
Abstract
Background and Purpose:
The optimal method of pain control after percutaneous nephrolithotomy (PCNL) remains controversial. We sought to determine whether intercostal nerve block with bupivicaine provided superior pain control, when compared with placebo, with a lower need for narcotics and improved health-related quality of life (HRQL) in the immediate postoperative period.
Patients and Methods:
Sixty-three patients were randomized to receive intercostal blockade with either 20 mL of 0.5% bupivacaine with epinephrine or 20 mL physiologic saline. All patients received intravenous narcotic patient-controlled analgesia (PCA) postoperatively. Data were collected on stone parameters, demographics, analgesic usage, length of stay, and HRQL as assessed by the Postoperative Recovery Scale.
Results:
The mean age was 47.7±1.2 years; mean body mass index was 28.0±5.0 kg/m2; mean stone diameter was 29.2±15.8 mm. Within the first 3 to 6 hours after surgery, there was a significant reduction in narcotic use for the group receiving intercostal nerve blockade with bupivacaine compared with placebo. At 3 hours, narcotic use was 2.4±3.1 mg vs 4.3±3.8 mg morphine equivalents (P=0.034), and within 6 hours of surgery, narcotic use was 5.9±6.1 mg vs 8.8±7.4 mg (P=0.096). Durable improvement in HRQL was also observed in patients receiving intercostal nerve blockade with bupivacaine compared with placebo (P=0.034). No complications were attributable to the intercostal nerve blocks in either group.
Conclusions:
Intercostal blockade with bupivacaine significantly improves both pain control and HRQL in the early postoperative period. The effectiveness of bupivacaine disappears within 6 hours of surgery, after which narcotic use becomes indistinguishable. Intercostal nerve blockade is an easy, safe, and inexpensive method that can be used to optimize pain control after PCNL.
Introduction
Another option in these patients is to augment pain control using regional anesthetic techniques. One such technique, intercostal nerve block, is a well-established form of regional anesthesia that has been successfully used after procedures such as nephrectomy. 6 We investigated the effect of intercostal nerve blocks with bupivacaine vs saline in patients undergoing PCNL on both narcotic use and health-related quality of life (HRQ) in the immediate postoperative period.
Patients and Methods
We conducted a prospective, double-blinded, randomized controlled trial of intercostal nerve block after PCNL. The trial was limited to patients who were undergoing PCNL solely for the management of stone disease, who were able to complete questionnaires in English, and whose preoperative plan was for a single (vs multiple) access tract. In addition, patients who were undergoing concomitant surgical procedures such as URS or endopyelotomy were excluded. All patients were followed up 1 week after PCNL. The study protocol was approved by our Institutional Ethics Review Board.
Technique
Single-tract PCNL was performed using the fluoroscopically guided “bull's eye” technique with the patient in the prone flexed position that we have described previously in detail. 7 Stone fragmentation and removal were accomplished using the Ultrasonic LUS-2 (Olympus) and/or Swiss Lithoclast (EMS) as needed. A complete, systematic flexible nephroscopy was performed with removal of any residual calculi using a tipless nitinol basket. At the completion of the PCNL procedure, nephrostomy drainage was secured using an 8.5F/6F internal/external nephroureterostomy tube (Cook Medical) in all patients.
Before the procedure, patients were randomized to either treatment arm by the research pharmacy. Medication was supplied in a 20 mL syringe so that the treating urologist was blinded to the medication received. After nephrostomy drainage was secured, patients underwent intercostal nerve blockade with 20 mL of 0.5% bupivacaine with epinephrine or 20 mL placebo (saline).
To ensure complete anesthesia of the adjacent chest and body wall around the nephrostomy tract, intercostal blocks were placed into the nerve sheath just below each rib, two ribs above and 1 rib below the PCNL tract (if applicable) (Fig. 1). This allowed anesthesia to be infiltrated into the dermatomes adjacent to the tract, to include cross-fibers between the dermatomes. Precise localization was performed using palpation of the targeted rib and fluoroscopic guidance as needed. The skin over the rib was retracted superiorly and the needle inserted onto the outer surface of the rib. The needle tip was used to probe the surface of the rib, after which tension on the skin was gradually released until the needle passed immediately below the rib margin. The needle was only inserted 2 to 3 mm deep to the rib and aspirated. If no blood was obtained, the fluid was injected into the neurovascular sheath. All patients had sitting erect chest radiography in the recovery room and a repeated chest radiography on postoperative day 1 if there was any suggestion of pleural effusion.
