
Abstract
Purpose:
We present our experience in the minimally invasive management of postoperative complications associated with urinary diversions using an ureteral access sheath (UAS) in an antegrade approach.
Patients and Methods:
From 2005 to 2011, 21 antegrade flexible ureteroscopies (F-URS) were performed in 17 patients with a urinary diversion. Urinary diversions in this population consisted of ileal conduits, orthotopic neobladders, catheterizable pouches, and an ureterosigmoidostomy in 9, 5, 2, and 1 patients, respectively. The most important reason for treatment was recurrent upper urinary tract infection. The indication for intervention was stone disease in 15 procedures and strictures in 6 cases. In two patients, “staged-therapy” was performed. Using UAS in an antegrade approach was the main concept.
Results:
A nephrostomy tube was already in place in 14 (66.6%) procedures, which was the access route used. Successful puncture was performed in all other patients. Eighty percent of patients were rendered stone free after the first antegrade session. Moreover, all strictures were successfully managed by dilation. In two sequential procedures in a patient, there was an inability to perform stone treatment because of abnormal position of the ureter (kinked), which did not allow the ureterorenoscope to pass. All other procedures were uneventful. Postoperative complications were reported in four procedures. There was significant urinary tract infection in two patients as well as an obstructed nephrostomy tube in two patients.
Conclusion:
An antegrade endoscopic procedure using UAS in patients who present with stones or ureterointestinal stricture as late complications of urinary diversion is a feasible, well-tolerated technique, especially when using smaller access sheaths.
Introduction
Radical cystectomy is currently the gold standard for management of muscle-invasive bladder cancer as well as for recurrent high-risk nonmuscle-invasive bladder transitional-cell carcinoma with failure of adjuvant intravesical therapy. 1,2 It is considered as the main indication for a urinary diversion, that can be of different anatomic subtypes: Abdominal (usually with Bricker ileal conduit or catheterizable pouches), urethral (orthotopic neobladders ), or rectosigmoid (ureterosigmoidostomy). A French national survey published in 2008 revealed that ileal conduit was performed as a urinary diversion in 84% of patients, even if a trend toward the use of more complex and continent forms of diversions was seen. 3
Major complications after radical cystectomy and abdominal urinary diversion are well known and have been reported to range from 20% to 56% during the first postoperative month and from 28% to 81% afterward in the case of ileal conduit. 4 In addition, morbidity was reported up to 57% with continent catheterizable pouches. 5 For many reasons, including metabolic derangements, urinary infection/colonization, and structural factors, patients are at increased risk of urolithiasis of the upper urinary tract, the reservoir, or the conduit. 6 Surgical management of stones in these cases can be highly challenging, with no clear consensus or algorithm about the best approach among percutaneous nephrolithotomy, shockwave lithotripsy (SWL), or retrograde or antegrade ureteroscopy. Furthermore, ureteral stricture disease is not uncommon after urinary diversion, leading to potential increased technical difficulties.
The goal of our study was to describe an antegrade endoscopic technique for the management of the complications associated with urinary diversion. In addition, we detail the use of and ureteral access sheath (UAS) as one of the tips and tricks that can facilitate the management of these complications.
Patients and Methods
Population description
We retrospectively identified 17 patients (7 women and 10 men) with a urinary diversion who underwent antegrade percutaneous endoscopic treatment between 2005 and 2011 in a single tertiary reference center for stone management. Mean age was 51 years (range 32–79years). Mean±standard deviation body height, body weight, and body mass index were 166±7 cm, 87±5.2 kg, and 33±4.1, respectively. The main reason for urinary diversion was muscle invasive bladder cancer, present in 12/17 (70%) patients. In five patients, urinary diversion was performed because of a history of bladder extrophy, or neurogenic bladder refractory to medical management. Urinary diversion types are described in Table 1.
Patient Characteristics
Median time between urinary diversion surgery and percutaneous surgery was 12.7 years. Previous urologic interventions for stone treatment were performed in six (35.3 %) patients. Retrograde endoscopic procedures had failed in three patients, and three patients had undergone SWL. The indication for intervention was stone disease in 15 procedures and strictures in 6 cases. Patients' presenting symptoms consisted mostly of recurrent urinary tract infections. One patient, however, presented with renal colic pain and another was found to have an asymptomatic stone during regular follow-up. Stone size ranged from 6 mm to 20 mm with a mean size of 13.4 mm. There were 10 (58.8%) patients with a nephrostomy tube at the time of the first procedure (Table 2). All patients had either sterile urine culture results or they were treated according to the antibiotic sensitivity tests preoperatively.
Upper Urinary Tract Characteristics
UIS=ureterointestinal stricture.
Surgical procedure
Urologic instrumentations were performed under general anesthesia with the patient in a modified supine position with elevation of treated side. The modified Valdivia supine position was needed, however, in patients with orthotopic bladder (Fig. 1). Optimal percutaneous access was performed under ultrasonographic guidance and/or fluoroscopic guidance. 7,8 If a nephrostomy tube was in place, a guidewire was placed under fluoroscopic guidance. A safety wire was introduced with the use of a double-lumen catheter (Cook Medical, Bloomington, IN).

