
Abstract
Purpose:
We designed a three-phase bedside assistant training course for those involved with robot-assisted radical prostatectomy (RARP). We also examined whether an experienced RARP team (>1000 cases) would perceive benefit from this three-phase bedside assistant training course.
Materials and Methods:
The 13 RARP bedside assistants were identified at our institution (three surgical technicians, two surgical assistants, four resident trainees, and four physician assistants). The course consisted of three phases that were taught at three separate morning sessions. Phase 1 focused on robot functionality. Phase 2 consisted of a step-by-step video session that focused on the assistant's role in each RARP step. Phase 3 involved three hands-on laparoscopic drills that were to be completed in a predetermined period. Pre- and postcourse questionnaires assessed learner knowledge pertaining to RARP.
Results:
All 13 learners completed the three-phase training course. Nine of 13 learners thought this course would be beneficial, although, 9 of 13 already thought that they were good RARP assistants before the course. Ten of 13 learners were able to complete the hands-on drills in the predetermined periods. On completion of the course, every learner thought the course was beneficial and that it should be repeated annually. Twelve of 13 thought that the course made them a better assistant and that their intra-abdominal spatial orientation was greatly improved. Seven of the learners thought the hands-on drills were the most beneficial portion of the course, while the other six found the step-by-step lecture the most beneficial.
Conclusions:
A three-phase hands-on RARP bedside assistant training course is beneficial to and desired by an experienced RARP team at least annually.
Introduction
We aimed to design a three-phase bedside assistant training program for assistants involved in RARP. We also desired to examine if our experienced robotic team (>1000 cases) would benefit from the simulation-based training.
Materials and Methods
Surgical leadership at our institution decided to limit the amount of assistants present for RARP. After consulting with the Mayo Clinic Institutional Review Board, they concluded that the questionnaire used in the study did not require approval. It was determined that the bedside assistants would be limited to urology residents (4), urology physician assistants (4), surgical technicians (3), or formally licensed surgical assistants (2). The bedside assistants were all experienced with RARP. More than 1000 RARP have been performed at our institution since 2006. The team also had extensive experience with other robot-assisted urologic surgeries (partial nephrectomy, pyeloplasty, and cystectomy) and robot-assisted gynecologic surgery. It was determined that the assistants would undergo formal assistant training pertaining to RARP, which would involve a hands-on component in our multidisciplinary simulation center.
A questionnaire was sent to all members of the team to ascertain their presumed weaknesses and areas in which they thought there could be improvement in their performance. The course was tailored to the answers received. The course was set up in three phases to be taught on three separate morning sessions.
Phase 1 of the course (90 minutes) involved hands-on robotic training and focused on robot functionality. Proper docking techniques, robot movement, console functionality, camera loading, Tile Pro, and other topics were reviewed. A representative from Intuitive Corporation (Sunnyvale, CA) was responsible for teaching the content of this course in the operating room.
Phase 2 of the course (60 minutes) involved a video review with one RARP surgeon. The video was spliced into segments from cases performed at our institution. The video included basic anatomy of the prostate, neurovascular bundles, and urethral sphincter. The video focused on 10 separate portions of the operation and the role of the assistant in each portion. The 10 segments of the video were: Positioning, port placement, bladder takedown, endopelvic fascia dissection/dorsal vein ligation, bladder neck dissection, seminal vesicle/vas deferens dissection, rectum dissection, nerve sparing, anastomosis, and exiting the abdomen.
All RARP at our institution are performed with the same port placement (Fig. 1). All are performed with a da Vinci Si surgical system using the fourth arm (placed on the patient's left side). The surgical assistant stands on the right side of the patient using a 12-mm port that is located 7 cm superior-lateral to the right side 8-mm robotic port. The assistant also uses a 5-mm assistant port placed 7 cm superior-lateral to the midline 12-mm camera port on the patient's right side. One focus of the video is to have the assistant focus the left hand on the 5-mm port that is occupied by the suction-irrigator throughout the case. The 12-mm port is accessed by the assistant's right hand and is used for any grasper, suture entry, specimen bag, etc.