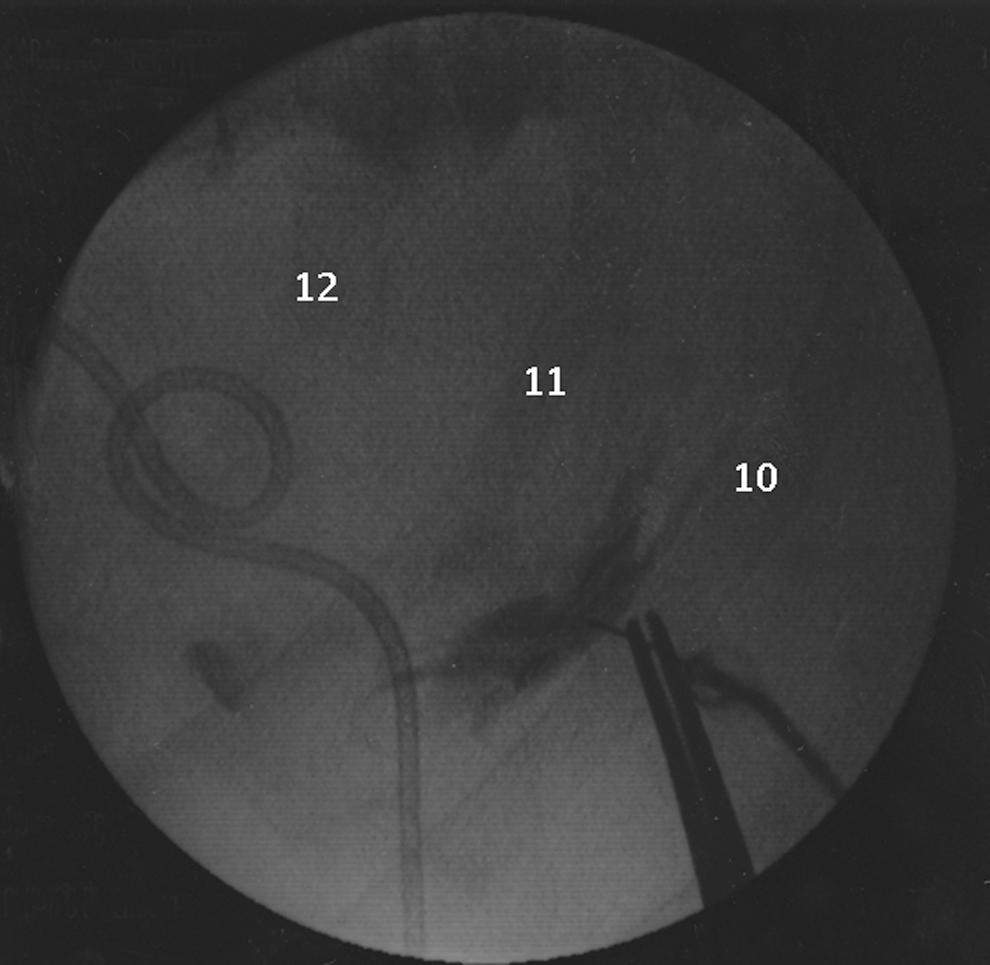
Technique of intercostal nerve block. A mixture of medication and Urografin® was used to demonstrate technique. The needle is held in a surgical clamp.
By protocol, all patients received patient-controlled anesthesia (PCA) administered through a bedside pump. Total analgesic use was recorded using standard conversions for morphine equivalents. The percutaneous nephrostomy tube was clamped first thing in the morning of postoperative day 1. If there was no significant flank pain or fever, the tube was capped and the patient was discharged home. Patients were followed up 1 week postoperatively and underwent radiography of the kidneys, ureters, and bladder (KUB) and nephroureterostomy tube removal. Patients with infected stones or radiolucent stones had a noncontrast low-dose CT scan.
