
Abstract
Purpose:
Stringent radiological follow-up is essential after renal tumor ablation. Drawbacks of postablation follow-up by contrast-enhanced computed tomography (CECT) are the associated ionizing radiation and nephrotoxic contrast agent. Contrast-enhanced ultrasound (CEUS) has shown potential to demonstrate microvasculature without using either ionizing radiation or toxic contrast agent. We assessed the concordance of enhancement patterns of CEUS and CECT/MRI in cryolesion assessment after laparoscopic renal cryoablation (LCA).
Methods:
From 01/2006 to 01/2009, a CEUS was performed before and after LCA (3 and 12 months) in addition to regular CECT/MRI. Using an enhancement score (0=no enhancement, 1=rim enhancement, 2=diffuse enhancement, 3=localized enhancement, 4=no enhancement defect), the cryolesion was assessed by both modalities, and concordance of enhancement score was assessed.
Results:
In total, 45 tumors were included (29 biopsy proven renal cell carcinoma (RCC), mean size 2.66 cm). One cryoablation failed, resulting in a nonenhancing cryolesion apart from the persisting renal tumor. There were no postablation recurrences during the study period.
Pre-LCA: Both modalities were available in 26 cases. In 20 out of 26, there was concordance of enhancement score (77%, all cases score 3 or 4). Three months: Both modalities were available in 32 cases. Enhancement score corresponded in 23 out of 32 cases (72%). Seven cases showed enhancement on CECT/MRI (“1” in six cases, “4” in one case) with enhancement score “0”on CEUS. Two cases showed enhancement on CEUS without enhancement on CECT/MRI (specificity 92%, negative predictive value [NPV] 77%). Except one case, all enhancement resolved on subsequent imaging. Twelve months: Both modalities were available in 21 tumors. Enhancement score corresponded in 19 out of 21 cases (91%). Two cases showed enhancement on CEUS without enhancement on CECT/MRI (specificity 90%, NPV 100%).
Conclusion:
This pilot study shows that CEUS is a safe imaging technique with high concordance of enhancement score between CEUS and CECT/MRI. While cross-sectional imaging seems sensible to demonstrate successful ablation at first follow-up, CEUS might be used to diminish the burden of contrast-enhanced cross-sectional imaging in the long-term follow-up.
Introduction
Unfortunately, the routine use of CT scans in the follow-up has several major drawbacks, including the unavoidable ionizing radiation and the nephrotoxicity of the iodine-based contrast agent. This potential toxicity will have a higher impact in younger patients and in those with an already impaired renal function. MRI as a follow-up alternative is costly and requires use of a gadolinium, which is reported to be potentially nephrotoxic when administered in patients with renal impairment. 6 –8
Recently, contrast-enhanced ultrasound (CEUS) has emerged as a diagnostic tool in several fields, in medicine, cardiology, and liver tumor diagnostics in particular. 9 CEUS is based on ultrasonography and uses stabilized microbubbles to improve the echogenicity of blood flow. CEUS can provide real-time information on the enhancement properties of tissue under study without using ionizing radiation or nephrotoxic contrast agent. This represents a major advantage compared with contrast CT/MRI scans.
Reports on CEUS as a potential diagnostic method for evaluation of radiofrequency ablation (RFA) of kidney tumors showed promising results. 10,11 However, very little is known on the value of CEUS to evaluate the cryoablated kidney tumors. 12
The primary objective of this study was to assess the concordance of enhancement patterns of CEUS scans and CT/MRI scans (gold standard) in the follow-up after CA.
Methods
Patients
From January 2006 to March 2009, a prospective study on CEUS on patients treated by laparoscopic CA (LCA) of a renal tumor was conducted in our center. The local Institutional Review Board approved the study. Patient selection, the interventional procedure, and follow-up protocol have been described earlier. 13 After obtaining informed consent, CEUS was performed in addition to the clinical protocol at three points in time (before LCA and at 3 and 12 months after ablation). Interval between CT/MRI scan and CEUS imaging was maximally 10 days. In the frame of an investigational study, patients were able to refuse participation in the study at any point in time and to join the study after LCA.
