
Abstract
Purpose:
To describe a novel technique for a single setup approach for robotic radical nephroureterectomy (RANU) that does not require patient repositioning, port reassignment, or redocking of the robotic arms.
Materials and Methods:
Twenty consecutive patients underwent RANU at a single institution between January 2009 and January 2012. We implemented a unique port placement strategy based on a modified paramedian line (MPL), which allowed sufficient access to both the upper abdomen and the deep pelvis for radical NU with bladder cuff excision and concomitant lymphadenectomy.
Results:
The mean operative time was 161.3 minutes (range 91–330 minutes), mean estimated blood loss was 98.8 (range 50–200), and the mean hospital stay was 3 days (median 2 days, range 1–16 days). None of the procedures were converted to open or required blood transfusions. Lymphadenectomy was performed on 16 out of 20 patients, and the mean number of lymph nodes removed per patient when lymphadenectomy was performed was 14.1 (range 2–35). Three patients had positive lymph nodes. One patient had prolonged postoperative ileus, and one had a hospital course that was complicated by pneumonia. Mean patient follow-up was 13.5 months (range 1–24 months); one patient was found to have a recurrence at 3 month follow-up.
Conclusion:
The use of our MPL line for novel port placement allows for an effective, efficient, and reproducible method for RANU without the need for repositioning of the patient or the robot.
Introduction
The da Vinci® surgical robot platform (Intuitive Surgical, Sunnyvale, CA) has been shown to overcome certain limitations of conventional laparoscopy, while maintaining many of the advantages inherent to minimally invasive surgery. 13,14 Computer-assisted robotic surgery provides high definition, three-dimensional vision, tremor-filtering, wristed instrumentation, up to 10×magnification, and improved ergonomics for the surgeon. At the same time, robotic surgery maintains the benefits of laparoscopic surgery such as smaller incisions, decreased analgesic use, and shorter hospital stay. Early series of robotic radical nephroureterectomy (RANU) with bladder cuff excision include the need for patient repositioning, and undocking and redocking of the robot to provide access to the deep pelvis for the dissection of the distal ureter and bladder cuff. These readjustments were initially made to account for the limited working field of the robotic instruments and camera. An additional 30–60 minutes of operating room time has been required to reposition the patient in some series. 10 –12 Recently, different strategies for port placement have been proposed to circumvent the inherent limitations in robotic arm and camera mobility. 9,11 These previously described techniques, however, require port reassignment strategies and redocking of the robotic arms; this adds complexity to the procedure and may be challenging to less experienced robotic surgeons. Herein, we describe a novel and simplified port placement strategy that allows for a single setup approach for RANU. Our completely robotic technique does not require patient repositioning, port reassignment, or redocking of the robotic arms.
Materials and Methods
Retrospective chart review
Patient charts for 20 consecutive patients who underwent RANU at a single institution between January 2009 and January 2012 were reviewed. Analysis of the institutional review board approved database involved preoperative variables, which included patient age at time of surgery, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) surgical classification, abdominal computed tomography (CT) scan findings, urine cytology, retrograde pyelogram, and ureteroscopy; and operative variables, which included operative time, estimated blood loss, and lymph nodes removed; and postoperative variables, which included length of hospital stay (days), final pathology report, histological grade, and positive lymph nodes. Operative time was defined as beginning at skin incision and ending at closure of the final port site.
Surgical technique
Indication
The primary indication for this procedure was TCC of the ureter, renal pelvis or intrarenal collecting system. None were deemed amenable for endoscopic treatment. All surgeries were performed by a single surgeon (D.D.E.). None of these patients were treated with neo-adjuvant chemo or radiotherapy. All patients were counseled that they may receive a retroperitoneal lymphadenectomy if they had a bulky tumor or suspicious findings intraoperatively.
Presurgical evaluation
All patients had confirmation of an upper tract tumor by positive pathology, radiographic imaging, or endoscopic visualization. All patients had a negative cystoscopy to confirm absence of bladder tumor and all patients had a negative CT chest and nuclear medicine bone scan prior to proceeding to RANU. In cases where a ureteral stent was placed, the stent was endoscopically removed before proceeding to RANU.
Position of the patient
All patients were positioned in full flank, with the table in full flexion (see Fig. 1). Pillows or a soft cylindrical roll were used to support the patient posteriorly. The lower arm was placed on a padded arm board and positioned perpendicular to the table axis, while the upper arm was placed at the patient's side in anatomic position. We did not use an arm rest to support the upper arm to avoid interference and collisions with the robotic arms.

