
Abstract
Preservation of continence and sexual function continues to be a formidable quality-of-life issue regarding outcomes after radical prostatectomy. There is little argument that physical preservation of the nerves and sphincters is a critical component to achieving success in these domains. Previously demonstrated factors such as advancing age, deteriorating physical health status, and subnormal baseline potency negatively impact outcomes. Our hypothesis, however, has been that inflammatory response to surgery has a large impact on surgical outcomes of prostatectomy.
Trauma-induced inflammation could account for variation in recovery despite nearly identical surgery on many patients, especially in high-volume surgeons. In other words, we suggest and maintain that younger and healthier patients tolerate and/or recover better from the trauma/inflammation of surgery. Those who do not recover as well may have altered inflammatory response to injury. A common response to decrease inflammation in response to physical injury would be as simple as to cool the injury with ice. Previous neurologic studies have suggested that using ice during surgical intervention can reduce the inflammatory damage. Therefore, we applied this concept that preemptive hypothermia could reduce inflammation to the robot-assisted prostatectomy procedure to potentially lead to improved continence and potency outcomes.
In 2009, we introduced the concept of regional hypothermia via an endorectal cooling balloon during robot-assisted radical prostatectomy (RARP). We have published our single institution data demonstrating a significant reduction of overall incontinence. Defining continence as zero-pads, our overall 1-year incontinence has been reduced by 70% (from 13% to 4%). Severe incontinence, defined as two or more pads, was likewise reduced by 70% (from 2.9% to 0.9%). Regional hypothermia used during the time of surgery represents a novel strategy for minimizing inflammation and subsequent muscle and nerve damage in RARP.
Methods
Indications and contraindications
Potentially, endorectal cooling balloon (ECB) hypothermia can be applied in men who present for robot-assisted radical prostatectomy (RARP), except where rectal or anal compromise is confirmed or suspected. For example, if one suspects rectal or anal stenosis such that the catheter or balloon might damage or tear the rectum, it should not be used. We have no problems, however, in men with active history hemorrhoids. We have also used it safely in men undergoing salvage radical prostatectomy after previous radiation therapy.
Preoperative preparation
A thorough history and physical examination including rectal examination should be performed to identify those patients with contraindications before surgery. The other major consideration is for the rectum to be free of stool, because stool content can inhibit the transfer of heat to the ECB. All patients need to have a cleansing rectal enema the night before or the morning of surgery.
Instrumentation
Nondisposable

UroCool Machine (Celsius Control Console).

UroCool Endorectal Balloon Catheter (EBC).
Surgical Steps
Preoperative
Components
(1) Food and Drug Administration approved Celsius cooling console (size of a small refrigerator) is used to cool (∼4°C), pump, and circulate saline. (2) UroCool circulating set is designed for 10 uses and includes a heat exchanger, circulating pump, and sensors and tubing that connects to the ECB. (3) The ECB is a single-use catheter approximately 20 inches in length with two balloons. The smaller inner balloon (30 cc) circulates the 4°C saline and cools the outer balloon. The outer balloon is adjustable and holds up to 150 mL. We recommend inflating to 100 cc, which can be adjusted up or down as needed. There is also a thermistor attached to the outer balloon, which is connected to the anesthesia control cart for continuous monitoring of rectal wall temperatures.
The Celsius control console and components should be prepared before the initiation of surgical preparation. The UroCool circulating set is designed for 10 applications. The heat exchanger coil, circulating pump, and sensor block are inserted into the top of the Celsius control console. The supply (blue) and return (yellow) tubing lines are connected to the single-use ECB. There are color-coded adaptors that connect with the supply or outgoing blue tubing line that carries ∼4°C saline to the inner balloon of the ECB and a yellow adaptor and tubing returning the saline from the ECB that forms a complete closed circuit (Fig. 3). The console is turned on and purged of all air pockets. The inner balloon of the ECB continuously circulates a supply of cooled (∼4°C) saline and, in essence, cools the outer balloon, which can be adjusted from 0 to 100 mL of saline. The combination of the two balloons “sucks the heat” out of the region. Real-time temperature readings are captured on the anesthesia console by a thermistor affixed to the outer balloon (Fig. 2).

