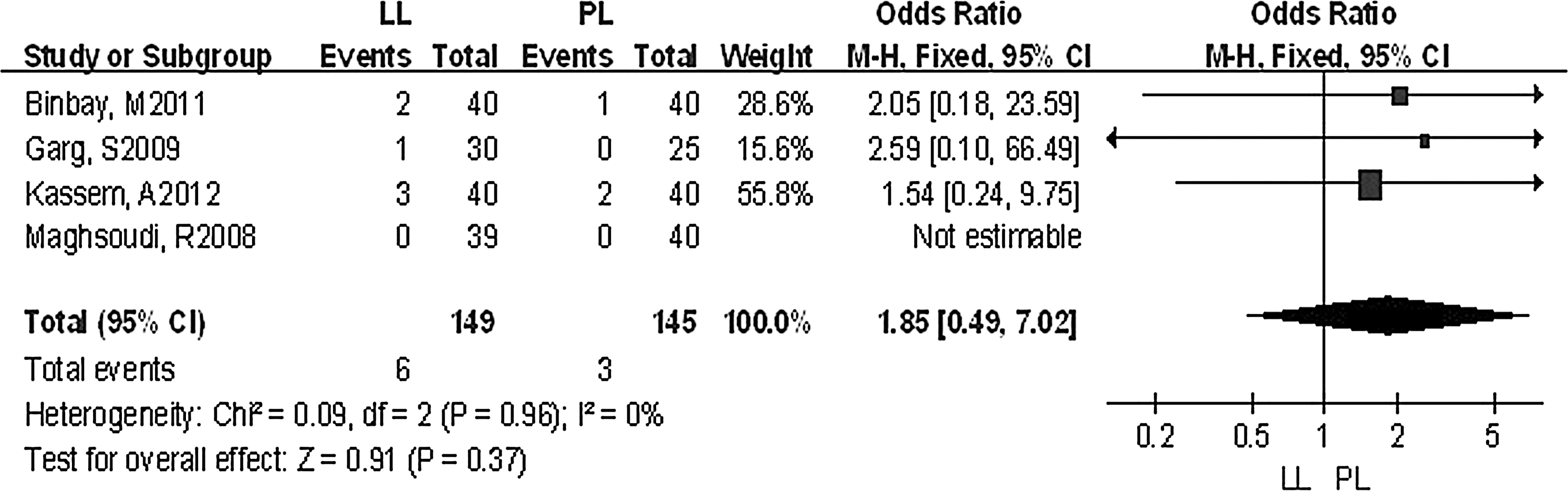
Comparison of LL versus PL on the ureteral perforation.
Postoperative hematuria rate
Only two trials 4,8 presented reports on postoperative hematuria. We employed the fixed-effects model in accordance with absence of heterogeneity. The result suggested that neither was likely to improve postoperative hematuria when compared with the other [OR=0.73, 95%CI (0.25, 2.11), p=0.56] (Fig. 7).
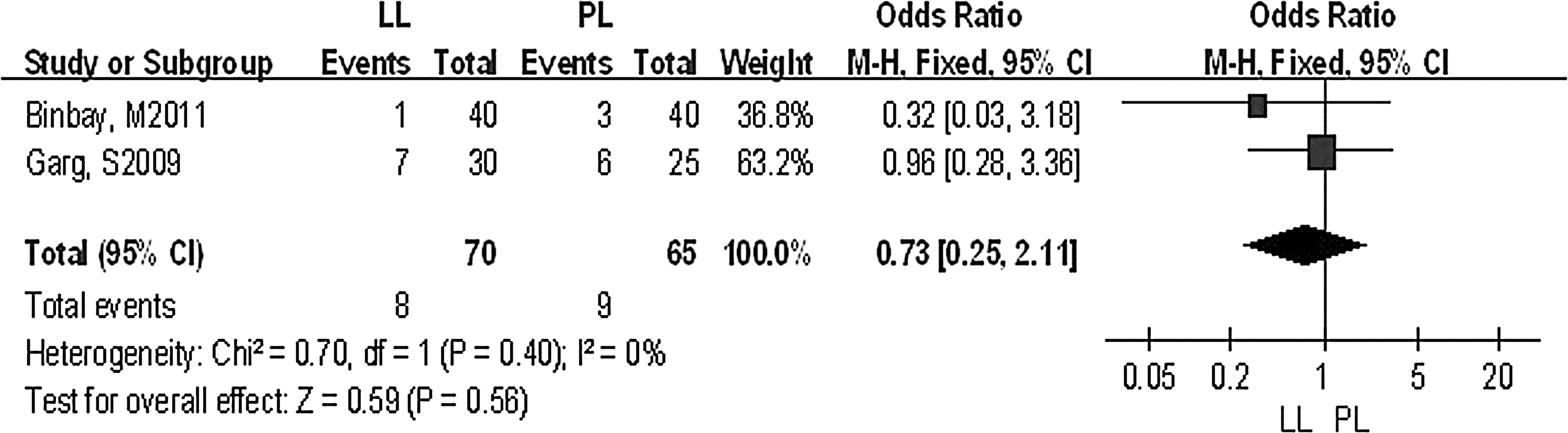
Comparison of LL versus PL on postoperative hematuria rate.
Retain JJ catheter rate
Three trials 4,8,9 presented reports on Retain JJ catheter. A correspondingly low level of heterogeneity was detected. Although the square from each individual study dispersed in both sides in this forest plot, there were significant differences between PL and LL when tested for overall effect [OR=0.44, 95%CI (0.25, 0.78), p=0.004] (Fig. 8).