Patient in full flank with table in full flexion.
Port placement
Since optimal port placement is critical for our RANU technique, the port sites are carefully mapped after establishing a full pneumoperitoneum. A total of five ports are used in the procedure and are placed in the following order: The initial port (Port 1) is a 12 mm assistant port, which is placed just above the umbilicus. The next four ports are placed in specific order from cephalad to caudad along a modified paramedian line (MPL); this line is drawn from the midpoint of the axilla (cephalad) to the insertion of the rectus abdominis at the pubic symphysis (caudad). This line should approximately form a 20° angle from the longitudinal axis. The second port (Port 2) is an 8 mm robotic instrument port and is placed 2 cm (1 finger breath) caudally from the costal margin, along the MPL. The third port (Port 3) is a 12 mm robotic camera port and is placed 8 cm (4 finger breaths) caudally from Port 2 along the MPL. The fourth port (Port 4) is an 8 mm robotic instrument port and is placed 8 cm (4 finger breaths) caudally from Port 3 along the MPL. The fifth port (Port 5) is an accessory 8 mm robotic instrument port and is caudally placed 8 cm (4 finger breaths) from Port 4 along the MPL (see Fig. 2).
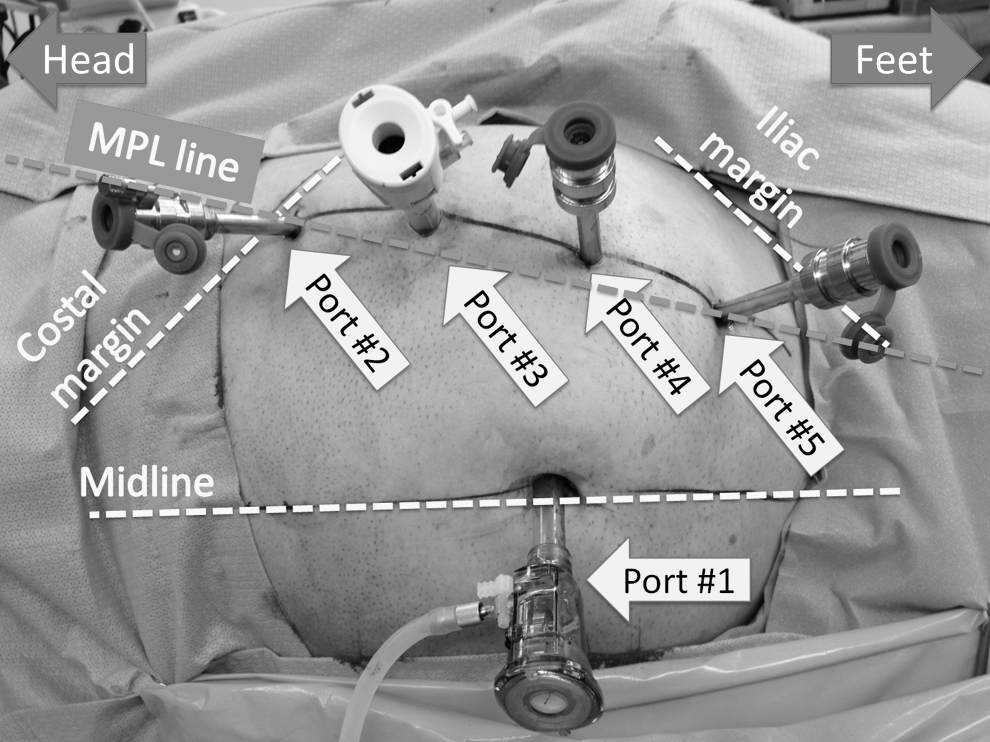
Modified paramedian line (MPL) and port placement. The MPL extends from the midpoint of the axilla (cephalad) to the insertion of the rectus abdominis at the pubic symphysis (caudad). Port 1, 12 mm assistant port; Port 2, 8 mm robotic instrument port; Port 3, 12 mm robotic camera port; Port 4, 8 mm robotic instrument port; Port 5, accessory 8 mm robotic instrument port.
For right sided cases, a 5 mm non traumatic laparoscopic locking grasper is percutaneously introduced at the subxyphoid location without a port. It is gently positioned under the liver as a liver ret ractor and locked into place on the peritoneal surface overlying the diaphragm.
