
Abstract
Purpose:
In this study, we report our initial experience using microperc for treatment of kidney stones and the implications of the microperc system in bladder stone management.
Patients and Methods:
Microperc was performed with a 4.85F “all-seeing needle” in 11 patients with stone disease; 9 of the patients had kidney stones and 2 had bladder stones. Access to the renal collecting system was achieved under fluoroscopic control in eight patients, while ultrasonography was used in one. Fluoroscopy was not used in any of the patients with bladder stones for bladder access.
Results:
The mean stone burden was 12.8 mm (range 7–18 mm). The stone locations were pelvis in three, upper calix in one, middle calix in two, and lower calix in three. The mean age for kidney stones was 20.8 years (range 3–47 years). Single access was sufficient in all cases. In two patients, although the procedure was progressing without complication, conversion to miniperc was needed because of operator-related system errors. There were no intraoperative complications. The stone-free rate in the postoperative first month was 85%.
Conclusion:
The least invasive microperc with an optical puncture system appears to be a safe and effective treatment modality in patients with different kinds of stone disease with respect to various features. Although the initial cases were patients with single stones of less than 20 mm, the combined use of this system with other minimally invasive treatment modalities for the management of larger stones is promising.
Introduction
The aim of stone disease treatment is total stone clearance with a single session, performed without injury or with minimal damage. Today, open surgery is used only rarely. Our experience with the minimally invasive modalities shockwave lithotripsy (SWL), PCNL, and flexible ureterorenoscopy is increasing daily. It is almost possible to address every stone disease with these modalities, but all have their inherit limitations. Urologists are still seeking perfection in stone disease treatment, especially in stone burden between 10 mm and 20 mm.
As a result of this search, Bader and associates 7 recently introduced an optical system “all-seeing needle” to puncture the kidney. Desai and colleagues 8 recently reported the first series of the microperc, which skips the tract dilation step, and thus a new player is added to the table in the management of stone disease.
In this study, we report our initial experience with microperc for kidney stones and additionally for bladder stones in two patients. To our knowledge, we present the initial report of using microperc in bladder stone treatment.
Patients and Methods
During the 1-month period from April 2012 to May 2012, microperc was performed in 11 consecutive patients at our hospital. Of those 11 patients, 9 had renal and 2 had bladder stones. Patients were divided into two groups according to the origin of the stone disease: Group 1 patients (n=9) were treated for renal stone disease while those in group 2 (n=2) were treated for bladder stone with microperc.
Medical records of each patient of group 1 were reviewed to determine age, sex, location, stone size, mean operative time representing the initial cystoscopy, retrograde catheter placement, and the time needed to turn the patient in the prone position until the end of the procedure, including Double-J stent insertion. The degree of hydronephrosis determined according to the Society for Fetal Urology classification, intraoperative complications, postoperative hospital stay, and stent requirement were also reviewed. The stone clearance was assessed by ultrasonography and/or kidneys-ureters-bladder radiography at the postoperative first month.
For group 2, the medical records were reviewed for age, sex, stone size, mean operative time, intraoperative complications, duration of catheterization, and postoperative hospital stay.
