
Abstract
Purpose:
We report our experience with laparoscopic heminephrectomy (LH) in children with duplex kidneys, emphasizing complications and late outcomes, and including anatomic and functional aspects.
Patients and Methods:
We retrospectively reviewed medical data of 28 children with a duplex kidney who underwent LH. Complications were evaluated according to the Savata and Clavien classiffication systems.
Results:
Nineteen upper (67.8%) and 9 (32.1%) lower moieties were removed. All laparoscopic procedures were completed as planned without conversion. There were three (10.5%) cases of intraoperative bleeding successfully controlled by compression with gauze. Complications after surgery included two urinomas (7%), one intra-abdominal hematoma (3.5%), and two cases of complete functional loss (7%) because of torsion of the remnant upper pole. In six (21.4%) cases, a cyst at the resection margin of the kidney remnant was found. The function of the remnant pole was preserved in 23 (82.1%) cases and decreased in approximately 5% in 3 (10.5%).
Conclusions:
The anatomic and functional outcomes of LH must be evaluated with imaging studies and nuclear scintigraphy to rule out structural abnormalities and functional impairment. An extensive dissection in the lower pole LH can lead to the upper moiety torsion after surgery.
Introduction
Although LH is currently more popular than the open procedure, some authors criticize increased operative times and costs of LH. 5 Multiple reports describe the advantages of LH compared with the open approach, but very few indicate complications of this laparoscopic technique and show its late outcomes. 4,6 –8
We do not intend to assess which technique is safer or which should be the technique of choice for heminephrectomy. We report our experience with LH in children with duplex kidneys emphasizing the incidence of particular complications, their management, and late outcomes, including anatomic and functional aspects.
Patients and Methods
We retrospectively collected the demographic, operative, and follow-up data for 28 children (age 3–70 mos, mean 18 mos) with duplex kidney, who had undergone LH between 2003 and 2011 at our center. All patients were studied using ultrasonography (US) and isotopic studies, as well as voiding cystourethrography in case of associated vesicoureteral reflux (VUR). In three (11.5%) patients, MRI was performed to confirm systemic duplication. Renal function was assessed using technetium-99m dimercaptosuccinic acid (99mTc- DMSA) in 9 (30.7%) and technetium-99m mercaptoacetyltriglycine (99mTc–MAG3) in 19 (69.3%) patients with suspected urinary tract obstruction. A differential function of the affected pole of less than 5% on the isotopic studies was considered an indication for surgery. All procedures were performed using a transperitoneal approach, and the results were evaluated at 6 months after surgery with US and a radioisotope scan (99mTc- DMSA).
Intraoperative complications were grouped according to the Savata classification system (grade I, incidents without consequences; grade II, incidents repaired intraoperatively; grade III, incidents requiring reoperation) 9 (Table 1), and postoperative complications were grouped based on the modified Clavien system (grade I, minor complications, such as transitional subcutaneous emphysema, hematuria, and neuropathy, which disappear spontaneously; grade II, bleeding requiring blood transfusion, temporary ileus, prolonged urinary leak, port site infection or hematoma, fever, urinary tract infection, pneumonia, or thrombophlebitis; grade III, complications requiring reoperation; grade IV, severe complications, such as pulmonary embolism, myocardial infarction, or congestive heart failure; and grade V, death of the patient) 10 (Table 2).
Surgical technique
The operation is performed under general anesthesia with the patient's pathology side elevated to an angle of 45° from the supine position. We use nasogastric and bladder tubes to decompress the stomach and bladder, respectively. Three ports are used when operating on the left kidney and four in the case of the right one. An infraumbilical incision is made and a 5-mm port placed into the peritoneal cavity under direct vision. A 5-mm 30-degree telescope is used to visualize the operative field. Two additional 5-mm ports are placed, also under direct vision, one subcostally and the other lower, at the iliac fossa. On the right side, an additional 3-mm trocar is placed in the epigastric area to retract the liver. The colon is reflected to expose the kidney, and both ureters are identified and mobilized as high as possible to avoid injury to the unaffected ureter. To remove the ureter, it needs to be dissected up to the the level of the pedicle. It is then dissected further distally and transected. The vessels to the affected moiety are divided using clips or Ligasure® (vessel sealing, Covidien), and the parenchyma is incised using a harmonic knife, monopolar diathermy, Ligasure, or laser.