Data collection
Data collection included both patient demographics and preoperative stone parameters. Length of stay and HRQL using the Postoperative Recovery Scale (a modification of the SF.36 that includes visual analog scale [VAS] score assessments of pain) 8 were also recorded. PCA narcotic use was recorded at 3, 6, 9, and 12 hours after receiving the intercostal nerve block. HRQL was recorded at 12 and 24 hours after the intercostal nerve block as well as at the follow-up appointment, 1 week after surgery. Fever was defined as documented T >38.5°C lasting more than 24 hours during the inpatient stay. Success and stone-free rates were determined from KUB examination conducted at the time of nephrostomy removal, 1 week after surgery, or with CT scans for patients with infected or radiolucent stones. Success was defined as sand or fragments ≤3 mm, with no need for auxiliary procedures such as second-look nephroscopy, URS, or SWL.
Sample size
Sample size was determined using pilot data from studies that compared PCNL performed with and without intercostal blocks. The calculation was performed using the Student t test to compare the milligrams of morphine equivalents used by patients during their inpatient stay. It was our belief that a 13-mg difference between the groups would represent a clinically meaningful difference in narcotic use. Calculations included a type I error (α) of 0.05 (two-tailed) and a type II error (β) of 0.2 (power of 80%). The projected enrollment was for a total sample of 62 patients without inflation because of dropout. In total, 70 patients were enrolled; however, 7 did not receive perioperative PCA and were thus excluded from the analysis. As a result, follow-up data were available for 63 patients (33 placebo and 30 bupivacaine).
Statistical analysis
The primary outcome was assessed using the Mantel-Haenszel chi-square function, as performed by the SPSS 16.0 statistical package on an intent-to-treat basis. Parametric parameters were compared with the Student t test. Nonparametric parameters were compared using the chi-square and the Mantel-Haenszel statistic or the Mann-Whitney test where appropriate. Statistically significant differences were considered at two-sided, P<0.05.
Results
Enrollment for this study began in May 2004 and ended in March 2009. A total of 70 patients were enrolled, and informed consent was obtained. The rate of enrollment was affected by other competing studies and our policy that patients can be enrolled in only one study at a time. Seven patients, however, did not receive PCA anesthesia postoperatively and were thus excluded from the analysis. Patients were randomized to receive either intercostal nerve blockade with either 20 mL 0.5% bupivacaine with epinephrine (30) or 20 mL placebo (saline) (33). All patients received the treatment to which they were assigned.
Baseline characteristics are presented in Table 1. Patients were similar in terms of age, sex, body mass index, initial stone area, and location of the nephrostomy access site (P>0.05 for all). Stones were an average of 28.3±12.3 mm2 in the placebo group and 30.1±15.7 mm2 in the bupivicaine group (P=0.416). In the placebo group, 20 (60.6%) of all punctures were above the 12th or 11th rib, whereas in the bupivicaine group, 16 (53.3%) of all punctures were supracostal (P=0.833). One patient in each group had a super-11th rib puncture.
N.B. Data are reported as N (%) or ±standard deviation where appropriate.
BMI=body mass index; max=maximum.
Within the first 3 to 6 hours after surgery, narcotic use was significantly less in the patients receiving intercostal nerve blockade with 0.5% bupivacaine (P=0.034 and 0.096, respectively, Table 2). Narcotic use, however, was not significantly reduced over the entire hospital stay (Fig. 2). Narcotic use in the placebo group was 59.3±35.2 vs 58.3±31.6 morphine equivalents (P=0.908). Similarly, length of stay was not found to be significantly different between either group (P=0.441). HRQL was improved both in the early and late postoperative periods in the group receiving intercostal blockade with 0.5% bupivacaine (P=0.034, Fig. 3).