Patient in the supine position, sterile drape for percutaneous access, and the urinary diversion stoma.
Kidney stones management
Dilation with a high-pressure balloon (Nephromax, Boston Scientific, Natik, MA) was performed. A 28F or 30F Amplatz sheath was placed afterward. In some cases, a flexible nephroscope was used to explore the entire urinary collecting system, if possible.
Ureteral stones and ureterointestinal strictures (UIS) management
A 0.035-inch polytetrafluoroethylene-coated hydrophilic guidewire was introduced in the ureter through the percutaneous access and dilation was performed. A UAS (9.5–11.5F or 12–14F UAS [Cook Medical] or 11–13F UAS [Boston Scientific]) was inserted under fluoroscopic control in the ureter over the guidewire, allowing us to pass the endoscope (Figs. 2 and 3). Stone disintegration was performed with a holmium:yttrium-aluminum-garnet (YAG) laser under endoscopic vision with good quality irrigation. Then, a nitinol basket was used to mobilize and extract any fragments. In the case of UIS (Fig. 4), a flexible ureteroscope was introduced to visualize the stricture, then to pass a guidewire through the stricture under vision. A holmium:YAG laser incision was then performed in a safe manner.

Insertion of flexible ureteroscope through the ureteral access sheath.
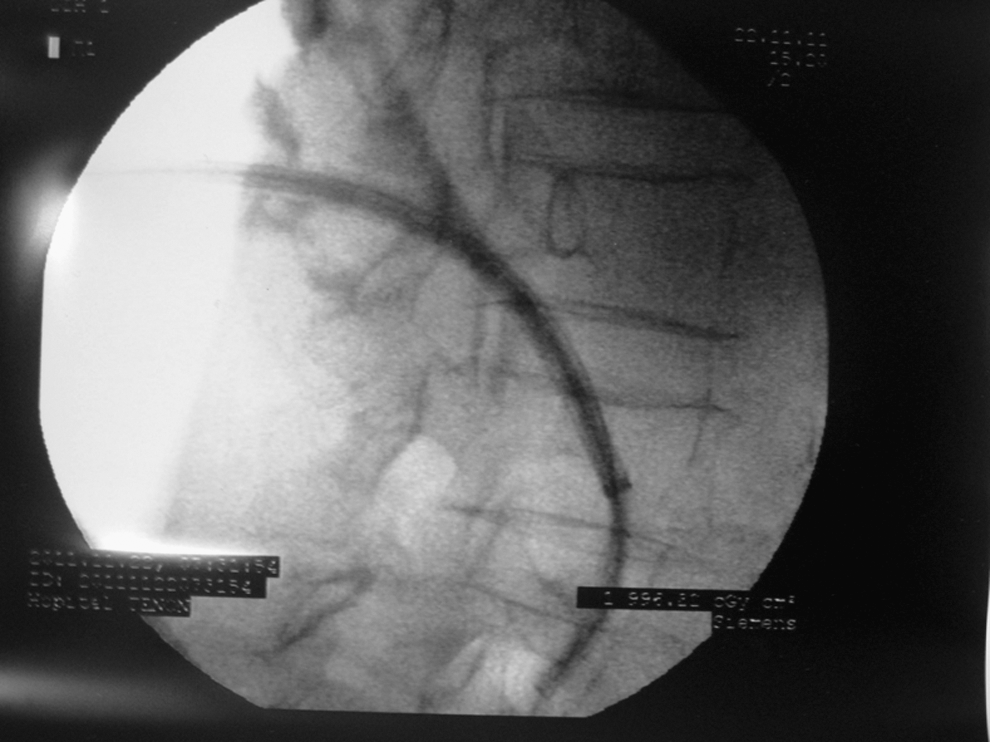
Insertion of flexible access sheath through the ureteral access sheath (fluoroscopy).

Endoscopic vision of ureterointestinal stricture.
Balloon dilation with UroMax (Boston Scientific—4 cm length, 15F size—was performed for all strictures. Placement of a Double-J stent—7F, 30 cm length—in antegrade fashion or a 9F Mono-J stent in retrograde fashion was performed according to the urinary diversion. In all cases, a clamped nephrostomy tube was left in place as a security access. Absence of fever and/or renal colic pain allowed us to remove the nephrostomy tube 24 hours postoperatively if no second look was needed.
Follow-up
Patients were followed in an outpatient setting with renal ultrasonography or noncontrast CT at a 1-month visit. Removal of the Double-J or Mono-J stent was performed 6 to 8 weeks postoperatively, depending on patient and appointment availability. All UIS cases underwent an ultrasonography control 6 weeks after removal of the stent in our center. Control ultrasonography was performed again at 6 months. Long-term follow-up was performed by the referring urologists who addressed the patient.
Results
A total of 21 procedures were performed in 17 patients. In seven patients, puncture was successfully established with fluoroscopy and/or ultrasonographic guidance. Lower pole puncture was mostly performed with no impact on the outcome. Percutaneous access dilation was performed in all procedures.