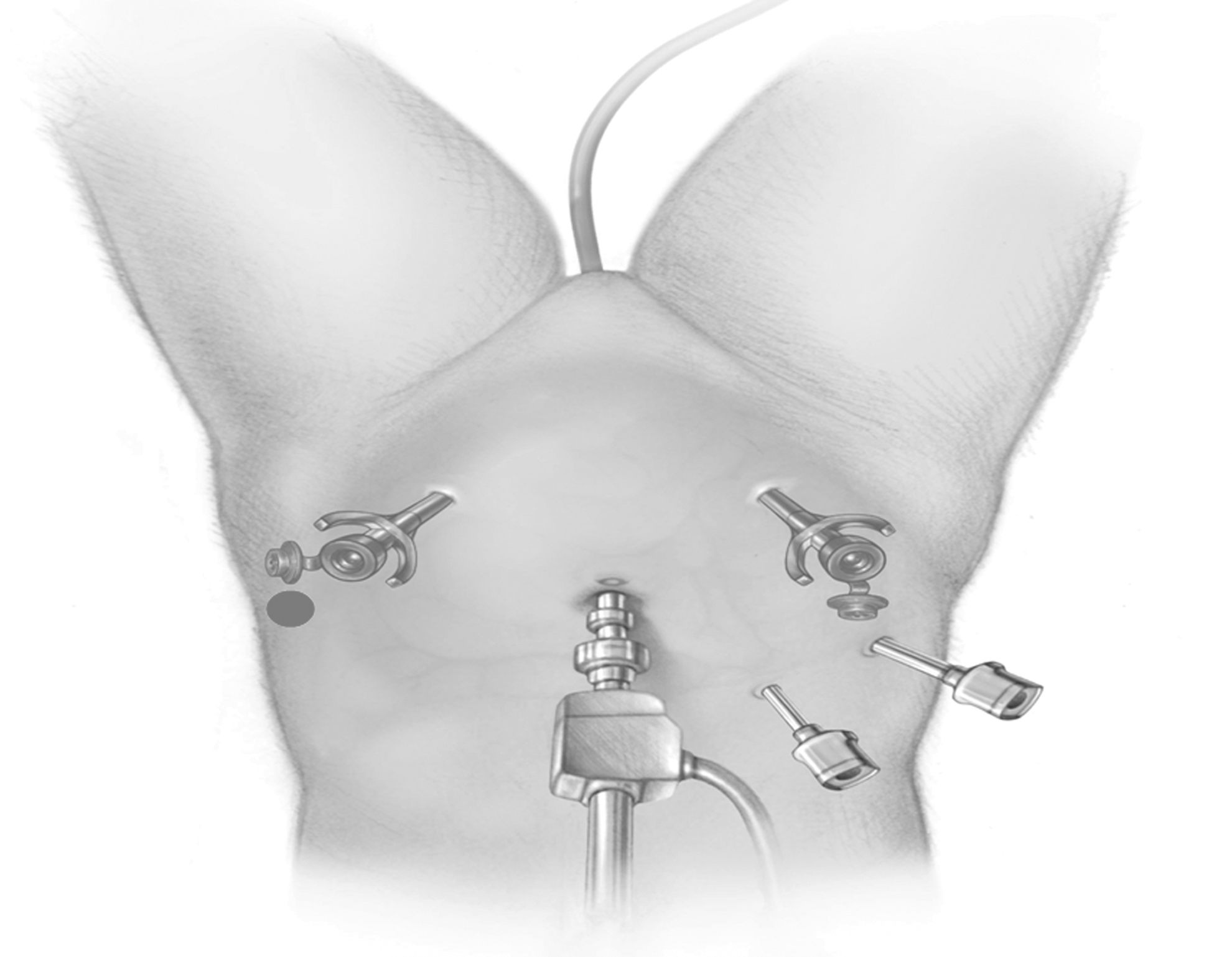
Robotic port placement. Standard robotic port placement consists of a supraumbilical midline 12-mm camera port with 8-mm robotic ports to be placed 2 cm inferior to the umbilicus and 10 cm lateral to the midline. The right side assistant 12-mm assistant port is placed 7 cm superior-lateral to the right side 8-mm robotic port. The 5-mm assistant port (sucker port) is placed 7 cm superior-lateral to the 12-mm midline camera port. If a fourth arm is used, it is placed on the patient's left side 10 cm lateral to the left 8-mm robotic port. Reprinted from: Thiel DD et al. Urology 2011:77:1238–1242, with permission from Elsevier.
