
Abstract
Pelvic lymphadenectomy for prostate cancer is an important tool in the prognostication of the disease in selected patients who are at risk of occult lymph node metastases. This procedure, usually performed in conjunction with radical prostatectomy, had progressed successfully from an open approach to the current robot-assisted approach. The following article and accompanying video describe the surgical technique of robot-assisted pelvic lymphadenectomy for prostate cancer. We also discuss the indications, patient selection, preparation, complications, and tips to avoid the major pitfalls in the procedure.
Introduction
Methods
Indications
The role of lymphadenectomy in prostate cancer is still the subject of much debate. 2 –4 The controversies center around identifying the risk group of the disease for which the procedure should be performed and the extent to which the dissection should be performed. Various studies have looked into these issues, and these will be discussed briefly later in this article.
The benefits of lymphadenectomy in localized prostate cancer are twofold: (1) Accurate prognostication of the risk of progression and/or recurrence based on pathologic evidence of regional nodal spread and (2) to assess the need for adjuvant treatment based on possible survival or progression-free benefits. 5,6 There is some limited evidence that this may also have some therapeutic benefits in a subset of patients. 7,8 The indication for pelvic lymphadenectomy in localized prostate cancer after prostatectomy will therefore be those who are presumed to be at significant risk of occult nodal spread.
The criteria for selection for these patients differ according to the various guidelines. The National Comprehensive Cancer Network states that lymphadenectomy may be omitted if the nomogram-assessed risk of nodal spread is less than 2%. The European Association of Urology guidelines put this cutoff as 5% but also included all high-risk patients (defined as cT3a or Gleason score 8–10 or prostate-specific antigen (PSA) level >20 ng/mL). The American Urological Association Best Practice Statement on PSA excludes patients whose PSA levels are less than 10.0 ng/mL and the Gleason score is less than or equal to 6.
D'Amico and colleagues 9 stratified localized prostate cancer into three risk groups based on the probability of disease progression after primary definitive therapy in 1872 men. These risk groups are commonly used to categorize localized prostate cancer for diagnostic, therapeutic, and follow-up purposes. We find this classification a useful adjunct in deciding the need to perform lymphadenectomy. In the absence of consensus on this issue, our practice at Indiana University has been to perform bilateral pelvic lymphadenectomy in all patients with D'Amico high-risk disease or any patient with intermediate-risk disease with 50% or more involvement of any core biopsy. While there are emerging data that the frequency of nodal metastases is higher than previously recognized even in low-risk patients, we have not found this in our low-risk patients even with extended pelvic lymph node dissection (PLND). 10,11
Contraindications
Patients with a diagnosis of overt distant metastases on preoperative evaluation will not be candidates for locoregional extirpative surgery. These patients should be considered for androgen deprivation therapy to control the systemic disease. Most urologists would consider the presence of nodal metastases as a contraindication to surgery because these patients would eventually fail treatment and need further adjuvant therapy. Such patients can have excellent disease control with external beam radiotherapy with concurrent long-term hormonal therapy as the primary form of treatment. 12,13 Conversely, large retrospective studies had also shown potential benefit of lymphadenectomy during prostatectomy even for node-positive disease, although the majority of patients would need some form of adjuvant therapy. 14,15
Comorbidities that preclude robot-assisted pelvic lymphadenectomy after prostatectomy include severe cardiac or pulmonary diseases. Such patients will not tolerate the pneumoperitoneum and extreme Trendelenburg position needed for the procedure. Other contraindications include uncorrected coagulopathy, recent episode of deep vein thrombosis, or pulmonary embolism. Furthermore, we generally would not perform lymphadenectomy in patients with previous pelvic radiotherapy or previous pelvic vascular grafting.
Preoperative workup
Routine preoperative workup include blood tests for creatinine, electrolytes, complete blood cell count, coagulation profile, and chest radiography. Active urinary tract infection should be excluded before surgery. Appropriate antibiotics should be started and a negative culture obtained before the patient undergoes surgery. Patients with high-risk prostate cancer should undergo contrast-enhanced abdominal and pelvic CT to rule out regional lymphadenopathy and radionuclide bone scan to rule out bone metastases.