Technique for renal access
Under general anesthesia, a ureteral catheter was placed transurethrally. Then, the patient was converted to the proper position, and percutaneous access was obtained by placement of 4.85F all-seeing needle (PolyDiagnost, Pfaffenhofen, Germany) (Fig. 1) with optical guidance under fluoroscopic or ultrasonographic guidance into the appropriate calix. Surgeon controlled irrigation system (IP 200, PolyDiagnost, Pfaffenhofen, Germany) or 20-mL was used for irrigation. 7
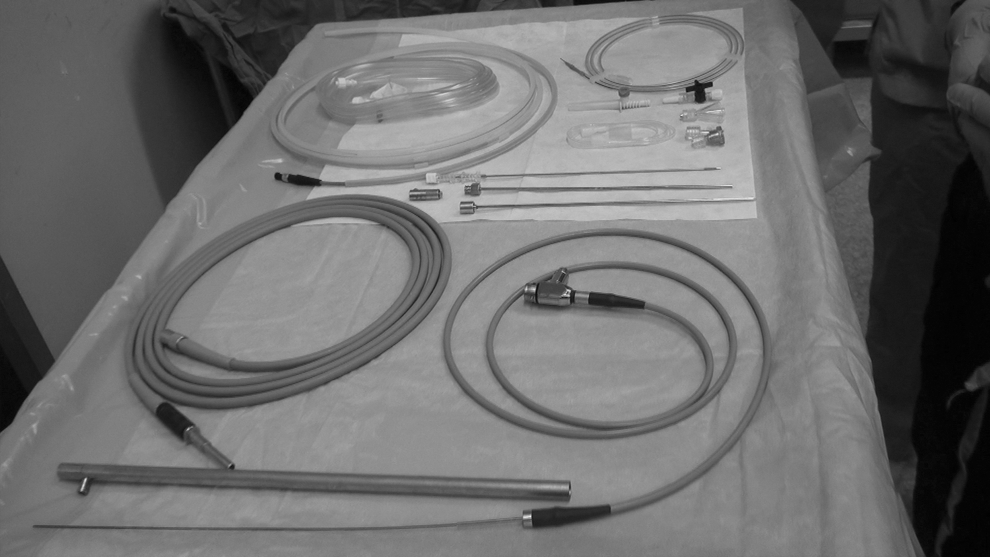
The “all-seeing needle” with the equipment.
The inner needle was removed. A three-way connector was attached to the proximal end of the sheath. The telescope was passed through the connector side port, and the other side port was used for irrigation. The connector central port was used to pass the laser fiber. The calculus was then fragmented by a holmium: yttrium-aluminum-garnet (YAG) laser using a 200 μm fiber (Figs. 2, 3).
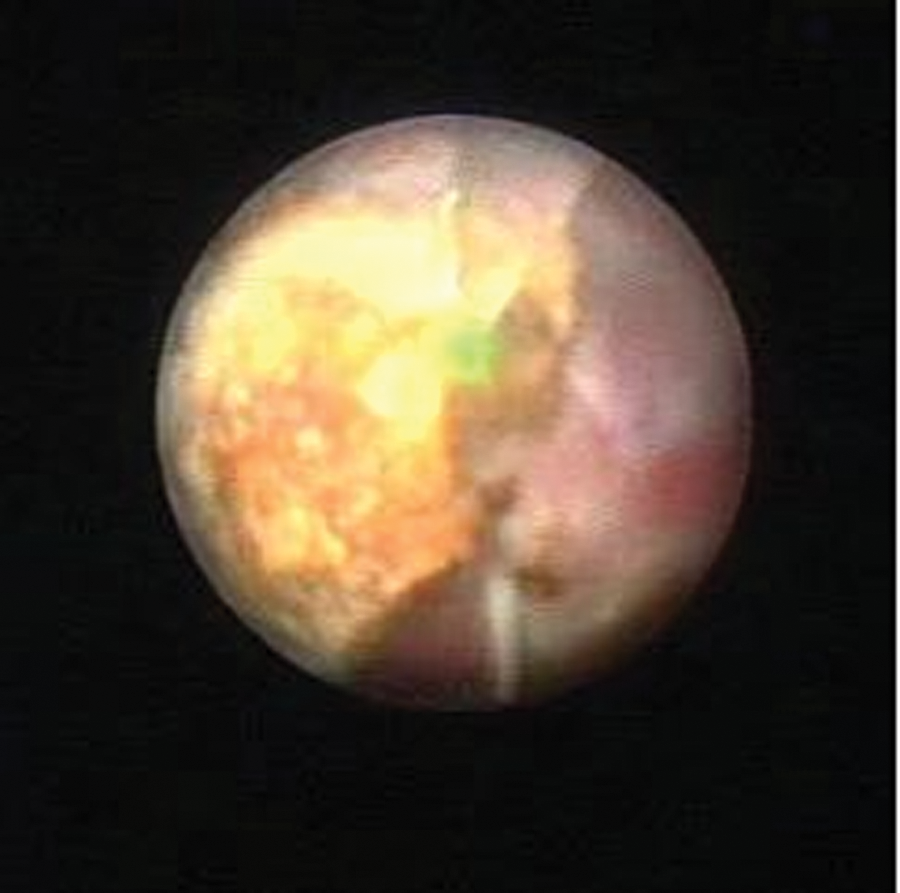
Internal endoscopic view of laser lithotripsy during microperc.

Overview of the operating room during microperc.