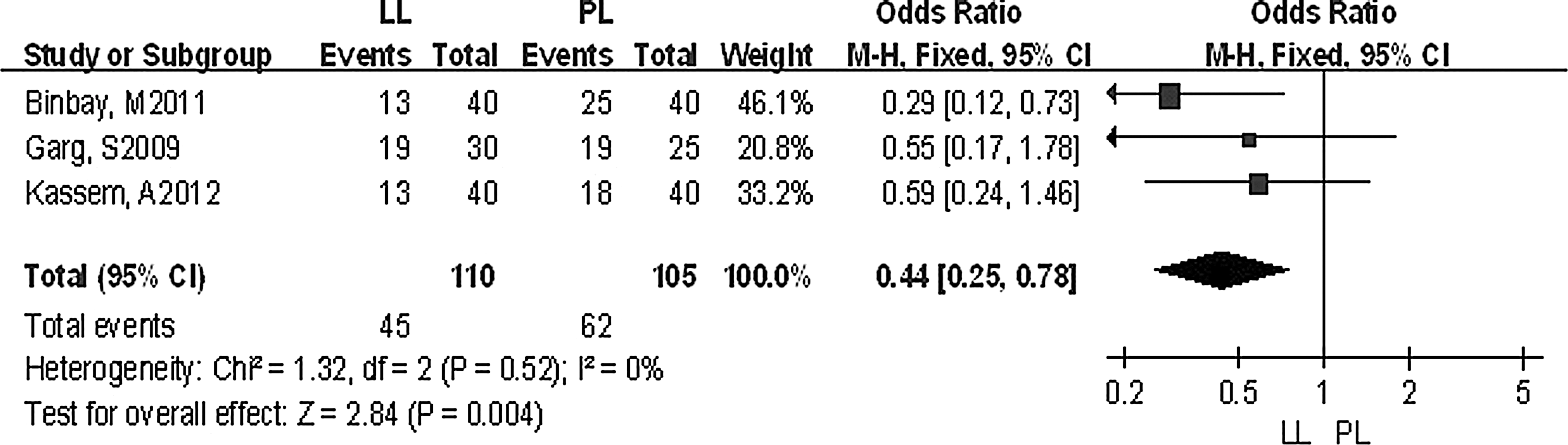
Comparison of LL versus PL on retaining JJ catheter rate.
Discussion
PL has been the most widely used method of stone disintegration. It fragments calculi mechanically like a pneumatic jackhammer with no thermal or cavitation effects. Thus, the risk of causing injury to the ureteric wall is minimal. 16,17 It is a safe and effective method for stone treatment. 18 Nevertheless, there exist some disadvantages that we cannot ignore. Semirigid probe requires a rigid or at least a semirigid ureteroscope, and there is a high possibility of undesired retrograde displacement of the calculus. 19,20 The holmium: YAG laser, on the contrary, has excellent stone-fragmenting properties, and as a result, it is now a well-established modality for intracorporeal lithotripsy. 21,22 Ho:YAG lithotripsy is the small fragments created by the Ho:YAG laser versus please. 23 It uses photothermal energy to fragment stones. The thermal effect is limited to a few millimeters with a penetration depth of only 0.5 mm. LL light can be transmitted through a thin, flexible fiber compared with PL. It depends on photothermal mechanism for stone fragmentation; thus, the risk of retrograde stone propulsion could be minimized, but it may cause thermal injury to the ureter if used improperly. 24
In our study, we discovered advantages of LL in improving early stone-free rate as well as delayed stone-free rate. In addition, LL presented less incidence of calculus migration and mean operation time, retaining JJ catheter rate, whereas we failed to detect any significant difference between PL and LL in the ureteral perforation rate and the postoperative hematuria rate. Except for the early stone-free rate, the rest of these items were all analyzed on the basis of homogeneity across studies, indicating that the variation was only due to play of chance. Since a high level of heterogeneity exited between trials when analyzing the early stone-free rate, the interpretation of the outcome might not be as reliable as that of the other items. Personally, we suspected that the distinguished professional competence and familiarity with the two types of practice might account for the heterogeneity. We did not find obvious sources of heterogeneity by a sensitivity analysis, and we were unable to exclude patient-specific factors or study design factors contributing to the heterogeneity. Meta-analysis is a statistical strategy for the purpose of integrating the findings of individual studies into a single estimate. The review included four randomized controlled trails, Regretfully, none of their quality reached level A. In addition, funnel plots showed the presence of publication bias. Therefore, the findings of this review should be interpreted with caution unless more clinical trials become available in future.
Conclusions
This study generally compared the effectiveness and related complications of PL and LL in the treatment of distal ureteric stones for the first time. The pooled results of the trials suggest that LL had advantages over PL with high efficiency of stone-free rate and a low migration rate, retaining the JJ catheter rate. We recommended LL as a powerful, effective, and safe treatment modality for distal ureteral calculi.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix 1
Taking the search strategy of Medline for example:
#1. randomized controlled trial
#2. “Swiss Lithoclast “
#3. “pneumatic”
#4. (#2)or(#3)
#5. “YAG laser”
#6. “holmium laser”
#7. (#5)or (#6)
#8. “ureteral stones”
#9. “calculi”
#10. (#8) OR(#9)
#11. (#1) and (#4) and (#10)