For the upper pole LH, the previously dissected ureter is retracted to a suprahilar position to expose the upper pole vessels and parenchyma. The upper pole vessels are then divided and the parenchyma incised (Fig. 1). The ureter of the affected pole is transected all the way down beyond the pelvic brim and left open in the case of ectopic ureter or ureterocele, and tied in the case of reflux. The specimen is removed through the umbilical port.
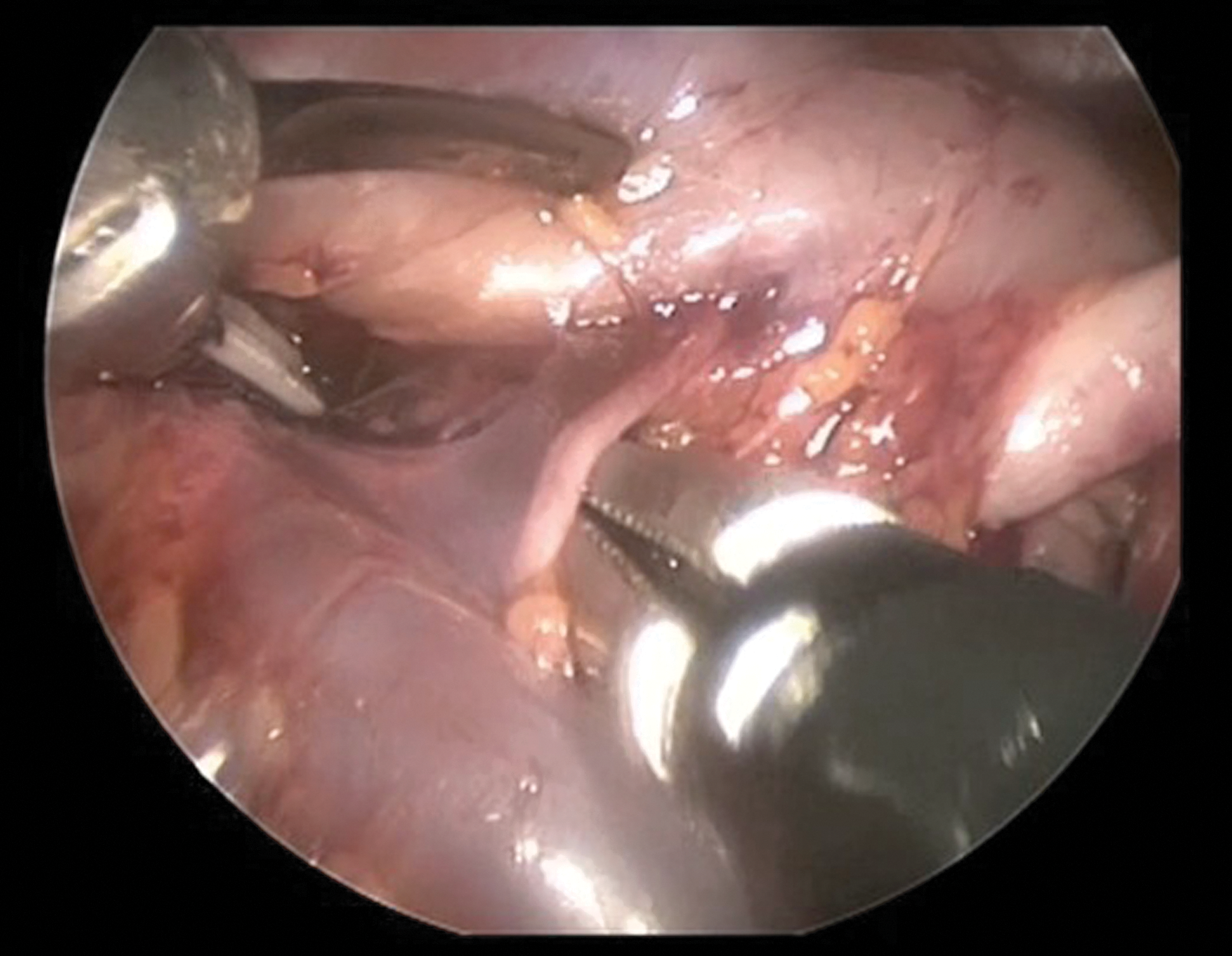
Upper pole vessel dissection.