Collection of imaging studies: CT/MRI scan
Preablation CT and MRI scans were performed either in the radiology department of our institution or in case of referrals (48%), the images were integrated in our hospital computer system. CT scans in our institution were performed using a Philips 4-slice MX8000 or a 64-slice Brilliance CT scanner (Philips Healthcare, Best, The Netherlands). For contrast enhancement, Ultravist 300 (Bayer Pharma AG, Leverkusen, Germany) was injected at a rate of 4 mL/s and a total maximum of 120 mL. Preoperative CT scans consisted of a four-phase abdominal 3 mm CT scan (unenhanced, arterial scan at 45 seconds, venous phase at 115 seconds, delayed phase at 10 minutes after injection of contrast), and follow-up scans were performed according to a predefined scanning protocol developed in collaboration with the department of Radiology of our institution consisting of a triple-phase 3 mm scan (unenhanced, arterial and venous phase). In case of a contra-indication for contrast-enhanced CT (CECT) scanning (e.g., intolerance of iodine-based contrast or a serum creatinine >130 μmol/L), a contrast-enhanced MRI was performed using a Siemens Avanto 1.5 Tesla MRI scanner (Siemens AG Healthcare Sector, Erlangen, Germany) with 16-channel body array coils. Standard protocol consisted of T2-trufi coronal and transversal series with fat suppression, a contrast-enhanced T1-fl2d sequence in and out of phase, T2-haste (transversal and coronal), and T1 vibe transversal with both unenhanced and dynamic series (at 30 seconds, 60 seconds, and 15 minutes with 3 mm slices). Images were acquired during breath hold in inspiration and using Gadovist® 1.0 (Bayer Pharma AG) for contrast enhancement.
Collection of imaging studies: CEUS
For all CEUS imaging, a Siemens “ACUSON Sequoia” ultrasonography device with contrast pulse sequence (CPS) imaging was used. 14 CEUS was carried out in an out-patient setting by a urologist or urology researcher with experience in performing renal ultrasonography.
After preparation of the patient, including placement of a venous cannula in the antecubital vein, grayscale ultrasonography was used to localize the renal mass or cryolesion. After a slow intravenous injection of 2.4 mL of CEUS contrast agent SonoVue® (Bracco, Milan, Italy), the contrast-enhanced images showing the renal mass or cryolesion were recorded using CPS imaging. When necessary, an additional injection of 2.4 mL of SonoVue was administered to extend the time available for CEUS investigation. All recorded cineloops were stored for offline evaluation. All cineloops and on-screen display functions were encrypted to enable blinded evaluation of the images after censoring the study.
Assessment of images
In order to assess the images, we utilized the descriptive enhancement score previously developed at our institution (see Discussion section). 12 The score consists of a scale: from 0 to 4 were “0” represents no enhancement at all, “1” represents presence of a tiny peripheral rim enhancement, “2” represents weak diffuse enhancement, “3” represents nodular enhancement, and “4” represents absence of any enhancement defect in the lesion/full enhancement of the lesion. All CEUS scans were assessed by one investigator who was blinded to the CT/MRI scans and the clinical results.
For the reference test, the original clinical radiological report was retrieved and converted to a enhancement score. After determination of the degree of enhancement using the score, the data were subsequently entered in a Predictive Analytics SoftWare 18.0.2. database and merged with clinical and procedural data of the corresponding patients.
Analysis of results
For the comparative analyses at the three individual time points, cases with a missing CEUS and/or CT/MRI were excluded for analysis at that particular time point.
Concordance of enhancement score between cross-sectional imaging and CEUS was assessed. Furthermore, accuracy of CEUS with regard to the regular follow-up cross-sectional imaging was calculated using contingency tables. For the latter purpose, we dichotomized the enhancement scores with “0” being considered as negative and ≥1 being considered as positive.