Dissection of the kidney
To minimize arm collision during the initial portion of the case, Port 5 (robotic third instrument arm) is left undocked until the bowel is fully mobilized and the ureter is located. A 0° camera can be used for the whole case and changing to a 30° camera is not necessary.
The ipsilateral colon is mobilized to expose the kidney and hilum using a monopolar hook in the right hand and Maryland bipolar grasper in the left hand. The peritoneum is laterally incised to the colon along the white line of Toldt, and the avascular plane between the posterior mesocolon and anterior Gerota's fascia is developed. Left-sided operations require release of the splenocolic and renocolic ligaments and careful dissection away from the pancreatic tail and splenic vessels. During a right-sided operation, the attachments between the liver and kidney are released, and careful duodenal mobilization is required to expose the lateral aspect of the inferior vena cava.
Once the ureter and gonadal vein are identified, the third robotic instrument arm is docked and a 55 mm Grasping Retractor robotic instrument is introduced to provide lateral retraction of the ureter and kidney. This lateral traction effectively place the hilum on traction, facilitating hilar dissection. Except in cases with very distal ureteral tumors, an extra large Hem-o-loc Weck clip (Teleflex Medical, Research Triangle Park, NC) is placed in the distal ureter to prevent downward efflux of tumor cells into the bladder during renal manipulation. Once the medial aspect of the kidney and hilum is dissected, the hilum is usually divided after placement of multiple extra large Hem-o-loc Weck clips (Teleflex Medical) on the vessels.
Lymphadenectomy
If there is any suspicion of lymphadenopathy on preoperative imaging, intraoperative findings, or if the primary tumor is felt to be bulky, a retroperitoneal lymphadenectomy is performed for staging purposes. The lymph node dissection template differs according to the operative side. On the right side, we typically remove precaval and retrocaval node beds between the adrenal gland and the caval bifurcation. For left sided cases, our template includes the preaortic and retroaortic lymph nodes between the adrenal bed and the aortic bifurcation. The interaortocaval region is not dissected unless there is a clinical or imaging based suspicion. After controlling and dividing the hilar vessels and before the takedown of the lateral and superior attachments of the kidney, the lymph nodes along the ipsilateral great vessels are carefully inspected. When necessary, lumbar branch vessels are clipped using robotically applied large Hem-o-loc Weck clips (Teleflex Medical) and divided to enable a more thorough lymph node dissection.
Dissection of the ureter, bladder cuff, and cystorrhaphy
Once the remainder of the kidney is mobilized, the dissection is directed down the pelvis to mobilize the distal segment of the ureter. Once the ureter crosses over the common iliac artery, the view of the pelvis can be disorienting due to the lateral patient positioning. It is advisable at this point to survey the pelvis and consider the locations of landmarks such as the major vasculature, obturator nerve, pubic bone and bowel before proceeding. During the distal dissection of the ureter, reliable landmarks that will be encountered will be the superior vesical artery followed by the inferior vesical artery. The inferior vesical artery in a male and the uterine artery in a female is a consistent structure that posteriorly originates from the internal iliac artery and marks the beginning of the transmural portion of the ureter and the bladder cuff. These vessels should be clipped or carefully controlled as this may be a source of persistent hemorrhage. The bladder cuff is usually dissected using blunt dissection and focused cautery is greatly facilitated by an assistant who provides gentle and directed retraction of the proximal ureter. Once the bladder cuff is adequately mobilized from its muscular attachments and is attached only at the mucosa, it will have a characteristic tapered appearance that will indicate the completion of the bladder cuff dissection. Before transection of the bladder cuff, a 9 inch 2-0 absorbable barbed suture on a V 20 needle (VLOC; Covidien, Mansfield, MA) is placed as a holding stitch, lateral to the bladder cuff. Next, the bladder cuff is sharply transected and the preplaced holding stitch is used to run a two or three layer water-tight bladder cuff closure, paying close attention to re-approximate the mucosal edges in the first layer closure. In addition, the medially placed sutures must be carefully placed and not too widely as to not obstruct the contralateral ureteral orifice. Indigo carmine is administered to confirm that the contralateral ureteral orifice remains unobstructed after our suture placement.
The bladder is tested with 300 cc to ensure that the cystorrhaphy is water tight before specimen extraction. We did not place an abdominal drain. The caudal-most port site (Port 5) is then dilated to introduce a 15 mm specimen extraction bag and the incision is slightly extended to make a muscle splitting mini-Gibson incision for specimen extraction.