Patient preoperative preparation
On the day before surgery, the patient is advised to take light meals, and the bowel is cleared with a laxative. The patient fasts from midnight onward. A single dose of cephalosporin is given at induction of general anesthesia. The patient is placed in the lithotomy position, and pneumoperitoneum is created using the Veress needle to a setting of 15 mm Hg. Trocars are placed for RALP as shown in Figure 1. We use four arms of the da Vinci Si system (Intuitive Surgical Inc, Sunnyvale, CA) in this surgery. The initial 12-mm trocar is placed in the midline just above the umbilicus. Under direct vision, two 8-mm trocars are placed 8 cm from the midline on either side of the umbilicus. A third 8-mm trocar for the fourth arm is placed 8 cm lateral to the left arm trocar. Lastly, a 12-mm trocar for the assistant is placed 8 cm lateral to the right arm trocar. The patient is placed in the Trendelenburg position, and the da Vinci patient cart is docked.
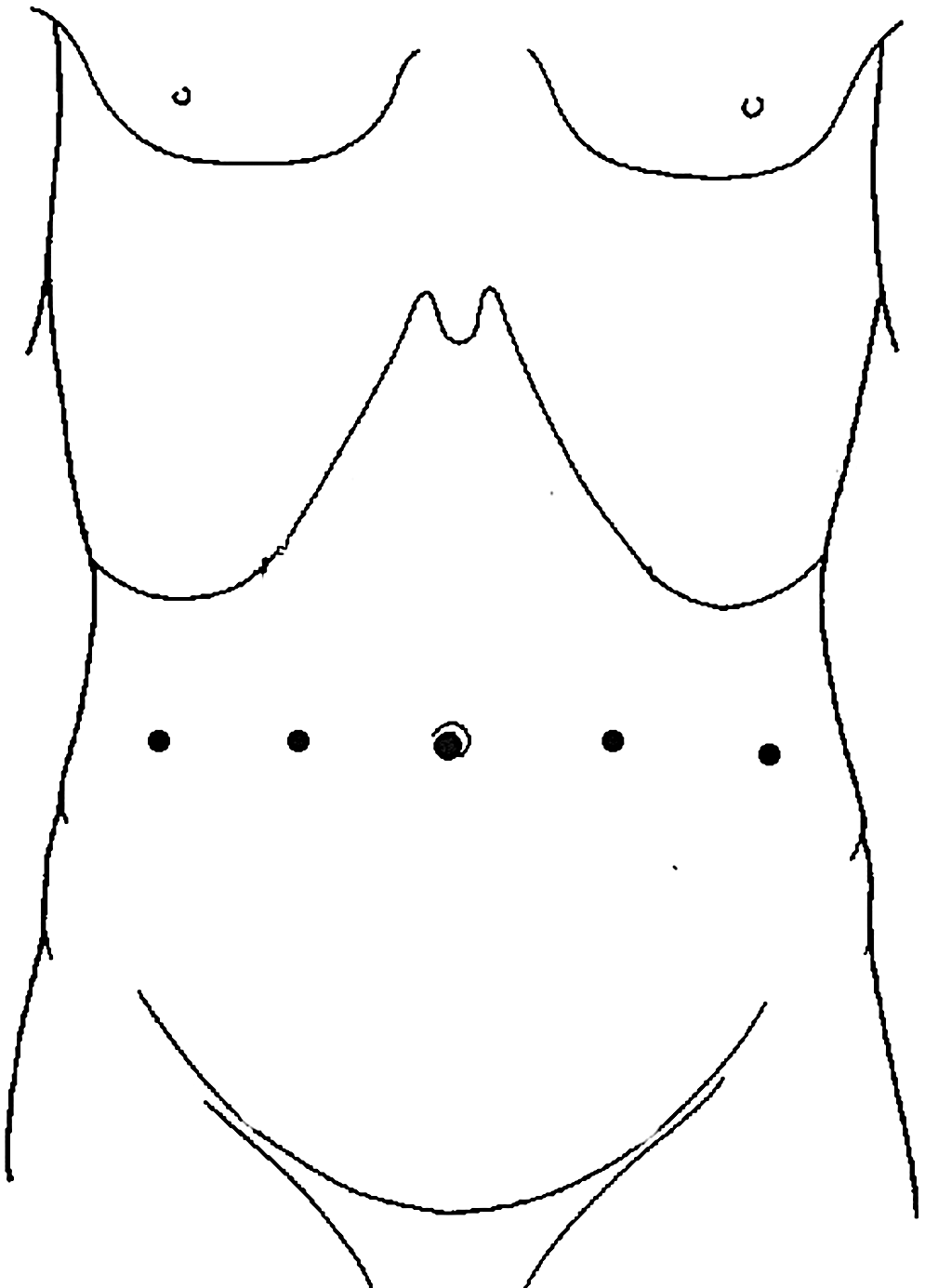
Position of trocars set up for robot-assisted laparoscopic prostatectomy at Indiana University.