There were 82.3% of patients with stone disease who were rendered stone free after the first antegrade procedure and all strictures could be passed and dilated. Stone disintegration was performed by holmium laser in 50% of patients, and extraction of small fragments was performed in 10 (58.3%) patients using a nitinol basket. In two patients, “staged-therapy” was performed because of inability of stone manipulation in a kinked ureter. Average operative time was 77 minutes (range 30–119 min). Mean hospital stay was 4.2 days (range 2–7days). Postoperative complications were reported after four procedures. In two cases, significant urinary tract infection was treated successfully with appropriate antibiotics. In the other cases, hematuria was documented and resolved spontaneously.
Discussion
After urinary diversion, anastomotic stricture, conduit stenosis, and/or metabolic disturbances resulting in stone formation are not uncommon. The disturbances in acid-base balance can occur because of bowel wall secretion and urinary reabsorption and are influenced by the type and the length of bowel segment used for urinary diversion. Chronic bacteriuria is reported in 50% to 90% of urinary diversions and leads to an increase in the stone burden formation. 9,10 The incidence of renal stones and benign strictures in ileal conduits has been described as high as 15.3% and 7% to 14%, respectively, whereas approximately 13% of patients harbor metabolic abnormalities in contemporary series. 11,12 Metabolic acidosis has been described in most patients with orthotopic bladder in the early postoperative period, often necessitating oral substitution. 12
Despite the fact that a majority of patients have an ileal conduit as a urinary diversion, there is a tendency to increased use of orthotopic and continent diversions. 1 –3 The latter often require longer intestinal segments, which could potentially increase the complication rate. Because complications related to stone and stricture formation can cause significant morbidity and can potentially lead to renal failure, timely diagnosis and management is mandatory. 6 None of the currently available surgical options for stone management (open procedure, percutaneous nephrolithotomy, and flexible ureteroscopy (antegrade or retrograde), however, has proven to be the universal rescue for these challenging cases. SWL monotherapy has been described as a nonsurgical and valuable option. Nevertheless, secondary procedures were necessary in 18.5% because of drainage dilemma. 13
In recent years, great advances in endourologic instrumentation and miniaturizations increased the role of endoluminal treatment of stone disease. The retrograde approach in urinary diversions may be technically demanding because of an absence of anatomic landmarks. Retrograde introduction of an UAS over a guidewire can be limited by anastomotic strictures as well as changes in the ureteral anatomic axis; some authors reported that open surgical treatment was often needed. 14 Therefore, in these cases, an antegrade endoscopic approach is a good alternative.
With the advances in the endoscopic field, miniaturization and use of holmium laser, ureterorenoscopy has become an acceptable approach for upper urinary tract stones. 15,16 UAS in an antegrade fashion was the new and the main concept of our technique without any difficulties. Moreover, several urologists have recently promoted the use of laser endoureterotomy for stricture management. 17 The major advantages of using laser for UIS include: Laser provides clear vision during incision so that UIS is incised more precisely, provokes less bleeding, is associated with a shorter hospital stay, and possibly there isless scar tissue after healing.
Patients who presented with acute urinary tract obstruction and urinary tract infection were treated with an immediate nephrostomy tube. This drainage was necessary because of progression to renal failure, hydronephrosis, pyonephrosis, or urosepsis. In our experience, this percutaneous access could then be used as a therapeutic antegrade approach. In the remaining cases, we did not encounter any difficulties to access the ureter from the inferior calix using flexible ureteroscopy after a conventional puncture.
One advantage of the antegrade flexible ureteroscopic approach over the retrograde flexible ureteroscopic approach is that percutaneous access is created before the procedure; moreover, it is known to give reliable access to the upper urinary tract and to allow good irrigation with a faster passage of small significant fragments better than the retrograde approach.
The feasibility and safety of this minimally invasive antegrade approach was demonstrated in 82.3% of patients, because they rendered stone free after the first antegrade procedure. Complications were minor and successfully managed. Longer postoperative stay can be explained by second look or “staged-therapy” at the same hospitalization. Regular follow-up is needed to prevent stone formation and to manage stones when stone burden is still small.
Albeit our reports could assess the feasibility and an acceptable success rate of the antegrade approach in these difficult cases, it has a number of limitations. First, metabolic changes have to be observed and treated to prevent stone formation. Stone analysis is recommended in all cases; unfortunately, we did not obtain this information in this retrospective chart review. Then, our experience comes from a single tertiary reference center that may not reflect perfectly standard urologic practice. Finally, a systematic comparison of the antegrade approach and other therapeutic options would be the only definitive way to state what would be the best option to manage these complex situations.
Conclusion
An antegrade endoscopic procedure using UAS in patients who present with stones or UIS as late complications of urinary diversion is a feasible and well-tolerated technique. Dilation with the use of a small UAS provides good access to the ureter and allows good inspection. Endoscopic laser stone disintegration and stricture incision with balloon dilation could be performed in a majority of procedures. In the case of recurrence, certain secondary procedures seem affordable.
Footnotes
Disclosure Statement
Olivier Traxer is a consultant for Coloplast, Rocamed and AMS. For the remaining authors, no competing financial interests exist.