Postoperative follow-up
Postoperatively, all patients were followed up with serial chest and abdominal imaging, cystoscopy, and laboratory studies every 3 months for year 1, every 6 months for year 2, and every 12 months thereafter.
Results
All 20 consecutive patients underwent RANU by a single surgeon (D.D.E.) at our institution between January 2009 and January 2012. There were 9 men and 11 women in the study. The mean age of the patients at time of surgery was 70.7 years (range 25–99 years), the mean BMI was 27.8 (range 17.7–38.7), and the mean ASA was 2.5 (range 2–3). In addition to radiographic findings of a collecting system lesion, 12/20 patients had confirmation of upper urinary tract urothelial carcinoma by cytology and/or biopsy. Patient preoperative variables are shown in Table 1.
ASA=American Society of Anesthesiologists; BMI=body mass index; CT=computed tomography; MRI=magnetic resonance imaging; TCC=transitional cell carcinoma.
The mean operative time was 161.3 minutes (range 91–330 minutes). The mean estimated blood loss was 98.8 mL (range 50–200 mL), and the mean hospital stay was 3 days (median 2 days, range 1–16 days). Lymphadenectomy was performed on 16 out of 20 patients, and the mean number of lymph nodes removed per patient when lymphadenectomy was performed was 14.1 nodes (range 2–35). Three patients had positive lymph nodes. None of the procedures necessitated open conversion or blood transfusions. All patients were given a clear liquid diet on postoperative day 0 and all patients were advanced to a regular diet by postoperative day 1. One patient had postoperative ileus and one patient had bilateral atelectasia and pneumonia.
Pathologic analysis showed 17 patients with TCC, 1 patient with papillary renal cell carcinoma, 1 patient with collecting duct renal cell carcinoma, and 1 patient with chronic pyelonephritis. Of the 17 patients with TCC pathology, 7 were low grade and 10 were high grade. Staging revealed seven patients with pTa, six patients with pT1, one patient with pT2 and two patients with pT3, and two patients with pT4. One patient was found to have positive surgical margins. The mean follow-up time was 13.5 months (range 1–36 months). One patient was found to have a recurrence of TCC in the para-aortic lymph nodes on a 6 month follow up CT scan. A summary of operative and postoperative variables are shown in Table 2. One patient was found to have a biopsy proven recurrence of a para-aortic lymph node on a 6 month follow-up CT scan.
N/A=not applicable.
Two patients experienced a postoperative complication: one patient had a prolonged postoperative ileus (Clavien-Dindo Classification grade II); one patient had postoperative pneumonia (Clavien-Dindo Classification grade II). 15
Discussion
Traditionally, an open NU has been the gold standard treatment for patients with upper tract TCC. A major source of morbidity of the open approach includes the large single abdominal incision or two smaller counter incisions. Due to advances in minimally invasive techniques, an increasing number of surgeons have been performing LNU, since the first reported LNU in 1991. 3 Cohort studies comparing perioperative, short, and intermediate oncologic outcomes between open NU and LNU have showed that there were no statistically significant differences between the two approaches. 16 –18 Further, LNU has been associated with decreased hospital stay, less estimated blood loss, and reduced analgesia use by the patient. 18 –22
Currently, there is no standardized technique for minimally invasive NU. A major difficulty with pure LNU is the required complex bladder cuff dissection and reconstruction. Several minimally invasive modifications to addressing the distal ureter, such as endoscopic stripping or pluck-off techniques have been reported. Disadvantages of these various methods have been described. The laparoscopic stapling technique maintains a closed system but risks leaving tumor within the staple line for distal ureteral tumors. 4,23,24 Some authors have mentioned risk for stone formation at the staple line. 21 Transvesical laparoscopic ureterectomy with previous ligation is a valid approach with good oncologic results but is technically difficult and requires a two-stage approach with repositioning. Transurethral resection of the ureteral orifice and intussusception techniques have been also described but requires repositioning and also poses the risk for seeding. 4,23
The da Vinci robotic interface has been used as a potentially transformative tool for LNU and may decrease the technical difficulties inherent to the distal ureter dissection and cystorrhaphy. There have been a variety of approaches proposed for RANU. Initial experiences in RANU described a two-stage technique in which the patient was initially positioned in the flank position for nephrectomy and then was repositioned to supine lithotomy for the distal ureter dissection and cystorraphy. This two-stage approach highlighted the need for increased operative time due to time spent repositioning the patient and/or redocking the robot. Nanigian et al used a laparoscopic approach for nephrectomy, and a robotic approach for bladder cuff management. 10 Rose et al used a robotic approach for nephrectomy, and an open approach for bladder cuff management. 12 Both aforementioned studies required that the patient be repositioned from the flank to supine position. 10,12 Park et al used a robotic approach for both nephrectomy and bladder cuff management using a dual-port system. This technique required piggybacking of ports for the robotic trocars and repositioning of the robot when moving from nephrectomy to bladder cuff management. 11