The statistical setup of the analysis and the analysis itself were performed in close collaboration with the Department of Biostatistics of our center. Quantification was based on percentage agreement without correction for chance agreement, and specificity, sensitivity, negative predictive value (NPV), and positive predictive value (PPV) were calculated. Data were reported in adherence to the strengthening of the reporting of observational studies in epidemiology (STROBE) guidelines. 15
Results
In total, 45 cases (45 tumors) were included in the study with the characteristics being described in Table 1. In one patient, the ablation missed the tumor, resulting in one unsuccessful CA; all other patients underwent treatment successfully with no persistent or recurrent disease at 3 or 12 months of follow-up. There were no CEUS-related complications or adverse reactions due to administration of the SonoVue.
Biopsies without tumor cells or with insufficient tumor cells hindering differentiation between a benign and malignant tumor were classified as nondiagnostic.
Not 100% due to rounding of percentages.
CKD-EPI=chronic kidney disease epidemiology collaboration; eGFR=estimated glomerular filtration rate.
In total, 129 conventional cross-sectional scans (121 CT; 95%) and 115 CEUS scans were collected.
Pre-LRC
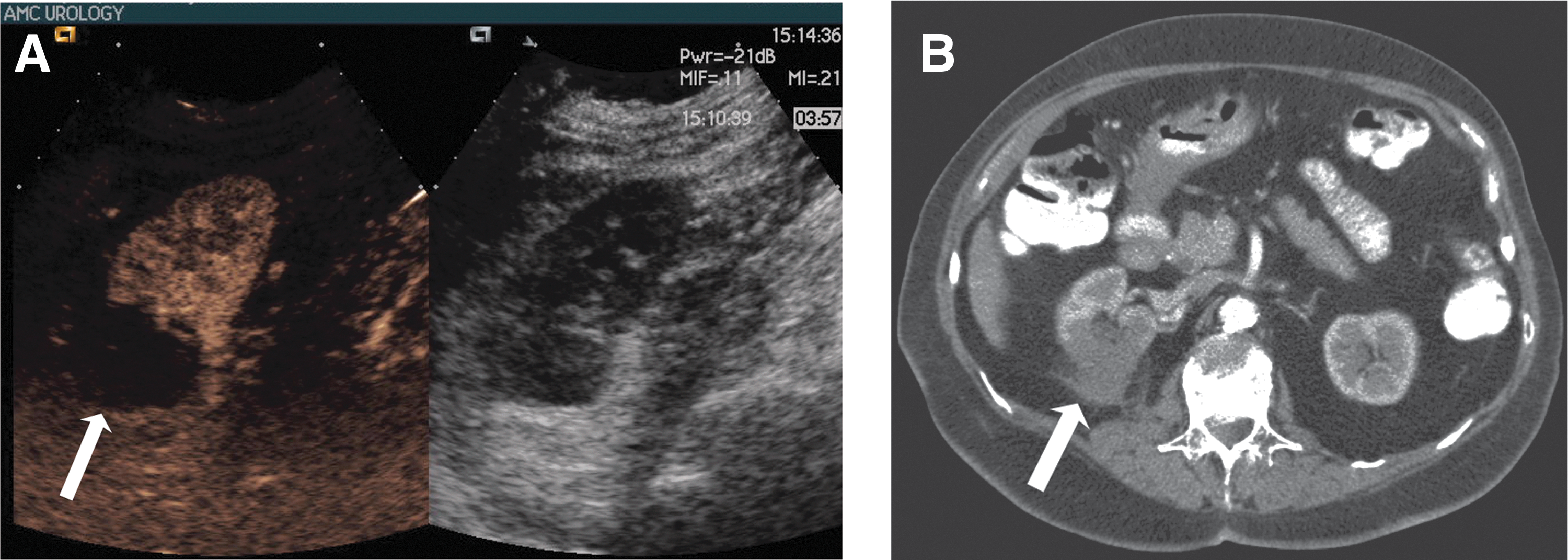
In 26 tumors, preablation scans on both modalities were present. In one case, an MRI was performed. An enhancing lesion was recognized in all cases and on both CT/MRI and CEUS with all cases presenting with an enhancement score of 3 or 4 on both the CT/MRI and CEUS. In 20 of 26 cases (77%), these scores were concordant (see Fig. 1).