The UroCool machine has color coded tubing for easy labeling and assembly.
After a lubricated digital rectal examination and mild dilation, an additional 60 mL of lubrication is injected into the rectum. All connections from the ECB to the Celsius control console have been connected, and tubing will run underneath the leg of the patient, who is in the lithotomy position. The lubricated ECB is inserted directing the catheter tip toward the center of the rectal lumen following the normal rectal curvature. The catheter is inserted such that the balloon is just inside the anal sphincter. The outer balloon is then filled with 100 mL of saline. Routinely, however, we have used 60 to 100 mL. The Celsius control console can now be placed in the “RUN” mode to cycle cooled physiologic saline. The video (Supplementary video available online at
Suggestions
Do not force the rectal catheter at any time. If difficulty is encountered while inserting the ECB, use your finger to guide and maneuver the tip away from the rectal wall.
Intraoperative management
Temperatures from the ECB/rectal wall as well as core temperature are monitored continuously throughout the case. All patients are protected with usual intraoperative warming techniques of the upper chest and arms. We have not seen any major change (>2°C) in the core body temperature during regional hypothermia. In addition to the cooling induced via the ECB, we also use cold water irrigation throughout the procedure.
Suggestions
In general, 100 mL in the outer balloon seems to optimally fill the rectum for maximal heat extraction. We recommend that the balloon be reduced down to 70 cc (or less as determined by the surgeon) when dissecting the rectum off of the prostate posteriorly or when dissecting the NVBs off of the prostate. In addition, the first few times the ECB is used, we recommend empiric adjusting of the outer balloon volume so each surgeon is comfortable with ECB volumes and space within the pelvis.
Use of the rectal cooling balloon has not increased intraoperative complications. There have been no rectal injuries in more than 500 cases. If an inadvertent rectal injury occurred, however, a two-layer repair is recommended using standard indications and techniques. The ECB can be deflated or removed as necessary to facilitate surgical repair. If a large rectal injury is made or if the patient had radiation therapy, a diverting colostomy is recommended. Fortunately, the profile of the ECB can be adjusted as needed by withdrawing/instilling saline as necessary.
Postoperative care
The balloon is removed after the skin incisions are closed to maximize cooling time. When ready to discontinue cooling, press “STOP” on the Celsius control console and turn the power off. Disconnect the catheter from the console by disconnecting the yellow and blue adaptors and let liquid from the inner balloon drain into a disposable container. The ECB is deflated completely using a 60 mL syringe. Slowly remove the catheter from the rectum and dispose.
Precautions
If the catheter is not removed easily, do not pull with force. Make sure to check that both inner and outer balloons have been completely deflated.
Management of postoperative complications
Complications have been minimal in our current trial of endorectal regional hypothermia. Patients were queried at the time of discharge (∼24 hours) using the Standard Verbal Descriptor Pain Scale 0 to 10. Of 144 men, 88% reported either mild (28%) or no pain (60%), scale 0 to 2; 10% reported moderate pain, scale 3 to 6; and 3% reported severe/worse pain, scale 7 to 9. Postoperatively, we surveyed 55 men for rectal complaints using the self-reported Expanded Prostate Cancer Index Composite questionnaire. At 1 month postsurgery, 92% of patients reported having only a small, very small, or no problem in all of the bowel function categories: (1) Rectal urgency, (2) uncontrolled stool, (3) loose stool, (4) bloody stool, (5) painful bowel movements, and (6) frequency of bowel movements.
Summary of Published Reports
Concept
The long-term side effects of RARP, including incontinence and impotence, have significant detrimental effects on patient quality of life. 1,2 While a multitude of factors have been implicated, age and health status have the most impact on recovery of continence and potency. 3 While, in essence, the same surgery with the same amount of acute surgical trauma occurs in all age groups, older patients will not recover as well as younger patients as seen in our overall single-surgeon cohort to essentially control for technique. 4 The difference, we believe, is because of the inflammatory response between the two age groups.