Some authors have proposed different strategies to overcome the problem of spending operating room time to reposition the patient and/or the robot. Eun et al described a four-port “baseball diamond” technique that was successfully performed on a cadaver, without the need for repositioning of the patient or robot. 8 Recently, Hemal et al proposed a unique port placement scheme that allowed for a smooth transition from nephrectomy to bladder cuff management, without the need for repositioning of the patient. Although repositioning of the patient was not required, Hemal et al's technique did require reassignment of the ports and redocking the robotic arms for ureterectomy and bladder cuff repair. The results of this series showed decreased operative time, estimated blood loss, and hospital stay compared with prior RANU studies. Further, there were no reported complications and none of their procedures were converted to open. 9
Our particular technique is novel in that it enables the surgeon to perform a single modality operation with a single setup that does not require port reassignment, patient repositioning, or robotic redocking. This is made possible by a unique port placement strategy that utilizes the MPL line. This study is our initial experience with RANU and, to our knowledge, is the largest published case-series of RANU to date. However, as RANU is still a relatively new procedure, we are unable to provide a meaningful statistical comparison of our particular approach to alternative approaches for RANU, and/or laparoscopic and open approaches for NU.
Nevertheless, our study showed that our unique technique for RANU is feasible, demonstrates good oncologic outcomes, and is associated with minimal complications.
One patient was found to have a biopsy proven recurrence of a para-aortic lymph node on a 6 month follow-up CT scan. This was treated with salvage chemotherapy followed by a robotic retroperitoneal lymph node dissection and radiation therapy. To date, 1 year since his salvage surgery, the patient has no evidence of disease. Two of 20 patients in our study experienced a complication. First, one patient had a complicated case of postoperative ileus that led to a prolonged hospital stay of 16 days. This patient was managed with nasogastric tube and parenteral nutrition, prior to gradually advancing her diet. Second, one patient had postoperative pneumonia, and was managed with antibiotics and supportive therapy. The patient who had pyelonephritis on final pathology had prior segmental ureterectomy for TCC of the mid ureter. Although there was no evidence of recurrence, the ureter developed a stricture and the kidney suffered subsequent renal deterioration, so a completion RANU was performed.
Lymphadenectomy in the setting of a NU may have diagnostic utility, but because there is no clear therapeutic benefit, it is currently not routinely performed. Given the advantages of enhanced visualization and wristed instrumentation, the robot provides unprecedented access to the renal hilar, para-caval, and para-aortic lymph node beds. This is the first minimally invasive series to routinely perform a concomitant retroperitoneal lymph node dissection. Lymphadenectomy was performed on 16 out of 20 patients, and the mean number of lymph nodes removed per patient when lymphadenectomy was performed was 14.1 nodes (range 2–35). Three patients had positive lymph nodes. These patients were referred to medical oncology and treated with adjuvant chemotherapy.
Through our experience with RANU, we feel as though our novel technique provides a simplified, one-step method of performing RANU while adhering to open oncologic principles and without making compromises in accessing the distal ureter and bladder cuff. As aforementioned, one limitation of this study was the limited number of patients included in our study, which precludes us from making statistically significant comparisons to laparoscopic and open NU. Also, due to the relatively short follow-up period, we are unable to provide long-term outcomes of our technique. In spite of this, we feel as though our approach to RANU is feasible, safe, and easy to reproduce. The durability of RANU could be improved in future studies by combining multi-institutional data and longer oncologic follow-up.
Conclusion
The use of our MPL line for novel port placement allows for an effective, efficient, and reproducible method for RANU without the need for repositioning of the ports, patient, and the robot.
Footnotes
Disclosure Statement
Ziho Lee and Ronald Cadillo have no conflicts of interest or financial ties to disclose. David Lee receives study support from Johnson and Johnson and Pfizer and is a lecturer for Intuitive Surgical, Ethicon Endosurgery, and Covidien. Daniel Eun was a surgical proctor for Intuitive Surgical and is a lecturer for Ethicon Endosurgery and Covidien.