Three months' follow-up
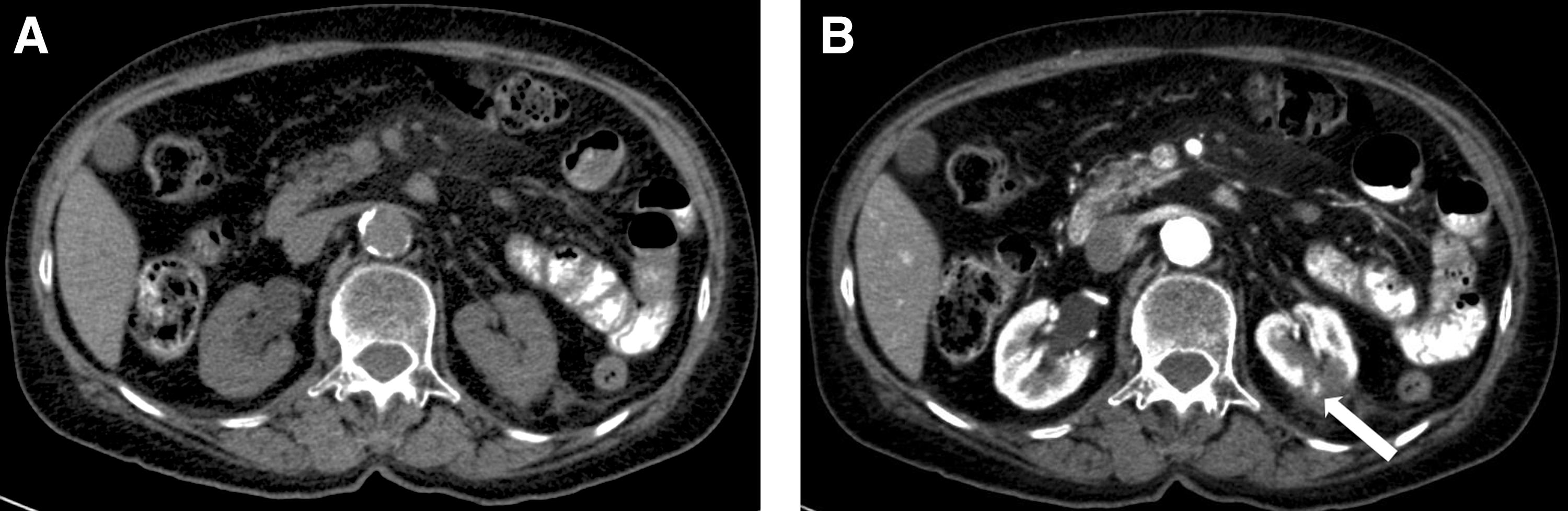
At 3 months after treatment, both CT/MRI and CEUS scans were available in 32 cases. In one case, an MRI was performed. There was a concordance of enhancement score in 23 cases (72%) (see Fig. 2). In 7 of 32 (22%) cases, there was enhancement on CT/MRI without enhancement on the corresponding CEUS. In the single tumor where the CA missed the tumor, there was enhancement of the tumor on CT/MRI (score 4) with a CEUS interpreted as score 0 (see Discussion section). In the six other cases, the enhancement on the CT/MRI scan concerned slight rim enhancement (score 1). These seven cases were considered false negatives (see Fig. 3).
Unenhanced
In two cases (6%), there were signs of enhancement on the CEUS (all score 1) without enhancement on the corresponding CT scan. These cases were considered false positives (Fig. 4). The contingency table (Table 2) shows a specificity and NPV of 92% and 77%, respectively.