Phase 3 of the course was a hands-on component in the multidisciplinary simulation center. The drills were designed with specific aspects of RARP in mind using a Fundamentals of Laparoscopic Surgery (FLS™) training box, two trocars in a fixed position, a fixed position camera, and standard laparoscopic instruments. The learner had to stand on the right-hand side of the laparoscopic training box (Fig. 2). The monitor was set up across the box, and the drills were designed to be performed in the base of the box on the right side to mimic the deep pelvis. The first drill (Fig. 3A) focused on the learner using the right hand to place the three objects in the target. The left hand had to remain in view of the camera at all times. The goal of this drill was for the learner to achieve spatial orientation and depth perception in a monocular viewing system.

Assistant setup for hands-on drills. The learners were placed on the right hand side of the laparoscopic training box and faced a monitor directly across from them while performing drills to their direct right to mimic the ergonomically challenging environment of assisting in the deep pelvis.
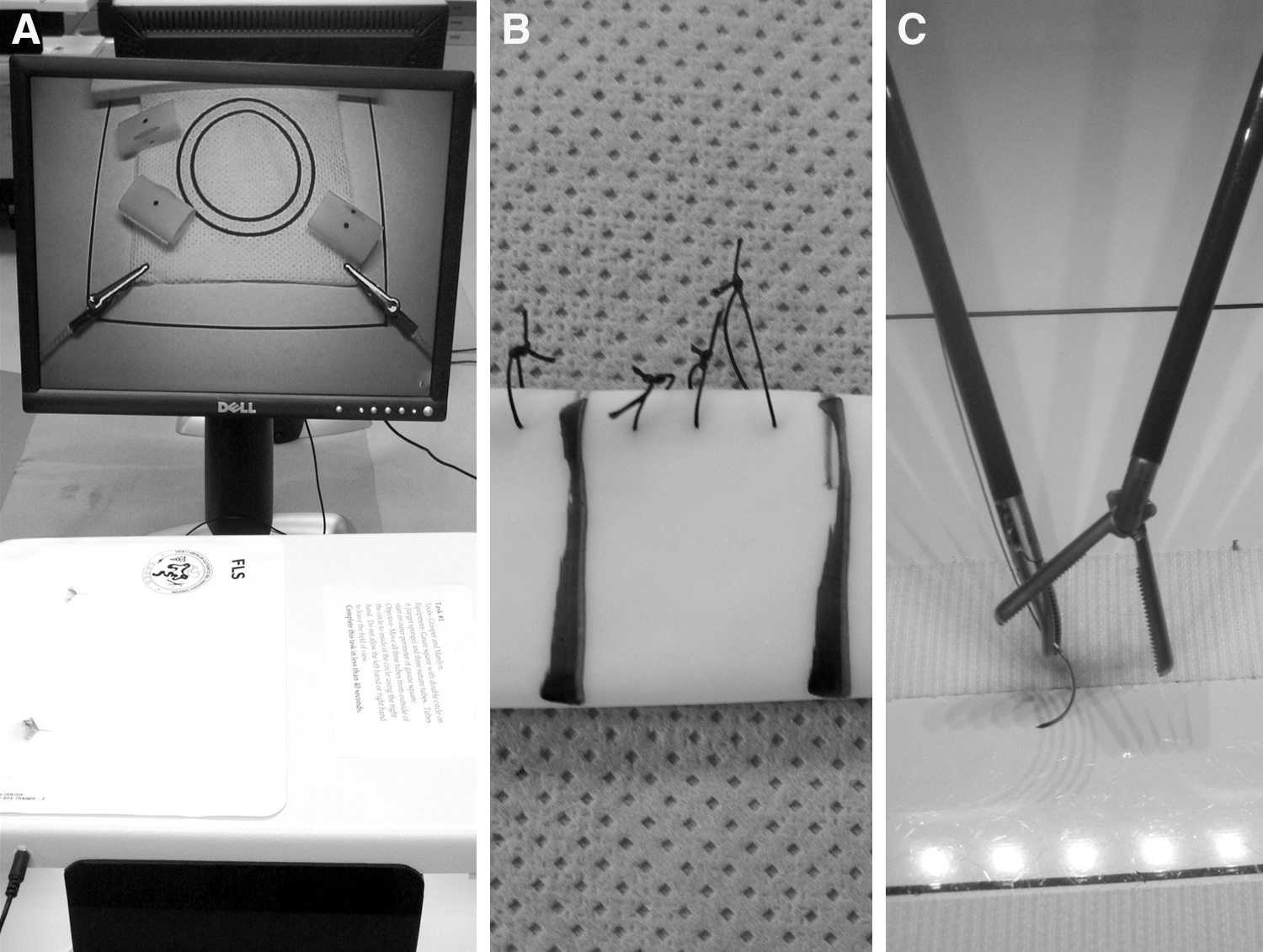
Hands-on drills performed.
The second drill (Fig. 3B) focused on the learner using the right hand to cut suture, holding the suture in place with the left hand while switching the scissors to a grasper and then removing the suture from the box with the right hand. The goal of this drill was to get the learner to focus on placing scissors in the right side assistant 12-mm port and then removing the suture through the same 12-mm port. The third drill (Fig. 3C) focused on spatial orientation and dexterity. A suture and needle were introduced into the box with the right hand and crossed to the left hand inside the box and then removed with the left hand from the box. This drill focused on the coordinated use of both the dominant and nondominant hand. This was repeated three times.