Instrumentation
Nondisposable
The same robotic instruments used for prostatectomy are used in pelvic lymphadenectomy. We use the da Vinci Hot Shears™ (Intuitive Surgical Inc) and PK™ (Plasma Kinetic, Gyrus ACMI) dissecting forceps in the right and left hands, respectively, for sharp and blunt dissection. The da Vinci Large Clip Applicator ™ may be used to ligate lymphatic pedicles with Hem-o-lock clips (Teleflex, Research Triangle Park, NC). The PK dissecting forceps may be used to seal small lymphatic and blood vessels.
Disposable
The assistant uses the Stryker Flow 2 suction irrigator through the 12-mm trocar on the right.
Surgical Steps
Identifying surgical landmarks
We routinely perform prostatectomy before pelvic lymphadenectomy and before urethrovesical anastamosis. Pelvic lymphadenectomy can also be easily performed before prostatectomy according to surgeon and patient preference. The surgical landmarks to identify before incision of the peritoneum are shown in Figure 2. In developing the space of Retzius, the peritoneum is incised from a point lateral to the medial umbilical ligament and extends inferolaterally across the vas deferens to a point about 3 cm from the common iliac vessels. The vas deferens is divided in this process. After the prostate has been removed and hemostasis achieved in the prostate bed, the anatomy is reassessed to identify the important landmarks such as the ureter and common iliac vessels. The fourth arm is used to retract the bladder medially and apply tension to the superior vesical artery, thus separating the bladder from the lateral nodal packet. Minimal suction is needed from the assistant other than to evacuate blood and lymphatic fluid from the field.
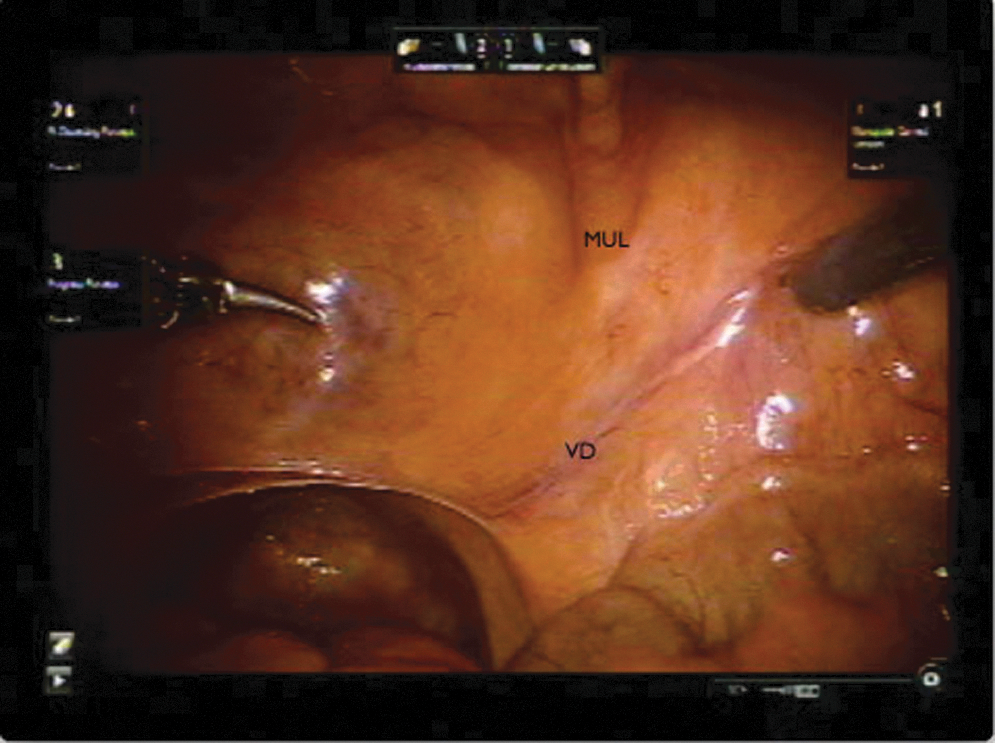
Surgical landmarks to be identified at the start of surgery including medial umbilical ligament (MUL) and vas deferens (VD).