Results
A total of 14 males and 14 females were included in the study. The median age at surgery was 18 months (age range between 3 months and 5 years). 19 upper pole moieties (67.8%) and 9 lower (32.1%) were removed. There were 16 right side (57.1%) and 12 left side (42.9%) LH performed. The cause of LH was: ureterocele in 8 cases (28.5%), ectopic ureter in 11 cases (39.2%), and vesicoureteral reflux in 9 cases (32.3%; 4 cases grade III, and 4 grade IV). Mean surgical time was 137 min (range: 90–200 min).
Intraoperative incidents/complications
Intraoperative complications were noted in six (21%) patients (Table 3). Satava grade I incidents were observed in two (7%) patients by discharge of pus into the abdominal cavity alter the puncture of the upper moiety ureter. Satava grade II complications occurred in four (14%) patients: Three cases of intraoperative bleeding (10.5%) that was successfully controlled by compression with gauze, and one (3.5%) case of opening calices of the lower pole moiety that was fixed by intraoperative laparoscopic suturing and monitored by leaving a drain in the surgical bed. The blood loss was minimal in these cases. There were no Satava grade III incidents. There were no conversions to open surgery in our group of patients.
Postoperative complications
Postoperative complications ocurred in 14 (50%) children. Six (21.4%) patients had Clavien grade I complications: The presence of cysts at the resection margin of the renal remnant. There were three children with Clavien grade II complications (10.5%): An intra-abdominal hematoma (managed conservatively) and two cases of discharge of pus into the abdominal cavity. These three patients needed a 7-day postoperative antibiotic course. Clavien grade III complications occurred in five (17.5%) children: Two (7%) urinomas, two (7%) cases of complete functional loss (caused by rotation of the upper pole remnant after the lower pole removal), and an omentum evisceration through the wound during drain removal (3.5%). The urinomas were managed with a Double-J stent and drainage months after the surgery.
The mean postoperative hospital stay was 2.2 days in the patients without complications. The hospital stay in the patients with incidents was: 2 days for the two cases of bleeding and the case of omentum evisceration, 4 days for the patient with the opening calices, and 8 days for the two patients who remained in the hospital with antibiotic treatment (two cases of discharge of pus into the abdominal cavity).
The function of the remnant pole was preserved in 23 (82.1%) cases and decreased in approximately 5% in 3 (10.5%). The mean follow-up is 3 years and 2 months (range 7 mos to 6 yrs).