All learners were brought into the simulation center and were shown the drills to be performed. The learners were allowed to practice the drills and then were asked to come back individually to perform the drills under set times. There was no time limit for the drills. The set times were established by having a surgical technician perform all three drills and then taking the average of the technician's three times as the set time. Drill 1 was to be performed within 40 seconds. Drill 2 was to be performed with 100 seconds. Drill 3 was to be performed within 45 seconds. These times were the average of three laparoscopic-naïve simulation center employees performing these tasks after a period of practice.
Two weeks after course completion, a postcourse questionnaire was completed. The questionnaire assessed overall learner satisfaction with the course as well as potential areas for improvement. The questionnaire was designed to assess answers to key questions. The questionnaire also assessed the learner's desire to have the course repeated annually and the desire to have a course for other similar types of surgeries in robotics or other disciplines.
Results
A precourse questionnaire demonstrated that no one had taken a formal hands-on or video-based laparoscopic training course in the past (Fig. 4). Nine of 13 thought this type of course would be beneficial to them, even though 9/13 considered themselves “good” assistants before the course. Two areas of emphasis for the course were to make sure the assistants understood that their biggest risk to the patient was inadvertent bowel or vascular injury and to emphasize to the assistants that needles and objects should be entered and removed from the body via the 12-mm assistant port site. As Figure 4 demonstrates, a majority of the learners demonstrated understanding of those concepts in the preprocedure questionnaire.