External iliac dissection
We start with the lateral limit of dissection, which is the external iliac artery. Dissection is avoided lateral to the external iliac vessels, because this area has not been shown to contain positive lymph nodes in anatomic mapping studies. 3 The external iliac vein is identified and skeletonized using blunt dissection. Dissection is carried around the medial and posterior borders of the vein until the obturator internus muscle on the pelvic side wall comes into view. The plane between the vein and the pelvic side wall is developed until the external iliac vein is completely skeletonized.
In the process of dissecting the lymphatic packet off of the external iliac vein, the surgeon will encounter an accessory obturator vein coursing from the external iliac vein to the obturator foramen in at least half of patients. (Fig. 3) Once recognized, the lymphatic packet can be dissected off this accessory vein. Multiple small perforating vessels are almost always present coursing from the pelvic side wall musculature to the pelvic node packet. These are easily secured with bipolar electrocautery and sharp dissection. Superiorly and posteriorly, the dissection is very close to the hypogastric vein. The proximal limit is marked by the crossing of the ureter where the lymphatic packet is divided (Fig. 4).
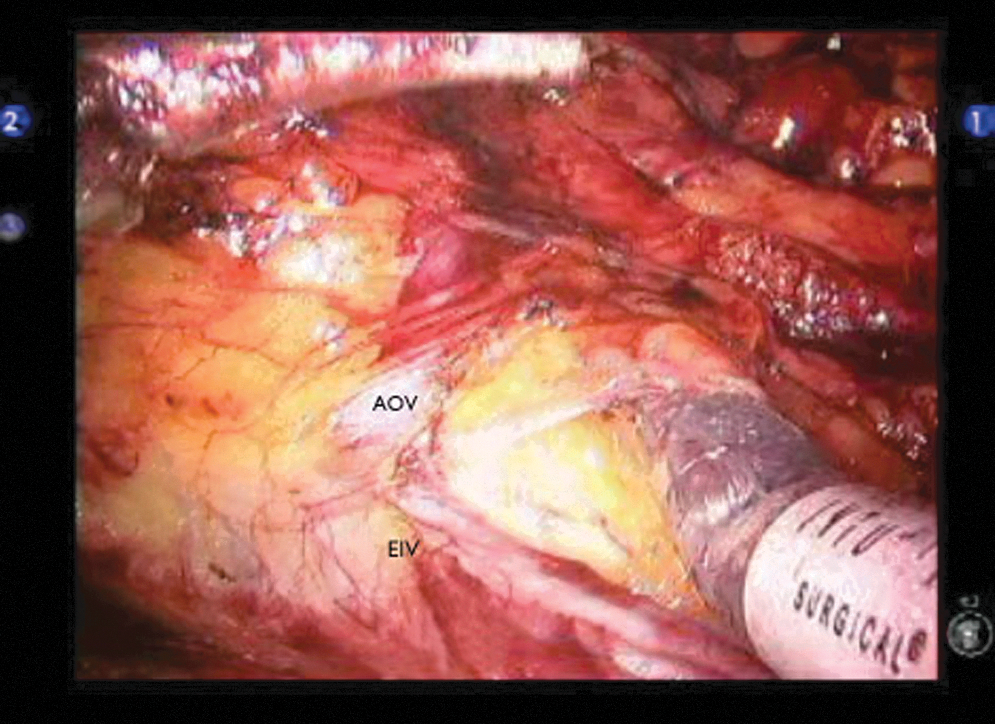
Accessory obturator vein (AOV), branch of the external iliac vein (EIV).

Proximal limit of dissection, showing the ureter and external iliac vein (EIV).