The inflammatory cascade includes activation of coagulation factors, proinflammatory cytokine formation, hypoxia, microcirculatory impairment from endothelial damage, acidosis, free radical production, and apoptosis. 5 Neutrophil and macrophage infiltration with subsequent release of proteolytic enzymes further contribute to tissue destruction. 6,7 Theoretically, this secondary inflammatory cascade seems the logical explanation for the delayed damage to the sphincter muscles, pelvic nerves, and the neurovascular bundle, which might be blocked (or at least mitigated) with the use of local tissue hypothermia.
Application of hypothermia preemptively (before dissection starts) prepares tissues for imminent damage by lowering their metabolic rate and oxygen demands. With sufficient temperature reduction, the cell enters into a quiescent state of low energy utilization. When injury ensues, energy reserves are available for repair without reverting to anaerobic metabolism. As a result, less lactate formation occurs, protein synthesis is preserved, and most importantly, the inflammatory cascade is blunted. With fewer proinflammatory molecules and free radical species generated, the risk of apoptotic cell death is reduced. Tissue damage from leukocyte infiltration is further reduced, because cooling also blocks adhesion molecule transcription and inhibits neutrophil adherence. 8
Hypothermia has been demonstrated to have a dramatic protective impact in numerous experimental injury models of the central and peripheral nervous systems. The use of mild to moderate hypothermia (ie, 33°C to 28°C) has been shown to be effective in shielding neurons from damage. In a rabbit model of spinal cord ischemia, Isaka and colleagues 9 applied transvertebral cold packs and infused cold saline into a cross-clamped aorta to produce spinal cord cooling. A modest reduction in spinal cord temperature of just 4.3°C completely prevented paraplegia compared with complete paraplegia in all of the control rabbits.
There is widespread evidence that hypothermia mitigates inflammatory pathways and improves repair mechanisms. Controlled hypothermia impacts a range of biochemical, histologic, and physiologic effects that include a temperature dependent reduction in cellular metabolism leading to reduced energy demands, decreased free radical production, interruption of the apoptotic cascade, and decreased inflammation. 1,10 –17 The protective effects of hypothermia have been demonstrated in the nervous system, cardiac system, shock, transplantation, and partial nephrectomy. 9,13,18,19 We have previously reported our results in applying this technique to radical prostatectomy to prevent inflammatory damage allowing improved preservation of continence and potency.