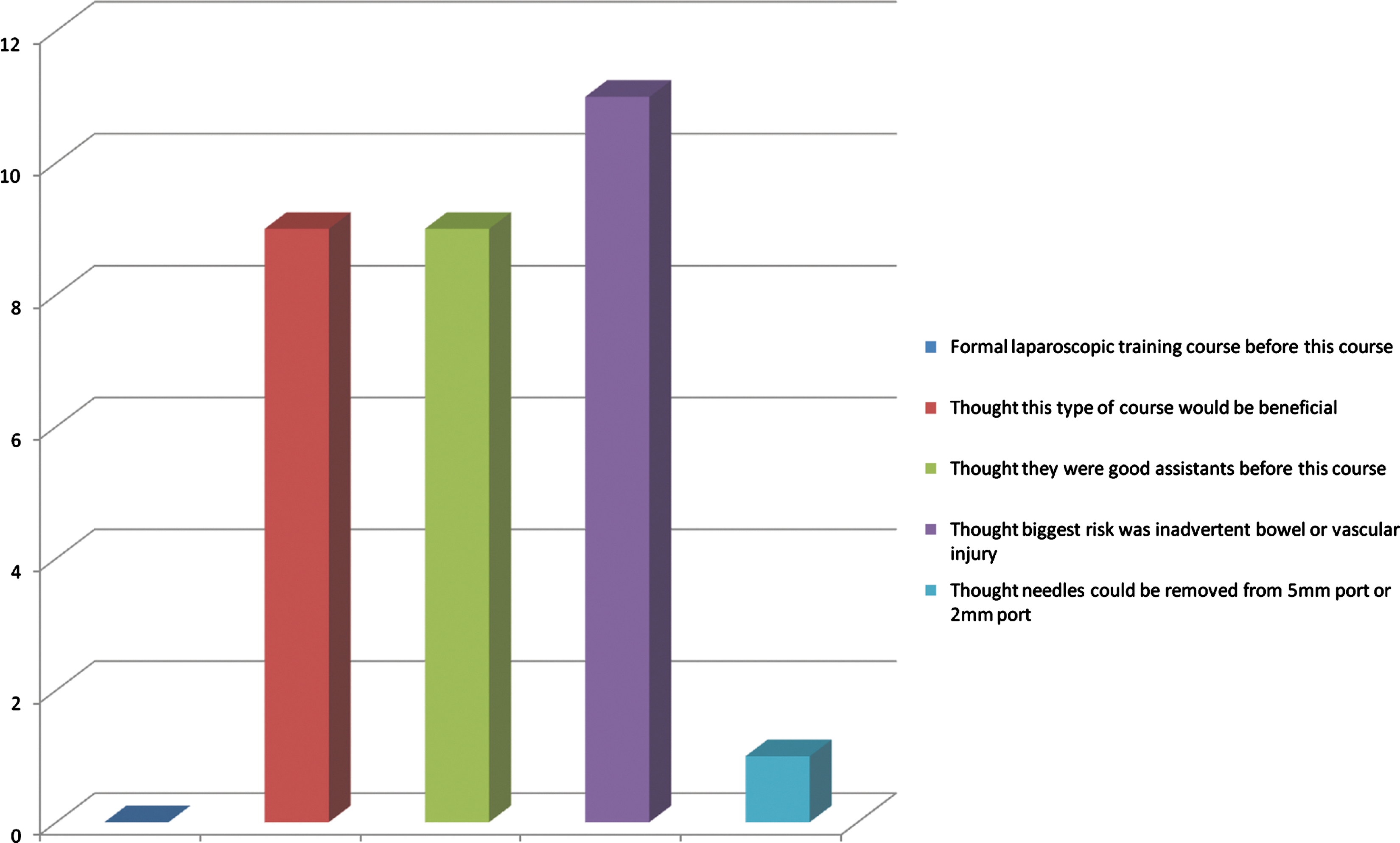
Pre-Course Questionnaire Responses.
All 13 members of the RARP team completed the three-phase course. One assistant had been involved in bedside assisting in more than 100 cases. Four of the learners had been a bedside assistant for fewer than 50 cases. The rest of the group had assisted in 50 to 100 cases. When asked what the assistant's biggest fear was, the four most common responses were: “Upsetting surgeon,” “puncturing bowel,” “nicking blood vessel,” and “troubleshooting the robot at the bedside.”