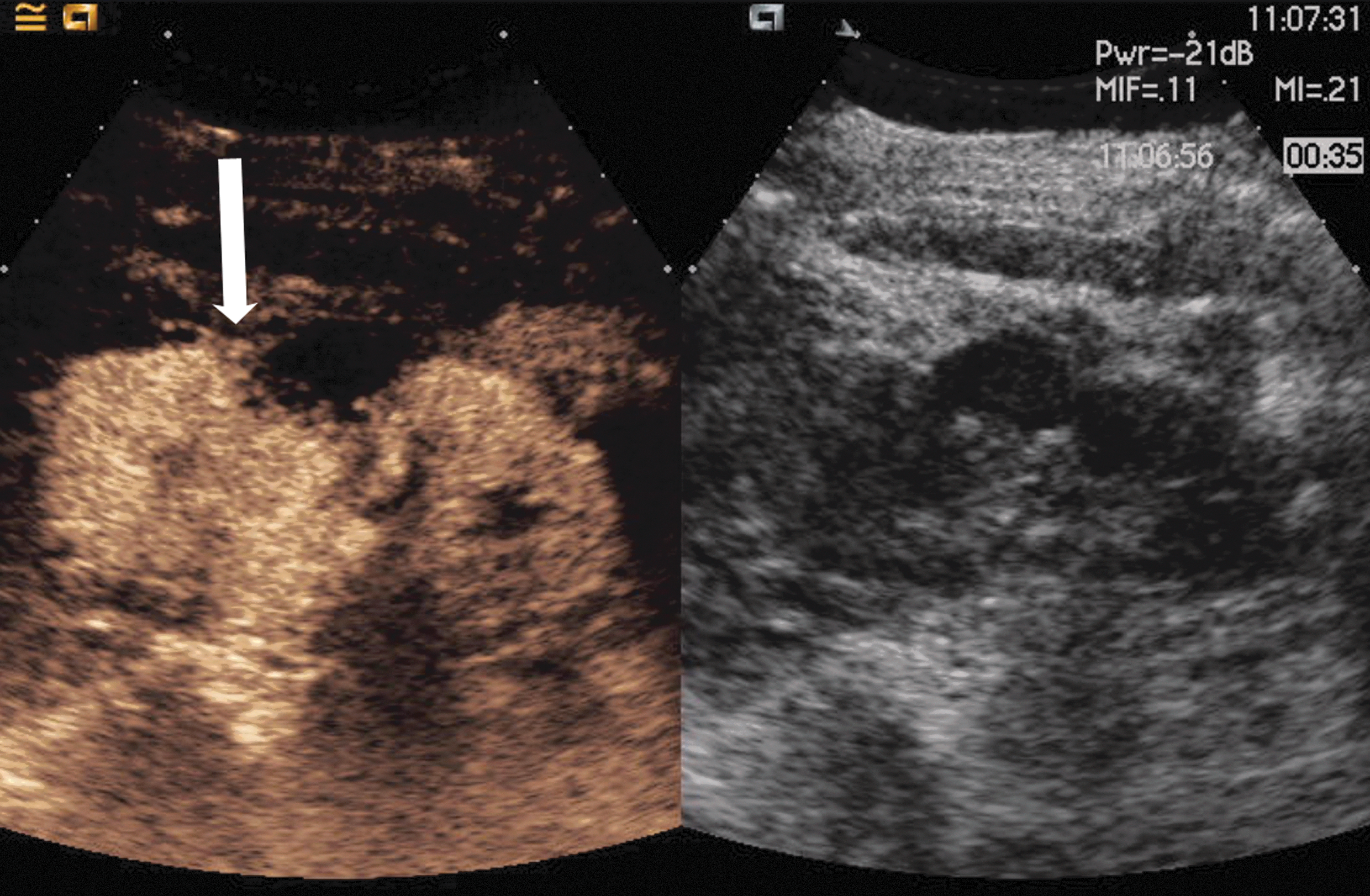
CEUS image 3 months after CA showing rim enhancement in the cryolesion (arrow). This was considered enhancement score 1.