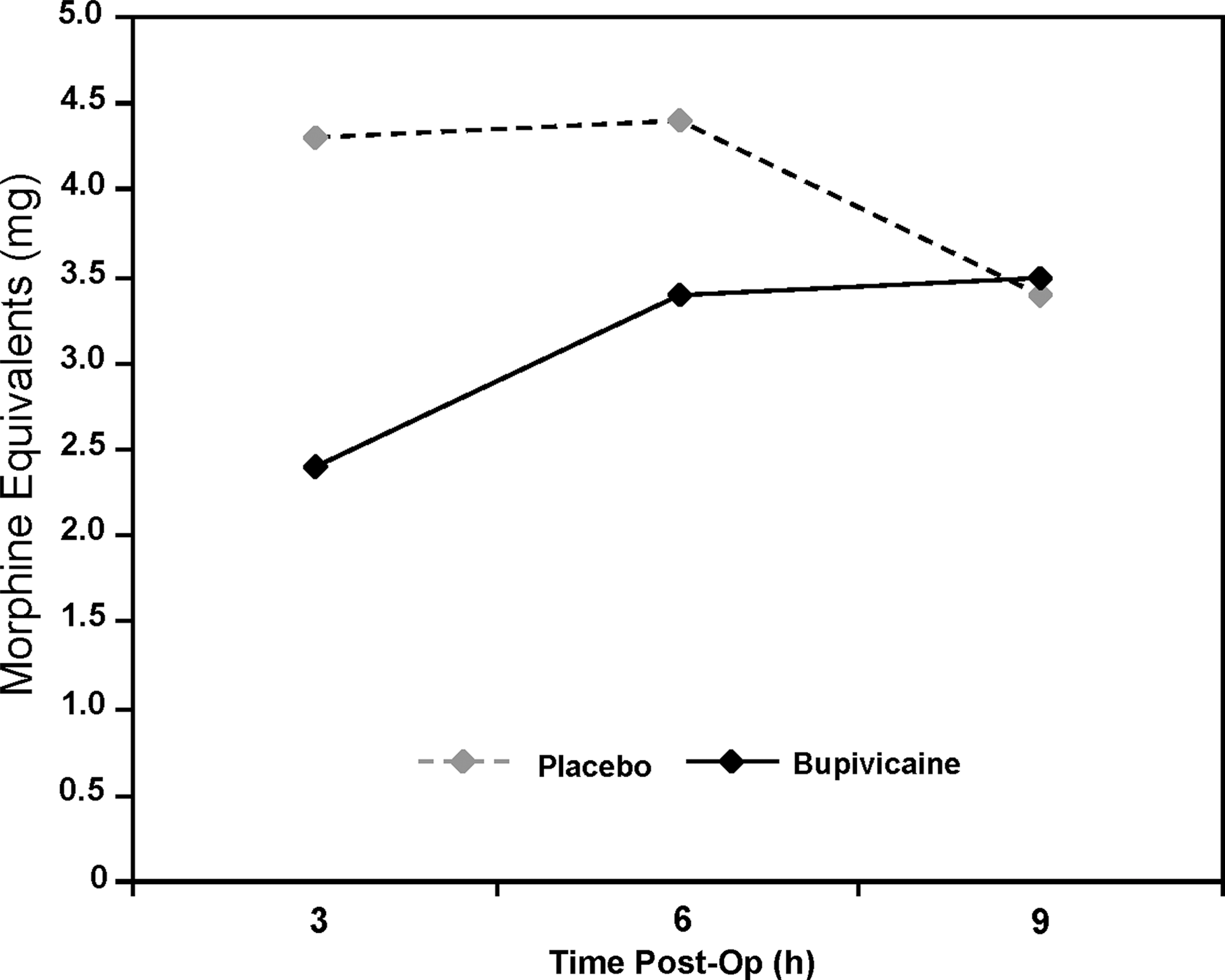
Postoperative narcotic use.
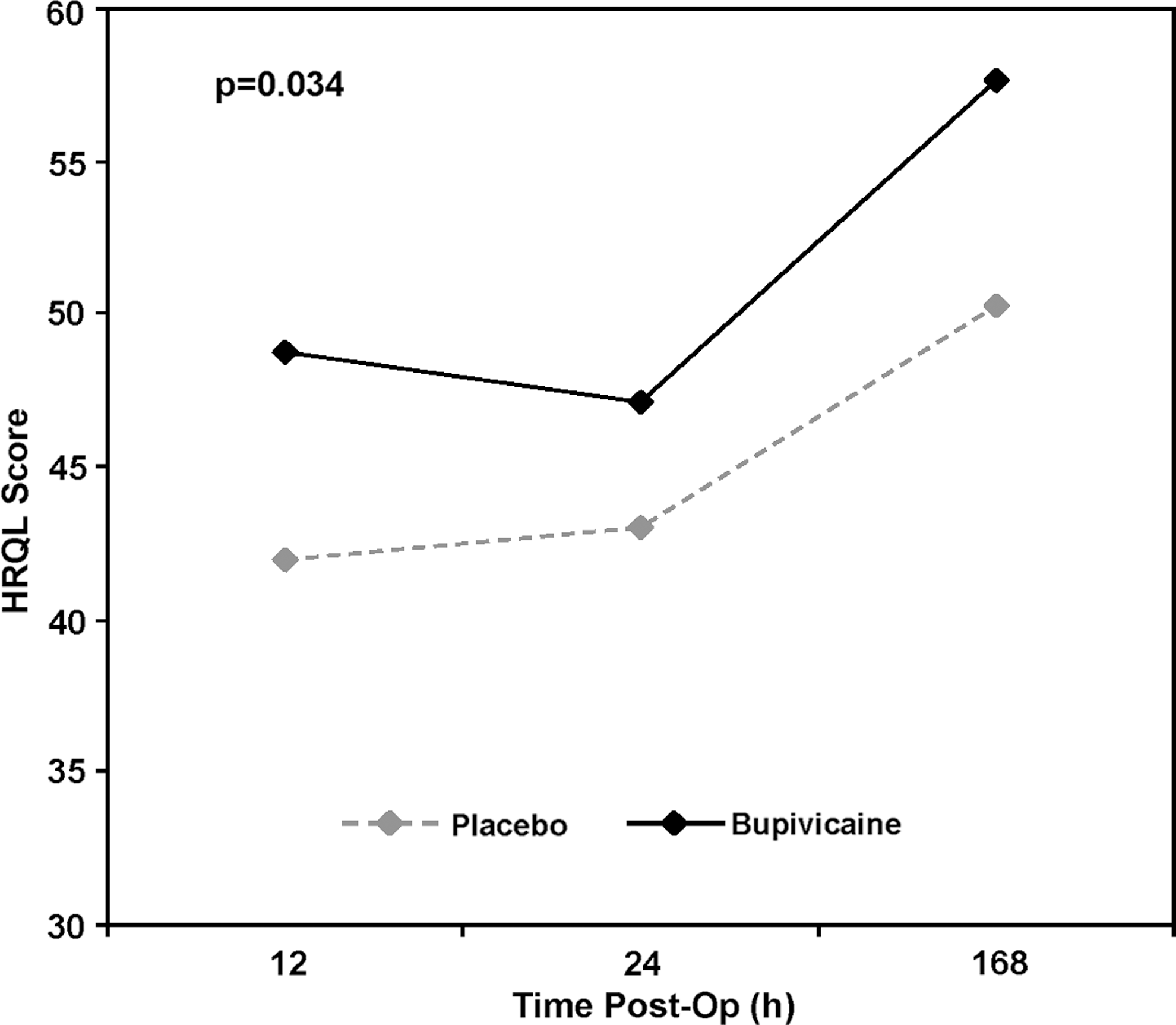
Postoperative health-related quality of life (HRQL).
Data are presented as mean±standard deviation or N (%), where applicable.
There were no transfusions in either group. In addition, no patients needed placement of a larger-caliber nephrostomy catheter because of intraoperative complications such as a large perforation of the collecting system or bleeding. There were no complications that could be attributed to the intercostal nerve blocks. Three (9.1%) patients in the placebo group and two (6.7%) patients in the bupivacaine group were found to have small pleural effusions on tpostoperative chest radiography. The majority of these occurred in patients with supracostal (4) as opposed to infracostal access (1); however, this did not reach statistical significance (P=0.282). Only two patients had tracts above the 11th rib. Both of these had small pleural effusions. No patients needed chest drainage, and all effusions resolved with conservative management. Two patients in the placebo group experienced a fever of >38.5°C lasting more than 24 hours.
Discussion
PCNL has almost entirely replaced open surgical techniques in the treatment of patients with large and complex renal calculi. Although less morbid, pain associated with the procedure, however, is of multifactorial etiology and may be significant in some patients. The goals of perioperative pain control should balance the often competing goals of effective analgesia with minimal narcotic use. These considerations are important because of concerns with patient safety, including the prevention of cardiac, gastrointestinal, and ventilatory complications. To that end, our study indicates that intercostal nerve blockade with bupivacaine reduces morphine use within the first 3 to 6 hours after surgery and improves HRQL.