Discussion
Duplex kidney is a common congenital abnormality with a potential for significant morbidity. This pathology may be associated with ureterocele, ectopic ureter insertion, or VUR. Partial nephrectomy is an established treatment for the nonfunctional moieties. 11 The techniques and results of open heminephrectomy are well known, 12,13 but a growing amount of evidence supports the preference of the laparoscopic approach to this procedure. 5 Since Jordan and Winslow 3 published their first experience of LH in 1993, several authors have validated the safety and efficacy of this approach. 14 –17 Because LH is a more complex procedure than a nephrectomy, laparoscopy has been introduced only gradually for this procedure. Advantages of this technique include magnification, excellent visualization of the parenchyma and the distal portion of the ureter, minimal blood loss, fast recovery, and less surgical scarring. 4,6,7,14,18
Several series confirm these advantages and the feasibility of performing heminephroureterectomy in infants and children using laparoscopic techniques. 4,7,8,16,18,19 Nevertheless, other authors show that LH is not always superior to open surgery in terms of safety, cost, and operative time, and related technical difficulties of LH in young children, especially when upper pole partial nephrectomy is performed. 5,7,16 Another controversy is about the kind of laparoscopic approach. Some authors advocate that the transperitoneal approach provides a more comfortable working space in small infants, allows more complete ureterectomy, and appears to have a lower conversion rate compared with the retroperitoneal approach. 20,21 On the other hand, several series concluded that there are no major technical advantages of one approach over the other. 21,22 LH is technically more demanding than a total nephrectomy and carries a risk of complications such as hematoma from hemorrhage, urinoma because of urinary fistula, and ischemia of the remnant pole from renal pedicle injury. 3,17
In our series, we attempted to standardize complications and determine the risk factors for particular complications. Therefore, complications have been categorized according to two classification systems and evaluated accordingly. To avoid or at least minimize incidents, it is important to understand the error itself and the factors leading to it, as well as the type of error that has been committed. 23
The use of classification systems to report the complications should be useful to compare different series. The Satava (intraoperative incidents/complications) and the Clavien (postoperative incidents/complications) classification systems are two standardized systems that can be used for evaluation of commplications. 9,10 These systems collect meticulously all surgical complications, including even minor incidents, such as a minimal bleeding described in our series or the appareance of cysts at the resection margin. These incidents were not even considered complications in other series of open and laparoscopic procederes. 24 For example, Jayram and associates 11 report that a postoperative urinoma developed in seven patients and one patient had a hematoma. After these comments, they explain that no other major complications were observed, but describe the development of an asymptomatic renal cyst in 38 patients and a persistent ureteral stump dilatation in 7 patients. You and colleagues 6 found only two complications after surgery (a patient who had a prolonged urine leak and a complete loss of function of the remnant pole), but after this comment, they also mention that the follow-up US showed asymptomatic cystic structures in six patients and one remnant ureteral stump that were not included as complications. Therefore, we think that the complication rate varies according to what the author considers a complication, and we think that without standardized systems for evaluation of complications, various series are not comparable.
Intraoperative complications were found in six patients and included in the Satava classification system. All these complications were managed by endosurgical methods. The Satava grade I complications are incidents without consequence and rarely are reported in the published series. These complications may go unrecognized or be recognized, but may not be significant enough to result in a complication. In our series, in two cases, a discharge of pus into the abdominal cavity occurred when the upper moiety ureter had been punctured. The Satava grade II incidents are errors with instant detection and correction, which results in the possibility of recovering from the error with minimal or no consequence for the patient. An example here may be our three cases of bleeding, which were identified and controlled by compression with gauze, or the case of opening the calices of the lower moiety also recognized and fixed by intraoperative laparoscopic suturing and leaving a drain in the surgical bed. The above measures prevent a hematoma or urinoma formation in the postoperative course. Immediate identification of error permits full recovery of the patients. Only in the case of Satava grade III complications can the surgeon be clearly blamed, because it is not only a committed error but also lack of its recognition that makes recovery from it impossible. An example would be a bowel perforation without recognizing it until the postoperative period or a section of the unaffected ureter that entails the conversion to open surgery to repair it.
We routinely closed all port sites except the one through which the drain was placed. In our series, we observed one omentum evisceration through the wound during drain removal, but this could be easily treated at the bedside.
The urinoma occurred in two (7%) patients with a nonfunctioning lower pole who had a high-grade VUR. These patients needed a Double-J stent placement and a percutaneous drain placement.