Diagnostic accuracy of the CEUS against the CT/MRI scan shows a specificity of 92% and an NPV of 77%. Sensitivity and positive predictive value could not be assessed.
CEUS=contrast-enhanced ultrasound; NPV=negative predictive value.
Twelve months' follow-up
In 21 tumors, both modalities were present at 12 months after ablation. In two cases, an MRI was performed. The enhancement scores of CT/MRI and CEUS were concordant in 19 cases (91%). All CT/MRI scans were negative for enhancement, resulting in no false-negative CEUS. In 2 cases (10%), there were signs of enhancement on the CEUS (all enhancement score 1) without enhancement on CT. These cases were considered false positives. The contingency table (Table 3) shows a specificity and NPV of 90% and 100%, respectively.
Diagnostic accuracy of the CEUS against the CT/MRI scan shows a specificity of 90% and an NPV of 100%. Sensitivity and positive predictive value could not be assessed.
Discussion
Our study compares in a prospective longitudinal manner CEUS enhancement scores with conventional contrast-enhanced cross-sectional imaging in a cohort of renal masses treated by LCA. At diagnosis, all renal masses showed enhancement on both the CT/MRI and CEUS with an absolute concordance in terms of enhancement score in 77% of cases. During follow-up, absolute concordance in terms of enhancement score was 72% and 91% at 3 and 12 months, respectively. There were no adverse reactions due to the SonoVue or other aspects of the CEUS, demonstrating that CEUS is feasible, safe, and well tolerated.
The need for regular follow-up with CECT or MRI represents a major disadvantage of renal ablation. A multiphase scan of the abdomen delivers a median radiation dose of 31 (range: 6–90) mSv, resulting in one radiation-induced malignancy for every 660–700 of such scans in a 60-year-old patient. 7 Furthermore, most of them are older and have comorbidities, including an impaired renal function. In this setting, iodine contrast is potentially toxic, may worsen the impaired renal function, and potentially even lead to contrast-induced acute kidney injury. 16 Therefore, CT scanning is far from ideal in performing long-term follow-up after CA. However, several aspects prevent MRI from being the ultimate alternative for CT scanning, such as the high costs and lower availability. Furthermore, since the MRI contrast-agent gadolinium may cause nephrogenic systemic fibrosis in patients with a glomerular filtration rate <30 mL/min/1.73m2, performing an MRI in patients with severe renal impairment is also contra-indicated. 6 CEUS imaging requires an intravenous injection of microscopic gas bubbles and availability of an ultrasound device equipped with specific software. The contrast images provide real-time information of the enhancement pattern of the tissue, while it is harmless for the kidney regardless of the renal function. The technique has shown its power in the detection and evaluation of tumors in other organs such as the liver, and it is possible that CEUS will replace the CT angiogram to evaluate the function and endoleakage of vascular endoprostheses. 17 Recently, several reports have been published showing promising results of CEUS in the follow-up after RFA of renal tumors. 11 While extrapolation of these studies to cases ablated by cryotherapy is likely, no studies have explored the subject apart from a feasibility study. 12
Using an enhancement score previously described, 12 CEUS replicated the results of the CT during follow-up of small renal masses after CA. At 3 months (first control in our setting), CEUS had a specificity of 92% and an NPV of 77% when compared with CT/MRI, which increased to 90% and 100%, respectively, at 12 months.
There was one persistent tumor at 3 months in our series that was not detected on CEUS and also missed on conventional gray scale ultrasound. This tumor was a small 1.2 cm tumor that was missed during the CA, resulting in a cryolesion located caudal of the tumor with the tumor being untouched. Since the CEUS investigator was blinded to clinical results while performing the CEUS scans, the cryolesion caudal of the tumor was interpreted as a cryolesion without signs of residual enhancement, and the small tumor was more cranially overlooked. As a result, there were no CEUS images of the residual tumor to be assessed. Since in this initial pilot study all CEUS images were assessed by one single observer, this might be a reflection of one investigator's miss. Including multiple observers would be favorable to overcome this limitation.