All 13 members of the RARP team completed the hands-on tasks in the presence of a neutral simulation representative on two separate occasions. All 13 learners completed the first drill (object placement) in the required 40-second period by their second attempt (range 10–33 seconds). Ten of the 13 were able to complete the second drill (suture cut and removal) in the required 100-second time frame by their second attempt (range 56–172 seconds). One physician assistant, one resident, and one surgical technician were unable to complete the task in the required time frame. Ten of the 13 learners were able to complete the third drill (needle passing with right and left hand) in the required 45-second time frame (range 21–63 seconds). None of the learners who failed to meet the time requirements were those who considered themselves “good assistants.”
The postcourse questionnaire results are demonstrated in Figure 5. Every learner thought that the course was beneficial and that it should be repeated annually. Twelve of 13 thought that the course made them a better assistant and that their ability to find themselves intra-abdominally was greatly improved. Only 10/13 thought that the course helped to alleviate their biggest fear of being a robotic assistant. Interestingly, 11/13 learners thought that this type of course would be beneficial for procedures other than RARP. Seven of the learners thought the hands-on drills were the most beneficial portion of the course while the other six thought the step-by-step lecture was the most beneficial portion of the course. Only one person (physician assistant) thought the hands-on portion was the least beneficial portion of the course. A majority (n=7) thought the Intuitive representative demonstration was the least beneficial portion of the course.
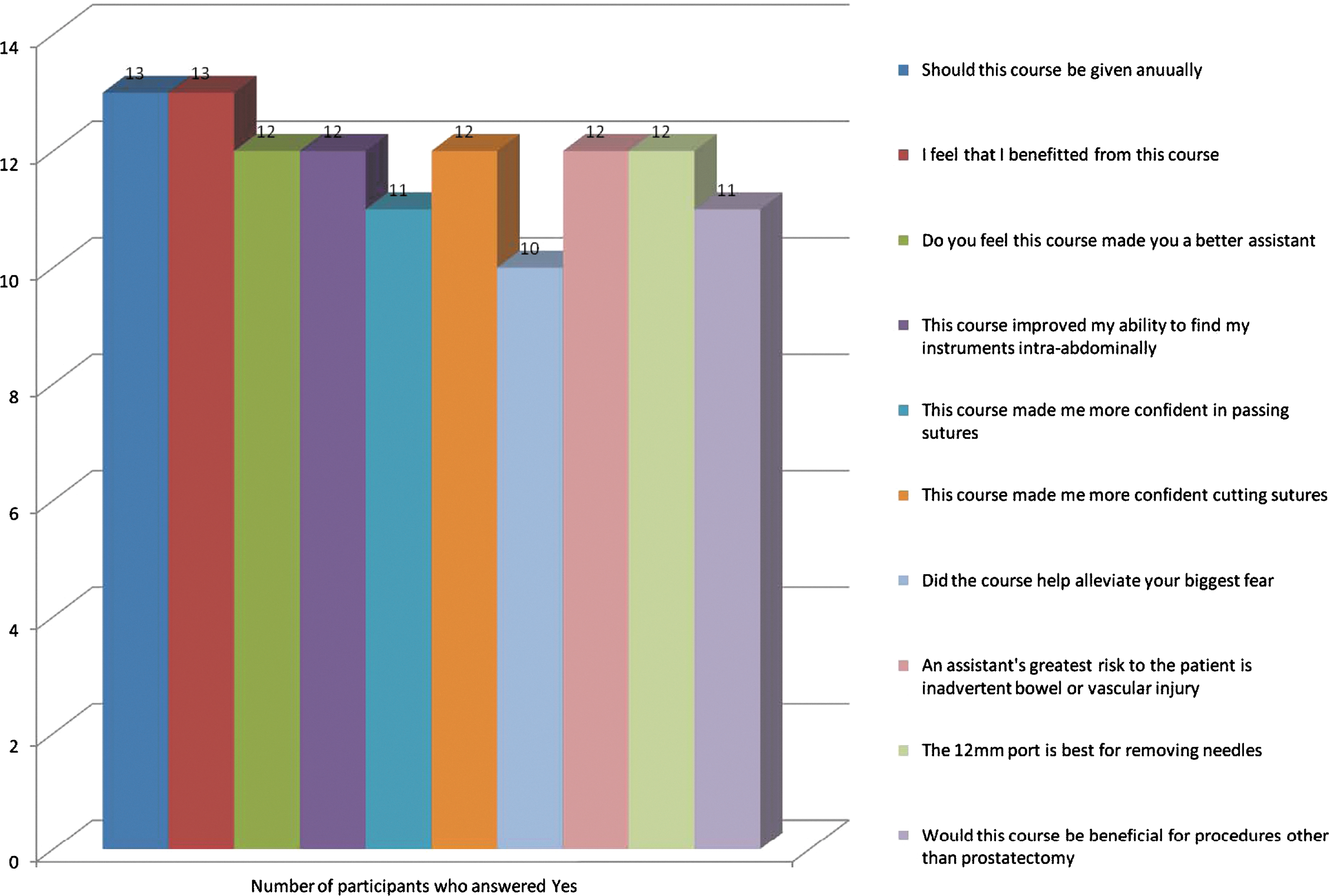
Post Course Questionnaire Responses.
Discussion
Although the bedside assistant is not actually performing surgery during RARP, the role is crucial to successful performance of the procedure. The assistant significantly affects the safety and efficiency of the operation, and this is especially true in the presence of experienced robotic prostatectomists. Cumulative mistakes by the assistant can cause significant patient morbidity, delay in surgical progression, and lead to open conversion. 4 Poor training of the bedside assistant can lead to such surgical situations as lost surgical needles and major vascular injury. 5,6