Obturator and internal iliac dissection
Using the fourth arm to retract the bladder further, the plane between the lymphatic packet and bladder is developed. The lymphatic tissue surrounding the internal iliac (hypogastric) vessels is dissected bluntly. The obturator and hypogastric packets are dissected en bloc carefully to expose the obturator nerve. The nerve can be easily exposed by sweeping the lymphatic packet in a direction parallel to the nerve. The nerve is preserved and dissected distally toward the obturator foramen.
During this portion of the surgery, the fourth arm may be adjusted to further retract the bladder medially to maintain tension in the tissue planes. The lymphatic packet can be dissected off the obturator artery and vein or, alternatively, these can be secured with clips or cautery and taken with the lymph node packet with no consequence to the patient. The obturator vessels can be found to travel toward the obturator foramen medial to the nerve (Fig. 5). The lymphofatty packet in the perirectal region is also included in this dissection.
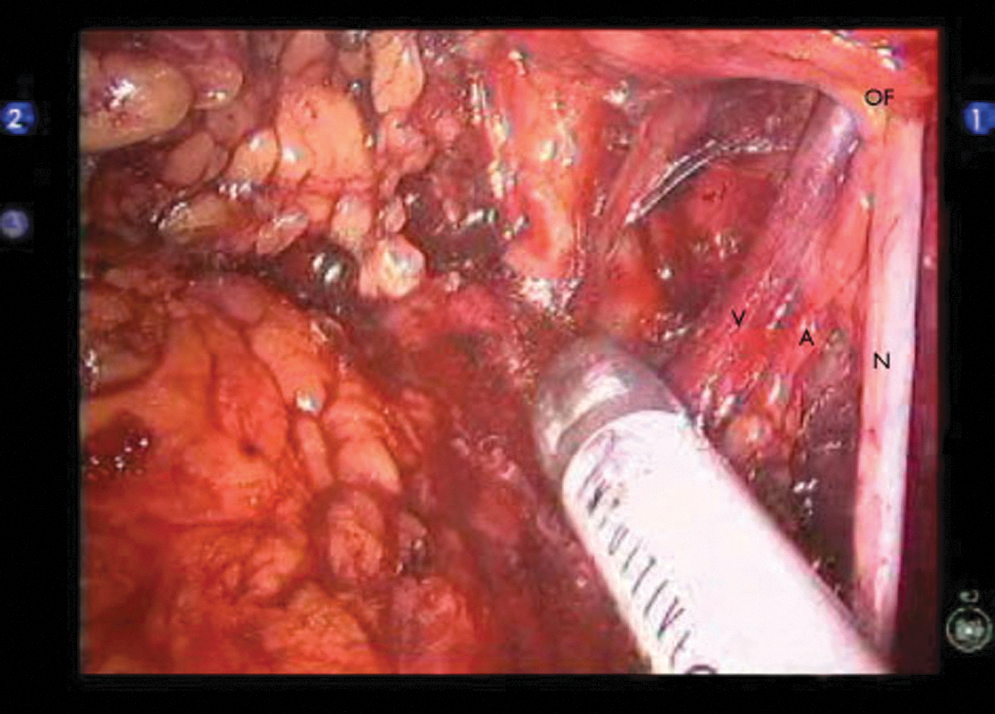
Obturator vessels (V and A), traveling medial to the obturator nerve (N), entering the obturator foramen (OF).
Node of Cloquet dissection
Distally, the dissection is limited by the circumflex iliac vessels. The distal limit of the lymphatic packet is the node of Cloquet. This packet is located between the external iliac vein anteriorly and the pubic bone posteriorly. A Hem-o-lock clip may be placed here to ligate the distal lymphatic tributaries. The entire lymphatic packet is now completely freed. The left and right lymphatic packets are placed in separate Endocatch bags (Covidien, Mansfield, MA) and retrieved after the da Vinci patient cart is undocked.
Postoperative care
The orogastric tube is removed before emergence from anesthesia. The patient is allowed clear liquid immediately after surgery and progressed to a regular diet on the first postoperative day. Ambulation is encouraged on the first postoperative day aided by adequate analgesia. Prophylactic low molecular weight heparin is administered until the patient is discharged from the hospital.