At the end of the procedure, we monitored the fragmentation by fluoroscopy.
Technique for bladder access
Under general anesthesia with the patient in the lithotomy position, a urethroscopy was performed with an 8F pediatric cystoscope, and the bladder was filled with saline in pediatric patients. The 4.85F all-seeing needle was inserted in the bladder 1.5 cm above the symphysis pubis. Access of the needle was controlled by cystoscopic view. In adult patients, the bladder was filled with saline with a 6F ureteral catheter; then access of the all-seeing needle to the bladder was achieved by ultrasonographic guidance 2 cm above the pubic bone. In a second case, a transurethral endoscope was not used.
The needle was prepared for stone fragmentation as was described in the kidney stone management section. Fragmentation was performed by holmium:YAG laser. A transurethral catheter was placed at the end of the procedure and removed on the postoperative first day.
Results
Microperc was performed in four female and seven male patients. Of those 11 patients, 9 treated for renal stones represented group 1.
For group 1, the mean age was 20.8 years (range 3–47 years). Access was achieved by all-seeing needle in all group 1 patients. In two patients, we converted to miniperc because of technical problems/operator error. Those two failures happened in two different surgeons' applications because the laser locking mechanisms did not work properly (misfiring the laser probe within the needle, thus damaging the telescope). The patients who needed conversion to mini-PCNL were excluded from the postoperative analysis. Except for one, all patients in group 1 had a single renal stone. The average stone size was 12.8 mm (range 7–18 mm).
Access to the renal collecting system was achieved under fluoroscopic control in eight patients, while ultrasonography was used in one patient. There were no intraoperative complications. One patient in whom a Double-J stent was not used was admitted to the hospital with renal colic on the postoperative third day and was treated medically without need for any auxiliary operation. We used double-J stents in four patients. Postoperative hospital stay ranged from 1 to 3 days. The overall clearance rate in the postoperative first month was 85% (six of seven cases). Patient characteristics for group 1 are summarized in Table 1.
Group 2 included two males (one child, one adult). The mean stone size was 13.5 mm. Patient characteristics are summarized in Table 2. There were no intraoperative or postoperative complications in group 2.
Discussion
The main purpose of stone management is to clear all stone burden as fast as possible and while doing so to give maximum effort—as in all fields of medicine—to treat the patient with minimal or no morbidity. From open surgery to minimally invasive surgeries, during the progression of stone disease, this fact is always considered.
While introduction of SWL to our daily practice temporarily slowed the development of the PCNL, it was later recognized that SWL was not a panacea. 9,10 Advancement and refinement of technology and experience have aided the maturation of the PCNL procedure. Although factors such as size and localization of the stone have impact on the treatment decision, today PCNL ranks as the most important option in the disease management. 11
While PCNL might be minimally invasive, it is nevertheless invasive. In PCNL, a tract between the collecting system of the kidney and the skin is formed. This tract should be large enough for the nephroscope to visualize the system, thus necessitating tract dilation.1–3 Many questions remain related to dilation of the tract; eg, which dilation method is superior, Amplatz or balloon dilation? Does the tract size matter? The complications seen during the dilation step of PCNL, such as bleeding, are closely related to the tract size. 11 Although the risk of complications are because of the puncture itself or the dilation is not known at the moment. We assume that the skipping of the dilation step would decrease the bleeding complication. Yet, the idea of using miniaturized instruments was based on the same assumption of a lower morbidity because of reduced tract diameter resulting in less renal trauma. 5 We may also speculate that the operation would be shortened; however, to prove this hypothesis, there is a need for randomized prospective studies.
Another issue is use of a postoperative nephrostomy tube. To date, some studies have reported that tubeless PCNL could be performed even in children, 12,13 although it is also underlined that tubeless PCNL cannot be applied to all cases. 13 Thus, this issue remains controversial. Whether tubing is preferred or not, because of the nature of the microperc itself, the procedure would end without nephrostomy tube placement. The necessity of ureteral stent placement might be discussed. In our series, one of our patients who did not undergo Double-J stent placement had postoperative renal colic necessitating rehospitalization. This complication might be related to the stone burden. Larger series with microperc will help to illuminate this issue.