Robotic surgery provides a unique challenge with regard to the bedside assistant secondary to the physical distance from the surgeon to the assistant and the surgeon's remote location away from the bedside. Tertiary academic care centers such as ours use various bedside assistants and have lately used more surgical technicians and surgical assistants at the bedside to free up residents for more robotic console learning. 2 Hands-on simulation has the potential to allow surgeons/assistants to develop skills in a risk-free environment and avoid potential medico-legal aspects of surgical training. 7 This article is an attempt to assess the value of a three-part hands-on robot assistant course for an experienced RARP team.
Although robotic technology offers a magnified view and an ergonomically comfortable environment for the surgeon, the same cannot be said for the bedside assistant. 8 The bedside assistant in our case is placed on the patient's right-hand side with the surgical monitor directly across the table on the patient's left-hand side. The assistant is then asked to assist deep in the pelvis, which is located directly to the right. This arrangement can be very ergonomically disorienting. Our hands-on drills were focused on the assistant standing on the right-hand side of the training box and looking across the table at a monitor while performing the tasks to their right (Fig. 2). While this may seem more intuitive to surgeons with extensive laparoscopic training, it can be very disorienting for untrained surgical technicians, surgical assistants, and new residents.
Sur and associates 4 used a step-by-step video to aid in training of bedside surgical assistants during robotic and laparoscopic prostatectomy. The video focused on the assistants aspirating, applying traction, passing needles, cutting suture, placing clips, exchanging instruments, and removing suture. The participants also participated in an Intuitive Corporation-sponsored (Sunnyvale, CA) instructional course. The authors describe the video contents in detail but do not provide data as to the satisfaction of the learners, whether or not their confidence increased, and whether or not it had clinical benefit. Six of our 13 assistants found the step-by-step training video to be the most helpful phase of the course. One must assume that being able to visualize each step of RARP and having a description of what is expected of the assistant during each step outlined is invaluable to an assistant of any level of experience.