Continence
In our initial feasibility study, we presented the rationale for hypothermia and demonstrated that we could cool the pelvis reasonably well (<30°C) without complications or patient discomfort. 20 In addition, using infrared cameras, we documented cooling of the entire pelvis by using thermal photography (Fig. 4a, 4b). Our most important finding regards the 12-month zero-pad continence of 96%. Time to continence is much more sensitive to bias than documenting no pad usage at 12 months. In our controls, 87% were pad free, and hence our 14% incontinence rate has been reduced to 4%, a 70% reduction. (P<0.001). 4 In addition, we noted that those in older age groups benefited more than those in younger age groups. For example, those patients over 70 years of age who were treated with hypothermia reached 1-year zero pad continence 92% of the time compared with only 72% in the nonhypothermia group. 4
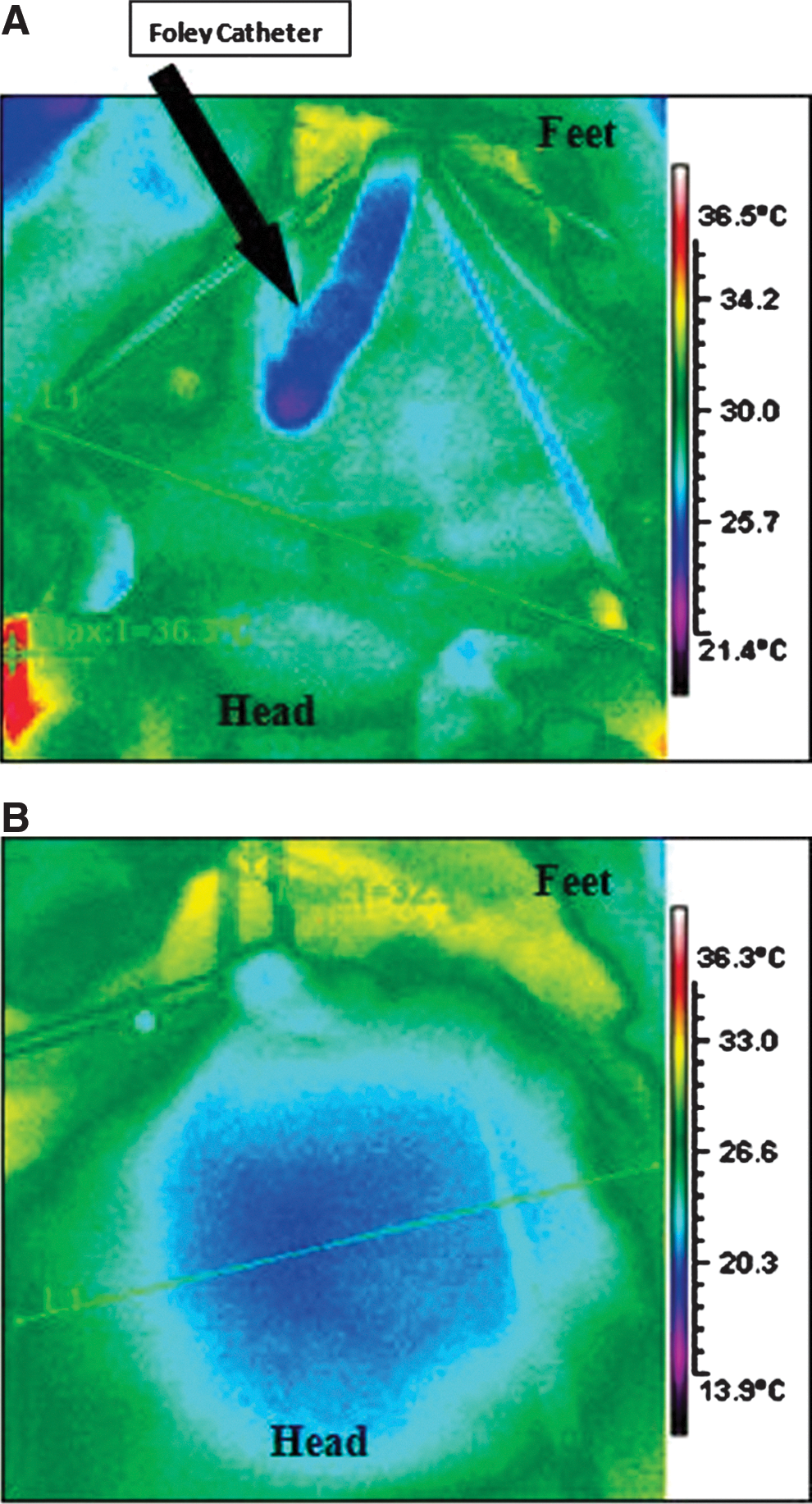
Representative example of hypothermia during open cystectomy with the bladder removed showing pelvic temperatures with and without the cooling balloon activated.
Sexual function
The benefit of hypothermia has been modest. Presently, we hypothesize that the cavernosal nerves are much more difficult to cool. This is because of the major impact of warm arterial and venous inflow limiting the cooling effect of the ECB. At 15 months, we saw a modest but significant improvement in potency recovery in men with normal baseline International Index of Erectile Function-5 scores aged 43 to 78 years (88% hypothermia vs 66% control, P=0.045). Interestingly, men older than 65 years were most impacted, with potency rates improving twofold (30%–70%, P=0.006). 4
Footnotes
Acknowledgments
We wish to thank Esequiel Rodriguez, M.D. and David Finley, M.D. for preclinical and clinical work and their contributions to our understanding of hypothermia.
Disclosure Statement
Presently, regional hypothermia via our endorectal cooling balloon (ECB) is pending patent and Food and Drug Administration approval. The University of California, Irvine, has a patent application for this technology currently under consideration. The University of California, Irvine, has a License Agreement with Philips Health Care, Inc, and use of the ECB and regional hypothermia is restricted.
Dr. Ahlering has grant research support from Philips and Astellas and is a consultant for Intuitive Surgical. For the remaining authors, no competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.