Several options are available to improve perioperative analgesia. It is common practice in other settings to infiltrate the surgical site with local anesthetics in an effort to augment pain control; however, the utility of this practice in PCNL has been questioned. 9 A novel alternative that has shown some promise is the infiltration of the renal capsule and parenchyma before tract dilation. 10 It must be cautioned, however, that the efficacy of this technique has not been assessed in a randomized controlled trial, and this has likely slowed widespread application of the principle. More widely applied techniques include both interpleural blocks and tract infiltration with local anesthetic. The first report of interpleural block for PCNL was made in 1990 by Trivedi and associates. 11 This group reported on four patients who had undergone blockade with 30 mL bupivacaine 0.5% under fluoroscopic guidance. They found that the mean duration of pain relief was approximately 10 hours. Similarly, Saied and colleagues 12 found that interpleural block with bupivacaine provided superior postoperative pain relief to meperidine and diazepam. This type of indirect block relies on diffusion of the local anesthetic solution through the parietal pleura and has the disadvantage of risking lung injury when the space is identified by negative pressure aspiration and during insertion of the catheter. In addition, the block is often performed high on the flank and may be outside the surgical field. 12
Overcoming some of these obstacles, Ugras and coworkers 13 used a more direct approach and found that deep infiltration of the skin, tract, and renal puncture site provided similar benefits to the interpleural technique. In a blinded study of 34 well-matched patients, 30 mL of ropivacaine 0.02% led to improvements in VAS pain scores 6 hours after surgery as well as time to first analgesic demand and total analgesic requirements. 13 Similarly, in a blinded study of 40 well-matched patients, Jonnavithula and colleagues 14 found that peritubular infiltration with 20 mL of bupivacaine 0.25% led to improved VAS scores within the first 24 hours after surgery as well as less tramadol use.
The differences in mode of delivery and type of anesthetic agent used in these reports indicate that there may be several modes of regional anesthetic that are effective at reducing pain in the early postoperative period. Aravantinos and associates 15 recently reported on a prospective cohort of 51 patients undergoing PCNL under epidural analgesia followed by peritubular infiltration with lidocaine to facilitate tract puncture and dilation. They found that under a multimodal analgesia regime, the procedure was well tolerated and suggested that the majority of the pain associated with PCNL was because of dilation of the renal capsule and parenchymal tract.
Our study appears to be the first to directly assess the use of direct blockade of intercostal nerves after PCNL. This approach has significant precedent because intercostal nerve blockade is well established in other disciplines, such as chronic pain, thoracic surgery, etc. 6,16 The approach is fast and easy to learn because the nerves travel in neurovascular bundles below the ribs; however, there remains no “gold standard” method of delivery. We thus describe a technique using both palpation of bony landmarks and fluoroscopy to aid delivery. Importantly, no complications were attributable to the intercostal blocks in our series, indicating that the procedure is safe and easy to perform. Although intercostal block can result in pneumothorax, the incidence is low. Two large series reported an incidence of 1.4% 17 and 0.073%. 18 Pneumothorax or any complications attributable to the intercostal block did not develop in any patients in our study.
Limitations to our study include the fact that we included patients receiving both supra- and infracostal access tracts. It is likely that tracts above the 12th rib would be more uncomfortable for the patient and lead to increased narcotic use. Also, although not significantly different, there was a trend toward decreased success and stone-free rates in the group receiving nerve blocks with bupivacaine. It is possible that symptomatic residual fragments could have accounted for additional narcotic use, masking some of the difference between groups. The time frame of the study, however, was likely too short for this to be a factor, and the ureter was protected with the nephroureterostomy tube.
Several important questions were not assessed in our study. First, despite the intercostal blocks, patients in both groups still had significant postoperative narcotic use, suggesting that at least part of the pain after PCNL may be from deeper nerves supplying the diaphragm, from the tract through the renal parenchyma and capsule or from fluid extravasation, and other undefined causes. Combining intercostal nerve blockade with tract infiltration may result in enhanced analgesia. In keeping with its pharmacokinetic profile, the benefit of bupivacaine lasted for only 6 to 9 hours after instillation, with a relatively small difference in narcotic use. Despite this, patients with bupivacaine intercostal blockade exhibited a more dramatic improvement in overall HRQL. Nonetheless, longer-acting agents would be likely to provide further benefit and should be evaluated. Finally, the role of intercostal nerve block after PCNL in patients without a nephrostomy tube remains undefined.
Conclusion
Our study indicates that intercostal nerve blockade with bupivacaine reduces morphine use and improves HRQL in the immediate postoperative period; however, as expected, the effectiveness of bupivacaine disappears within 12 to 24 hours of surgery, after which narcotic use and HRQL scores become indistinguishable. Intercostal nerve blocks are an easy, safe, and inexpensive method to optimize immediate analgesia after PCNL and may facilitate the conversion to an outpatient procedure.
Footnotes
Disclosure Statement
No competing financial interests exist.