Management of intraoperative complications
Injuries to the structures within the template are the main concern during pelvic lymphadenectomy. Injury to the iliac veins may be controlled by increasing pneumoperitoneum pressure to 20 mm Hg and direct tamponade. Arterial injuries will not be arrested by increasing intraperitoneal pressure. Hemostatic agents such as Floseal (Baxter, Deerfield, IL) and Surgicel (Johnson & Johnson, New Brunswick, NJ) may be used in adjunct. These measures will usually stop small vascular injuries. Bipolar coagulation should not be applied directly onto the vein. Injuries that do not respond to the above measures should be repaired with robot-assisted suturing or, rarely, open surgical repair.
Ureteral injuries may be encountered at the proximal limit of dissection. When detected during surgery, immediate repair should be performed with spatulated end-to-end anastomosis. If the distal segment is too short, the proximal end should be reimplanted to the bladder after adequate mobilization. A ureteral stent should traverse either the ureterouretero- or ureterovesical anastomosis.
Management of postoperative complications
There are only a few series of robot-assisted or laparoscopic lympadenectomy in the literature that reported complications specific only to the lymphadenectomy. Most series reported complications in conjunction with prostatectomy performed in the same sitting. In laparoscopic series, overall complication rate in these series ranged from 14.3% to 35.9%. 16,17 In robotic series, complications ranged from 5% to 23%. 18,19 Serious complications that can be attributed to lymphadenectomy include lymphoceles, deep vein thrombosis, and pulmonary embolism.
While the intraperitoneal approach during robot-assisted lymphadenectomy may decrease the rate of symptomatic lymphoceles occurring, one study showed that CT-detected lymphocele developed in 51% of patients, of which 15.4% were clinically symptomatic. 20 Without an intraperitoneal drain, patients present with sensations of pelvic pressure, abdominal distension, lower limb weakness, or febrile illness. In the presence of persistent symptoms, lymphoceles can be effectively treated with percutaneous drainage.
In our series of 65 robotic-assisted pelvic lymphadenectomies performed in the last 18 months, there have been no ureteral injuries and no vascular injuries. While cross-sectional imaging was not routinely performed in these patients postoperatively, we had noted asymptomatic lymphoceles relatively commonly in some patients. On several occasions, we had seen delayed infections in lymphoceles, which were definitively managed with temporary percutaneous drainage.
Results
The outcomes of pelvic lymphadenectomy after RALP can be evaluated in terms of frequency of nodal metastasis and yield. Some of these are summarized in Table 1, including our own results. The template used in our technique includes the nodes in the external iliac, internal iliac, obturator, and the common iliac groups up to the crossing of the ureter. This template is commonly called the extended template, as opposed to the limited template, which includes only the obturator group. 3 Many studies had repeatedly shown the superior detection rate of micrometastases using the extended template compared with the limited template. 7,17,21
Included in our template is the perirectal lymph node basin, which is not commonly discussed in surgical texts. On the contrary, the perirectal group had long been identified as a common area of “geographic miss” in radiation oncology literature. 22 In a sentinel node single photo emission CT (SPECT) imaging study for 25 high-risk prostate cancer patients, the top four commonest groups of sentinel nodes were external iliac (35.0%), internal iliac (18.3%), common iliac (11.3%), and perirectal (8.4%). 23 In a very similar study involving a lower risk cancer group, SPECT imaging identified primary lymphatic landing sites in the perirectal/presacral region in 8% of patients. 24
Leaving recurrence in the perirectal region has adverse clinical implications during salvage radiotherapy by putting patients at risk of rectal toxicity. Even with prostate bed-only intensity-modulated radiation therapy (IMRT) compared with whole pelvis IMRT, there was no difference in late gastrointestinal toxicities in a recent comparative study. 25 These studies clearly demonstrated the importance of clearing out the perirectal group during primary lymphadenectomy after prostatectomy.
Conclusion
With the ever increasing number of RALP being performed for localized prostate cancer, robot-assisted lymphadenectomy offers an effective minimally invasive technique for the pathologic staging of regional disease. To minimize unnecessary morbidity, only those patients at risk of occult lymph node metastasis should be selected. Identifying the important surgical pelvic landmarks and using an extended template are keys to maximize lymph node yields while reducing complications.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.