The other seven assistants found the hands-on drills to be the most helpful portion of the course. A recent examination of practicing urologists and urologists-in-training completing the Basic Laparoscopic Urologic Surgery training curriculum found that 98% of participants thought this type of hands-on curriculum using training boxes should be standard for all residents in training. 9 A similar program has been developed and validated for trainees called Program for Laparoscopic Urology Skills. 10 The drills for each of these two programs are based on those of the FLS with the removal of the knot tying requirement. 9 –11 Because the bedside assistant in RARP is never asked to suture tissue or throw knots, the curriculum in this exercise was altered to fit the anticipated needs of a RARP bedside assistant.
Sgarbura and Vasilescu 1 found that robot teamwork satisfaction increased as familiarity and training with the technology increased. They noted, however, that resident-in-training satisfaction increased more readily if residents were offered time on the console earlier. Surgical technicians and surgical assistants will never receive robotic console time. Therefore, it is important to keep the assistant satisfaction high for nonphysician bedside assistants. The authors also note that familiarity with the procedure cuts down on the need for console surgeon/bedside assistant communication. This is important because of distance playing a role in altering verbal communications.
This type of simulation training is desired by surgical nurse assistants for laparoscopic surgery. A recent study found that a majority of laparoscopic nursing assistants were interested in simulation training and thought it would make them safer and improve their surgical assistant ability. 3 The same study, however, found that nurse assistants were unlikely to train outside of working hours and that it was difficult to find time for training. The three-phase model completed on 3 separate days was instrumental in having all of our identified assistants complete the course in a determined time frame.
A few issues with our study deserve comment. Our experienced robotic team found great value and high overall satisfaction with this course. It is expected that novice teams would benefit from a similar course, but that is not certain. Our institution uses the fourth robotic arm, thereby eliminating the need for two assistants. An institution that uses a three-arm system may find more value in tailoring the course toward that goal as well as having assistants who are facile from both sides of the surgical table. In our circumstance, the hands-on simulation module focused on the assistant's view and feel from the patient's right-hand side. Some surgeons feel more comfortable with the fourth arm on the patient's right-hand side to allow for passage of material between graspers in the right and left hand. If that is the case, the drills would have to be modified to accommodate a learner standing on the patient's left side. If the 5-mm port is eliminated from the surgeon's armamentarium, the drills involving right and left hand could be eliminated as well. One aspect of the course that can be improved is simulating prostate pedicle clip placement, which was not exercised in this course; however, new methods of simulating vascular clip placement are being developed. 9
As with many simulation exercises, we do not have evidence that this curriculum will improve patient outcome or prevent morbidity in the future. In essence, the simulation lacks concurrent validity. Concurrent validity would only be able to be assessed if an objective measurement of learner performance during RARP was undertaken in subjects who completed the course and compared with a group who did not complete the course. 12 All learners, however, thought that they benefited from this course and all thought it should be given annually. Twelve of 13 learners felt more confident after the course and thought that this type of course should be replicated for other high-volume surgical procedures. This gives the simulation face validity in that a group of nonexperts believes that the simulation represents a facsimile of the actual procedure, as intended. 12
This course took place over three separate morning sessions to avoid the cost of doing the course during normal working hours. Breaking the course into three separate sessions may have improved learner attention. The fact that all 13 members participated in the three phases without mandate demonstrates the desire for this type of hands-on and step-by-step instruction throughout the operating theater even in the presence of an experienced team. Future avenues of an exercise such as this include creating “passing” criteria to be a bedside assistant and the creation of periodic competency evaluations for bedside assistants.
Conclusion
A three-phase hands-on robotic training course tailored to assistants for RARP increases robotic team satisfaction and is desired by the assistants even with an experienced robotic team. All learners thought that this type of course should be repeated annually and replicated for other high-volume operative procedures. Further studies are needed to assess the benefit of such a course for novice robotic teams and with other robotic procedures.
Footnotes
Disclosure Statement
No competing financial interests exist.
Abbreviations Used
Appendix Robotic Prostatectomy Assistant Course Follow-Up Questionnaire