The treatment of lower pole stones is an important issue, and urologists are still seeking perfection. Today, new treatment modalities are available, and these treatment options transform the treatment algorithms. Today, PCNL is accepted as the first treatment choice in lower pole stones over 10 mm. PCNL is used very commonly with a very high stone-free rate. Serious complications of PCNL have been described, however. 1 –3
Another treatment option is retrograde intrarenal surgery (RIRS), which is a minimally invasive surgery that uses natural orifices, and the stone-free rates are 90%. 14 There are some limitations of RIRS in the management of lower pole stones, one of which is the reduction of the deflection angle of the flexible ureteroscope after insertion of the laser probe. The durability of the flexible instrument falls short of expectations at present. The costs of the RIRS are still far from optimal and appear to be a disadvantage of ureteroscopy. 7 Further, there are some concerns regarding the safety of active dilation and access sheath use during orifice dilation in children. 15
Today, although the preference of SWL in the treatment of lower pole stones >10 mm has diminished, it is still used, and the stone clearance rate is less than 60%. 9,10 In addition, there are some concerns regarding the long-term effects of SWL. 16 Currently, the advantages of microperc over SWL would be more accurate targeting for fragmentation, and no concerns for stone hardness. The detractive influence of the lower pole caliceal anatomy on the SWL stone clearance rate, however, might be also a limiting factor in microperc. 9 As well, the active removal of the stones is not possible and another limitation of this new technology.
Desai and coworkers 8 mentioned that a long duration of stone fragmentation might be a disadvantage. In our experience, we only used microperc in a stone size up to 18 mm, and we also experienced the same difficulty. Based on our limited experience, the stone size might be a limiting factor in microperc at the moment, but further studies would facilitate identification of the upper limit of stone burden for microperc.
Another difficulty we experienced was movement of the stone during fragmentation in a dilated collecting system. To overcome this problem, we started laser fragmentation with a painting fashion with low frequency (5–10 MHz) and power (0.5–1 J). This approach also prevents the rupture of stones into large particles that need to be fragmented separately. We performed microperc to bladder stones 12 and 15 mm in diameter; this maneuver may fail in larger stones in a larger scope of bladder.
The intrarenal pressure during microperc, which is also a limitation of RIRS, might be a limiting factor. An ex vivo study demonstrated that the irrigation system creates 50 mm Hg pressure with a flow rate of 16 mL/min and 100 mm Hg pressure with 23 mL/min by using physiologic saline (0.9% NaCl) when the optic is within the needle. 7 To clarify the concerns regarding this, intrarenal pressure should be evaluated during the procedure in a further study soon.
Ureteral access sheath use might be more helpful to decrease the intrarenal pressure than an open-ended ureteral catheter. There are studies, however, that report that the access sheath increases the intraoperative complication risk—further, more especially in children leading to ureteral stricture 1% to 4%. 17
Although open surgery still has a role—especially in children—in the treatment of bladder stones, endoscopic bladder stone treatment is used widely. 18,19 The endoscopic interventions could be divided roughly into two subgroups: Transurethral or suprapubic interventions. The transurethral interventions have long been used in both children and adults. Bladder neck injury and secondary urethral strictures, however, are potential complications. 20 On the other hand, while suprapubic percutaneous cystolithotomy can avoid the urethral trauma, suprapubic tract dilation is necessary, which leads to important complications such as intra-abdominal fluid leakage and ileus. 20,21
The application of the microperc skips the dilation of the suprapubic tract, as when used in kidney stones. Microperc for bladder stones enables elimination of the risks of transurethral treatment complications. Furthermore, potential risks of the suprapubic approach, such as extravasations during dilation, would be minimized with microperc. Microperc might be an alternative in bladder stone management in infants, especially males, instead of the suprapubic approach with narrow urethra or transurethral approach with calibration.
Conclusion
The least invasive microperc with optical puncture system appears to be a safe and effective treatment modality in patients with different types of stone disease with respect to different features, if the patients are selected properly and the surgeon performing the procedure has the necessary experience. Although the initial cases were patients with single stones of less than 20 mm, microperc has a great potential in kidney and bladder stones, in which this system can also be combined with other minimally invasive treatment modalities. More studies with a higher number of participants are needed to define the place of this treatment modality, especially for stones of less than 20 mm, which represent the most controversial group in stone disease.
Footnotes
Disclosure Statement
No competing financial interests exist.