In our study, undilated, unrefluxing ureters were divided at the proximal level and left open. In severely dilated, unrefluxing ureters, a longitudinal incision was made opening the distal stump of the ureter, and a drain tip was placed in the lumen of the distal ureter for effective drainage. If VUR had been diagnosed before surgery, we performed a distal ureterectomy and sutured the vesical hiatus. There were no complications associated with the remnant ureteral stump in our group of patients. An appropriate level for ureteral resection has not been yet agreed. In the series from Dénes and coworkers, 25 they report that ureteral stump empyema occurred later after surgery in 16% of patients and needed surgical treatment. On the other hand, Mushtaq and Haleblian 18 reported the presence of a remnant ureteral stump on US in 13% of cases, and none of the patients was symptomatic during follow-up. Also the risk of injury to the healthy ureter might outweigh the benefits of a complete ureterectomy. 26
Although many authors do not treat the cysts at the resection margin as a complication, we have classified them as Clavien grade I complications, because these cysts do not cause any deviation from the normal postoperative course and there is no need for additional pharmacologic treatment or surgical, endoscopic, and radiologic interventions. We have found six cases of cysts at the resection margin of the renal remnant. The presence of a cyst structure on US is probably because of urine production from an incompletely removed urothelium, or urine leak from opening of the remnant collecting system. 6 These cysts have been reported in several laparoscopic series and were always asymptomatic. 6,11,18,25 We have found cysts in 21.4% of our patients, which is a similar number to the rate of 31% published by Mushtaq and Haleblian 18 or of 27% by Jayram and colleagues. 11 Although cyst formation is also seen after open heminephrectomies, the precise incidence has not been reported. 24
We have evaluated changes in function using DMSA before and after surgery. Although most of the remnant poles preserved their function (81.1%), and in three (10.5%) cases decreased only approximately 5%, a complete loss of function was seen in two (7%) patients. You and coworkers 6 reported one case of functional loss of the remnant pole (6%), and Dénes and associates 25 another one (5.3%). Several reports showed that severe functional impairment might be unrecognized. 3,25 You and colleagues 6 recommend nuclear scintigraphy after surgery in all patients. Jayram and coworkers 11 suggested routine US examination in the early postoperative period (around 3 months) to assess the anatomy of the remaining moiety, and in the case of a normal result, this should be repeated at 12 months. Alternatively, routine DMSA scanning postoperatively may be considered if there is concern of renal deterioration because of intraoperative technical difficulty or complicated anatomy. 11 The US is useful to rule out structural abnormalities.
Usually the upper pole injury during lower pole heminephrectomy may be from vascular injury during the surgery (when the renal hilum is dissected) or vasospasm after the procedure (for excessive traction of the lower pole). In our cases, the cause of loss of function was a twist of the remnant pole. In these cases, the US performed at 3 months after surgery showed hydronephrosis that did not exist on the US before surgery as well as cortical thinning. The DMSA confirmed the complete loss of function. In these cases, 1 year after the first surgery, we performed a remnant upper pole nephrectomy finding a twist of approximately 90 degrees that, we think, caused the upper pole hydronephrosis and the loss of funcion of the remnant pole. We hypothesize that an excessive upper pole moiety dissection could be the cause of such a complication because of exposure of the renal hilum. Although we have not found any similar complication in other LH series, perhaps less dissection is sufficient to avoid this complication without having to fix the upper pole moiety with stitches.
Most complications can be anticipated and therefore avoided. General principles of surgery may be applied to laparoscopic surgery: Check anatomy, provide adequate exposure, use a wide dissection rather than a deep one, and provide good visualization. If any of these goals cannot be accomplished, the likelihood of complications is greater. We think that conversion to open surgery is not a complication but in certain situations can prevent complications or incidents during laparoscopic surgery.
Conclusions
Prevention of complications may be possible, and the use of standardized systems for evaluation of complications should be used to help compare different series of patients.
The anatomic and functional outcomes must be evaluated after LH with an imaging study such as US to rule out structural abnormalities (for example, urinomas or hydronephrosis), and nuclear scintigraphy is necessary to visualize the function of the remnant pole, because the functional impairment from vasospasm or vascular injury might not be recognized during the procedure and can manifest months later as a loss of function.
An extensive dissection in the lower pole LH can lead to upper moiety torsion after the surgery.
Footnotes
Disclosure Statement
No competing financial interests exist.