Tumor persistence and recurrence occur in a low percentage of cases in all CA series; however, a long-term follow-up is of capital importance after CA, as recurrences may occur as late as after 58 months. 1,13 Based on our results, CEUS might substitute some of the repetitive cross-sectional imaging tests performed during this long-term regimen of follow-up. Determining the optimal interval between follow-up studies is an appraisal between (oncologic) safety and patient burden (both in terms of comfort and in negative aspects of the follow-up modality). However, being a noncross sectional imaging modality and focused on absence of enhancement in the cryolesion, other abnormalities in the kidney or the abdomen might be overlooked, which was also the case in our series with a persistent tumor located completely outside of the cryolesion. In a similar study comparing CT/MRI with CEUS after RFA, CEUS failed to detect a persistent tumor at 6 weeks in 3 of 14 cases compared to 0 with CT/MRI. 11 Therefore, it seems sensible to perform a cross-sectional study as a first follow-up study after ablation to demonstrate successful ablation. For the subsequent long-term follow-up, CEUS might be used to show absence of enhancement in the successfully ablated tumor, alternated by regular CT/MRI to detect abnormalities in other abdominal structures, including the contralateral kidney, resulting in a decrease of patient burden without compromising the oncologic safety.
At least two points deserve further comments, with the first one being related to the lack of radiological and clinical recurrences in our series. In fair strictness, we considered as positives those cases with enhancement score ≥1 at 3 and 12 months in both the index and the investigational test. However, clinical studies demonstrate that a tiny peripheral (rim) enhancement in cross-sectional imaging is present at the first evaluation in up to 26% of the cases and resolves later on. 18,19 Clinically, the cases with rim enhancement on cross-sectional imaging were not considered a radiological persistence but a finding deserving further cross-sectional evaluation. In our series as well, the rim enhancement disappeared later on in all cases when assessed by cross-sectional imaging. Negative cross-sectional imaging has proved to correctly demonstrate the absence of tumor persistence or recurrence after CA when verified by tumor biopsy. 5
The second issue is the appropriateness of the enhancement score used. There are no standardized scores to assess enhancement patterns in renal tumors and even less for postablation assessment. We, therefore, used a home-designed visual and an easy-to-use enhancement score with rather grade patterns of enhancement instead of intensity 12 and applied it retrospectively to CT and MRI. The absence of other scores precludes any comparison at the present time.
We acknowledge that technological developments currently enable raw CEUS data to be used for the calculation of time intensity curves (TIC) and several quantitative perfusion parameters. 20 We did not perform such calculations in this pilot study, as for our clinical question, an assessment of the entire cryolesion on CEUS is required rather than a TIC, which is based on a single-plane CEUS image. Second, similar calculations cannot be performed for CT/MRI images, which were considered the gold standard for comparison in this study.
To the best of our knowledge, no reports on cost effectiveness of CEUS after CA of small renal masses have been published, which is natural given the premature status of CEUS in this field. Although such economical assessments are highly setting dependent, one report showed a significant saving of costs when CEUS was used for the characterization of focal liver tumors compared with CT/MRI, and comparable results might be expected in the case of the long-term follow-up after renal CA. 21
While limitations inherent to ultrasound such as operator dependency and patient dependent factors cannot be overcome by CEUS and its use in renal masses is not yet approved by the FDA, 22 we postulate that CEUS might have a role in decreasing the cross-sectional imaging burden of the follow-up schemes after CA, although a study showing its ability to detect recurrences would further validate this.
Conclusion
CEUS is a safe imaging modality with a high specificity and NPV in the follow-up of cryoablated renal masses. The absence of recurrent tumors in this series hinders firm conclusions on sensitivity and PPV. While cross-sectional imaging should be used to demonstrate a successful cryoablation at first follow-up after ablation, clinical implementation of CEUS for further follow-up of the cryolesion can decrease the number of CT/MRI scans performed during follow-up.
Footnotes
Acknowledgment
This project is supported by the Cure for Cancer foundation.